접수일 : 2014 년 9 월 15 일 , 게재승인일 : 2014 년 11 월 15 일 책임저자 : 김상준 , 서울시 강남구 일원동 50
135-710, 성균관대학교 삼성서울병원 재활의학교실
Tel: 02-3410-6069, Fax: 02-3410-0052 E-mail: [email protected]
요추 신경근병증 환자에서 추간판 탈출 정도와 임상 증상 및 이학적 이상 소견과의 정량적 분석
성균관대학교 삼성서울병원 재활의학교실
박종욱ㆍ황지혜ㆍ권정이ㆍ김상준
Quantitative Analysis of Disc Herniation Related to the Clinical Symptoms and Physical Findings in Patients with Lumbar Radiculopathy
Jong Wook Park, M.D., Ji Hye Hwang, M.D., Ph.D., Jeong-Yi Kwon, M.D., Ph.D. and Sang Jun Kim, M.D., Ph.D.
Department of Physical Medicine and Rehabilitation, Samsung Medical Center, Seoul, Korea
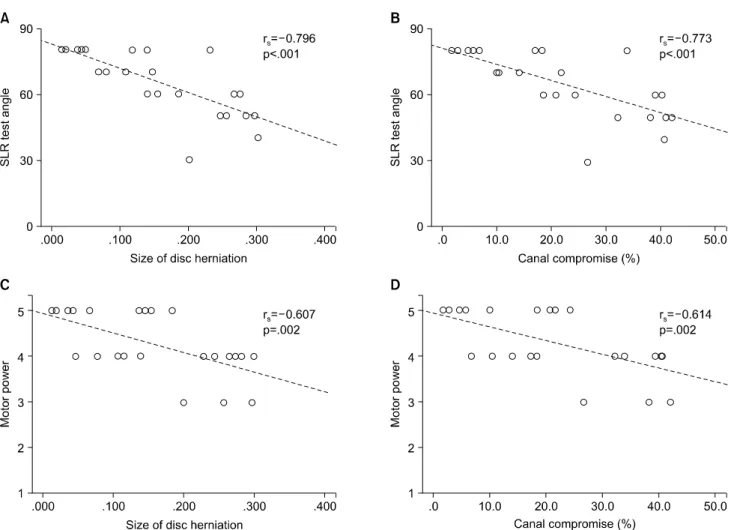
Objective: To identify the relationship of the quantitative size of disc herniation and canal compromise with the clin- ical symptoms and physical findings. Method: Twenty-four patients, who were diagnosed as having a single-level lum- bar radiculopathy caused by intervertebral disc herniation, were retrospectively evaluated for this study. The clinical symptoms included the presence of accompanying back pain and pain intensity expressed as a numeric rating scale score and physical examinations consisted of Dejerine’s tri- ad, straight-leg raise (SLR) test, slump test, Kemp’s test, and evaluation of motor and sensory involvement. The size of disc herniation and canal compromise (%) were calcu- lated by the quantitative image analysis of T2-weighted axial images. Results: The size of disc herniation showed a sig- nificant correlation with the SLR test (p<.001) and motor power grade (p=.002). The canal compromise also showed a significant correlation with the SLR test (p<.001) and mo- tor power grade (p=.002). Other variables did not show any correlation with the size of disc herniation and canal com- promise. Conclusion: Quantitative size of disc herniation and canal compromise were correlated with motor weak- ness and SLR angles in patients with lumbar radiculopathy.
(Clinical Pain 2014;13:84-93)
Key Words: Lumbar radiculopathy, Disc herniation, Canal com- promise, Straight-leg raise test, Motor weakness
INTRODUCTION
Lumbar intervertebral disc herniation is a common dis- order, and it can cause clinical symptoms including radicul- opathy, depending on the nerve root involvement. There are specific clinical symptoms suggestive of lumbar disc herniation, such as radiating pain, decreased sensation, and motor weakness. Many physical examinations are usually performed in the clinics to diagnose disc herniation, and computed tomography (CT) or magnetic resonance imaging (MRI) is performed to confirm the diagnosis.
Clinical information and physical examinations are im- portant for diagnosing herniated discs. Sciatica has high sensitivity and specificity, but its positive predictive value is low.
1The straight-leg raise (SLR) test shows high sensi- tivity with widely varying specificity in detecting lumbar disc herniation
2-4and nerve compression.
