대한소화기학회지 2008;52:9-15
접수: 2008년 1월 12일, 승인: 2008년 4월 29일
연락처: 김경모, 138-736, 서울시 송파구 풍납 2동 388-1 서울아산병원 소아과
Tel: (02) 3010-3380, Fax: (02) 473-3725 E-mail: kmkim@amc.seoul.kr
Correspondence to: Kyung Mo Kim, M.D.
Department of Pediatrics, Asan Medical Center, 388-1, Pung- nap 2-dong, Songpa-gu, Seoul 138-736, Korea
Tel: +82-2-3010-3380, Fax: +82-2-473-3725 E-mail: kmkim@amc.seoul.kr
위식도 역류가 의심되는 소아에서 Multichannel Intraluminal Impedance-pH Metry의 유용성
울산대학교 의과대학 서울아산병원 소아과학교실
이신혜ㆍ장주영ㆍ윤인자ㆍ김경모
Usefulness of Multichannel Intraluminal Impedance-pH Metry in Children with Suspected Gastroesophageal Reflux Disease
Shin Hye Lee, M.D., Joo Young Jang, M.D., In Ja Yoon, R.N., and Kyung Mo Kim, M.D.
Department of Pediatrics, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea
Background/Aims: pH monitoring of the esophagus has been considered as the gold standard for the measure-
ment of acid reflux. However, it has several limitations related to its inability to detect nonacid reflux. We con- ducted this study to characterize the proportion of acid and non-acid reflux events in children using pH-multi- channel intraluminal impedance (MII) monitoring and to determine the correlation of the symptom index with non-acid and acid reflux events. Methods: Seventy-five children, aged from 9 days to 12 years, underwent 24 hour pH-MII monitoring at Asan Medical Center from March 2006 to June 2007. We investigated the underlying disease and main problems related to gastroesophageal reflux (GER) of the patients, the number of acid and non- acid reflux, symptom index, symptom sensitivity index in pH monitoring only and pH-MII monitoring. Results:
While 2,247 reflux events were detected by MII, and only 967 reflux events were detected by pH probe alone.
The percentage of acid reflux was 43% (967) and that of non-acid was 57% (1,280). The non-acid reflux in- creased at postprandial time (p<0.001). The symptom index increased when measured by pH-MII (31.1%) com- pared with those by pH probe alone (8.2%) (p=0.003). Conclusions: This study suggests that significant number of GER include non-acid reflux which cannot be detected by pH probe alone, therefore combining pH with MII monitoring is a valuable diagnostic tool for diagnosing GER in children. (Korean J Gastroenterol 2008;52:9-
15)Key Words: Gastroesophageal reflux; pH monitoring; Multichannel intraluminal impedance monitoring; Acid re-
flux; Nonacid reflux
서 론
24시간 보행 식도 pH 검사는 식도 원위부에 pH 도자 (probe)를 위치하여 실제 산의 역류를 측정할 수 있어 과거
위식도역류질환(gastroesophageal reflux disase)의 진단에 표 준검사법으로 평가받아왔다.1 pH 검사 시 역류는 pH가 4 이 하의 산 역류(acid reflux)가 일정 시간 지속되는 경우로 정 의한다.2 식도 내부의 정상 pH는 5에서 7 사이이므로, pH 검
10 대한소화기학회지: 제52권 제1호, 2008
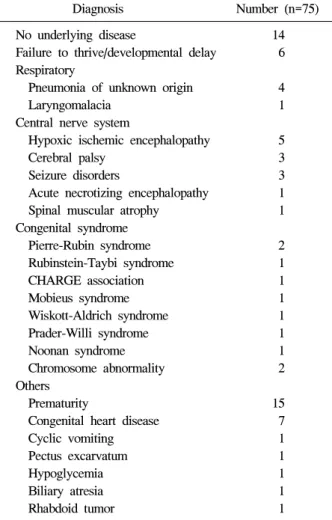
Table 1. Underlying Disease of 75 Patients with Suspected Gastroesophageal Reflux Disease
Diagnosis Number (n=75) No underlying disease 14 Failure to thrive/developmental delay 6 Respiratory
Pneumonia of unknown origin 4
Laryngomalacia 1
Central nerve system
Hypoxic ischemic encephalopathy 5 Cerebral palsy 3 Seizure disorders 3 Acute necrotizing encephalopathy 1 Spinal muscular atrophy 1 Congenital syndrome
Pierre-Rubin syndrome 2 Rubinstein-Taybi syndrome 1 CHARGE association 1 Mobieus syndrome 1 Wiskott-Aldrich syndrome 1 Prader-Willi syndrome 1 Noonan syndrome 1 Chromosome abnormality 2 Others
Prematurity 15
Congenital heart disease 7 Cyclic vomiting 1 Pectus excarvatum 1
Hypoglycemia 1
Biliary atresia 1 Rhabdoid tumor 1 CHARGE, coloboma, heart disease, atresia choanae, retared growth & development or CNS anomalies, genital anomalies
&/or hypogonadism, ear anomalies and/or deafness.
사로는 pH 4 이상의 비산 역류(non-acid reflux)는 측정할 수 없다.3,4 저자들의 소아를 대상으로 실시한 연구에서 위식도 역류(gastroesophageal reflux)는 주로 식후에 일어나는 것으 로 보고한 바 있는데,1 위내 음식물들이 중화된 식후 시간에 일어나는 역류는 수소 이온 농도만 단순히 측정하는 pH 검 사로는 식후 역류(postprandial reflux)를 완벽하게 측정할 수 없