5,6According to a systemic review, the SLR test showed a sensitivity of 0.91 but a specificity of 0.26, thus yielding a pooled diagnostic odds ratio of 3.74.
7The slump test showed 100% sensi- tivity and 83% specificity in diagnosing mid-lumbar radi- culopathy,
8but its sensitivity and specificity in diagnosing lumbosacral radiculopathy has not yet been investigated.
Kemp’s test is performed for establishing the diagnosis of lumbar disc herniation or spinal stenosis, and it was pos- itive in 53% of patients with disc herniation.
9Motor and dermatomal sensory tests are always performed to delineate the level of disc involvement and to measure the severity.
Motor and sensory tests have shown a greater than 70%
positive predictive value in diagnosing lower lumbar disc herniation, but they have limited value in cases of disc protrusion.
10Herniated intervertebral discs can be classified into sev-
eral categories according to the severity of the herniation
expressed as semi-quantitative indices; bulging, focal pro-
trusion, extrusion, and sequestration. Disc extrusion and se-
questration tend to compress the nerve root, thus inducing greater weakness and sensory changes compared to disc bulging or protrusion.
11,12A migrated herniated nucleus pulposus is an important risk factor for motor deficits in lumbar disc herniation, which can be improved by surgical treatment.
13,14A previous study also demonstrated that pa- tients treated with surgery had larger disc herniation areas than patients in the nonoperative group.
15However, with respect to the natural course of the injury, the further the herniated disc migrates, the greater the decrease in size of the herniation because of lack of the nutritional supply.
16Therefore, it will be useful to know the severity of lumbar disc herniation for assessing the natural progression and for decision making regarding the treatment, although radio- logic and clinical diagnoses do not generally overlap.
17,18The direction of disc herniation can be classified into central, paramedian, lateral, and far lateral types. The direc- tion of herniation is important with respect to symptom development.
19,20Paramedian disc herniation can affect the nerve root as the herniated disc descends in the lateral re- cess, just before the nerve root enters the neural foramen.
Conversely, far lateral herniation can affect the nerve root as the nerve root exits the neural foramen, and central her- niation can affect any part of the cauda equine depending on the level. Therefore, symptoms can be different for her- niation at the same level, depending on the direction of herniation.
Magnetic resonance imaging (MRI), CT, and disco- graphy can demonstrate the severity and direction of disc herniation. However, MRI and CT are expensive tests, and discography is an invasive procedure, and hence these imaging techniques are performed only in selected cases.
If we can identify the relationship of the severity of disc herniation with clinical symptoms, physical findings, or a combination of both, it will assist in predicting the natural course of disc herniation and in selecting the appropriate treatment before imaging studies are performed. According to several studies, clinical symptoms and physical findings might predict nerve root compression on MRI through mul- tivariate logistic regression analysis.
4,11,21Contrary to nerve root compression, it is generally accepted that the severity of disc herniation expressed as semi-quantitative indices is not related to the clinical symptoms and physical findings, and there are many asymptomatic people who have lumbar disc protrusion and extrusion.
22Considering that the quanti-
tative analysis of spinal canal compromise can predict the surgical trend,
15clinical symptoms and physical findings can be related to the quantitative canal compromise rather than to the semi-quantitative indices of disc herniation.
However, there has been no study to identify the relation- ship of the quantitative canal compromise with the clinical symptoms and physical findings.
Therefore, the aim of this study was to identify the rela- tionship of the quantitative canal compromise with the clin- ical symptoms and physical findings.
PATIENTS AND METHODS
This is a retrospective cross-sectional study performed through a chart review. Among the patients who visited the outpatient department of the spine center at the Now Hospital from December 2009 to December 2010, 24 pa- tients, who were diagnosed as having a single-level lumbar radiculopathy caused by intervertebral disc herniation, were selected. The diagnosis of lumbar radiculopathy was based on clinical symptoms, electromyography (EMG), and MRI findings. Clinical symptoms included motor weakness, sen- sory disturbance including paresthesia and hypesthesia, or unilateral radiation to unilateral lower extremities with or without low back pain. Lumbar radiculopathy was diag- nosed when there were clinical symptoms to a myotomal or dermatomal level or the involved level confirmed by EMG matched the level of disc herniation on MRI. Axial MRI image is done with 4 mm thick slices. The involved level confirmed by EMG was determined when the sensory nerve conduction study was normal and abnormal sponta- neous activities were observed in the muscles based on the myotomal chart used in a previous article.
23The inclusion criteria were as follows: 1) radiating pain that started within the last three month; 2) a single-level of disc herniation without spinal stenosis or facet joint hy- pertrophy on MRI; 3) no previous history of lumbar sur- gery; 4) no history of interventional procedure including epidural steroid injections after the symptom onset. Patients who did not meet any of these criteria were excluded from our study.
The clinical symptoms were categorized based on the
presence of accompanying back pain, and pain intensity
was expressed as a numeric rating scale (NRS) score (0 to
10 points). Physical examinations were performed by an
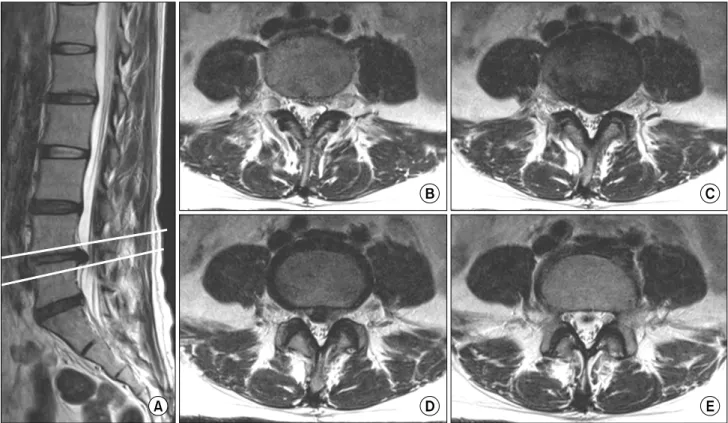
Fig. 1. Based on the sagittal view (A), several T2-weighted axial images were selected starting from the image cut (B) just above the upper margin of herniated disc material to the image cut (E) just below the lower margin, (C), (D) selected axial images between upper and lower margin of herniated disc.
expert physician who had an experience of examining more than 10,000 cases with lumbar radiculopathy. The physical examinations consisted of the following: 1) Dejerine’s tri- ad; 2) SLR test; 3) Slump test; 4) Kemp’s test; 5) Evaluation of motor involvement; and 6) Evaluation of sen- sory involvement. The Dejerine’s triad was positive when the pain became worse during coughing, sneezing, or Valsalva maneuver. The Kemp’s test was considered to be positive when the pain radiated down to the side towards which the patient was bending, which meant there was lumbar intervertebral disc involvement.
9The slump test was performed with the patient seated and the knee ex- tended with the neck in flexion, and this test was regarded as positive when the patient complained of pain.
8The SLR test was performed in a supine position, with the knee ex- tended in the same manner as performed in a previous study.
2Motor involvement was evaluated based on the muscle power corresponding to the myotomal level same as the level of disc herniation, and it was graded on a 0∼5 scale based on the Medical Research Council War
Memorandum. Sensory involvement was scored as 0 or 1, based on the presence of hypesthesia or paresthesia in the corresponding dermatome.
Lumbar MRI findings were interpreted and analyzed by an experienced radiologist who had interpreted more than 5,000 MRI findings of patients with disc herniation. For preventing bias, the radiologist was blinded to the in- formation about clinical symptoms and physical findings.
The severity of disc herniation was classified as bulging, protrusion, extrusion, or sequestration according to the scoring criteria used in a previous study,
24and the direction of the herniation was classified as central and lateral. This classification has already shown substantial intra- and in- ter-reader agreement in a previous study.
25The size of the disc herniation was calculated by the
quantitative image analysis. Based on the sagittal view,
several T2-weighted axial images were selected starting
from the image cut just above the upper margin of herni-
ated disc material to the image cut just below the lower
margin (Fig. 1). These axial cuts were captured as “.tiff”
Fig. 2. The size of canal cross-section area (A) and disc herniation area (B) in axial cuts were measured through the polygon selection of the NIH ImageJ software (dotted lines). The canal compromise (%) was calculated by dividing the disc herniation area by the canal cross-sectional area.
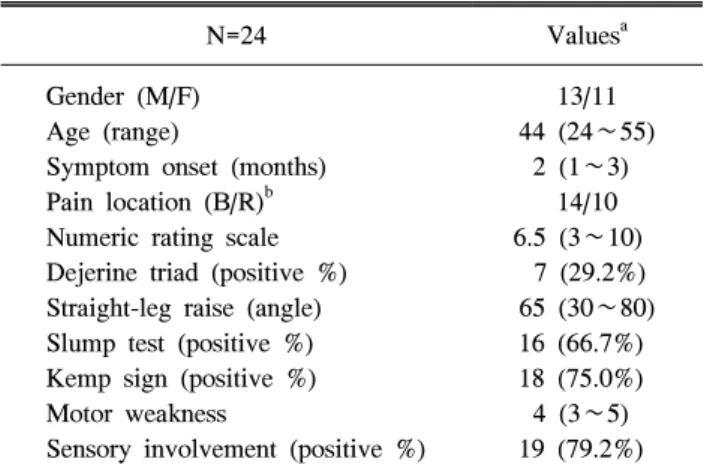
Table 1. Clinical Symptoms and Physical Findings of the Patients with Lumbar Herniated Intervertebral Disc
N=24 Values
aGender (M/F) 13/11
Age (range) 44 (24∼55)
Symptom onset (months) 2 (1∼3)
Pain location (B/R)
b14/10
Numeric rating scale 6.5 (3∼10)
Dejerine triad (positive %) 7 (29.2%) Straight-leg raise (angle) 65 (30∼80) Slump test (positive %) 16 (66.7%) Kemp sign (positive %) 18 (75.0%)
Motor weakness 4 (3∼5)
Sensory involvement (positive %) 19 (79.2%)
a
Values: Values are the number of patients or median (minimum value∼maximum value).
bPain location (B/R): Pain site is clas- sified into pain radiating to lower leg with low back pain (B) or without low back pain (R).
figure files. The size of disc herniation area and canal cross-section area in each cut were measured through the polygon selection of the NIH ImageJ software (version 1.47 for 32-bit Windows) and summated (Fig. 2). Then, the canal compromise (%) was calculated as the total size of disc herniation divided by the total canal cross-section area and multiplied by 100. The method for measurements was described in detail in a previous article.
15To determine the correlation between the severity and size of disc herniation, clinical symptoms and physical findings, Spearman correlation tests were performed using SPSS, version 12.0 (SPSS Inc., Illinois). To check the dif- ference of the severity and size of disc herniation according to the gender, Mann-Whitney U test was conducted. p-val- ues less than 0.05 were considered significant.
RESULTS
The median age of 24 patients (13 men and 11 women) was 44 years, and the median time interval from symptom onset to physical examination was 2 months. Fourteen pa- tients complained of radiating pain to the lower extremity without back pain, and 10 patients complained of radiating pain to the lower extremity with back pain. The pain start- ed at a median value of 65 degrees during the SLR test.
Data about demography and physical findings are presented
in Table 1.
Magnetic resonance images showed L5/S1 disc hernia-
tion in 17 patients, L4/L5 disc herniation in 6 patients, and
L3/L4 disc herniation in 1 patient. Twelve patients (50%)
had central disc herniation, and 12 (50%) had lateral
herniation. Disc bulging occurred in 4 patients, disc pro-
trusion in 10 patients, disc extrusion in 7 patients, and disc
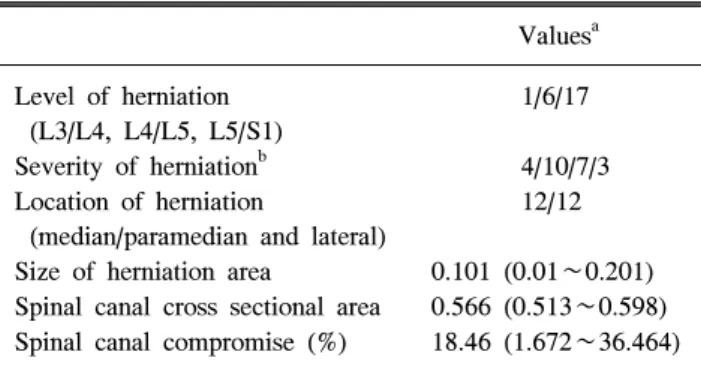
Table 2. Characteristics of Disc Herniation in Lumbar Spine Magnetic Resonance Imaging Study
Values
aLevel of herniation
(L3/L4, L4/L5, L5/S1)
1/6/17
Severity of herniation
b4/10/7/3
Location of herniation
(median/paramedian and lateral)
12/12 Size of herniation area 0.101 (0.01∼0.201) Spinal canal cross sectional area 0.566 (0.513∼0.598) Spinal canal compromise (%) 18.46 (1.672∼36.464)
a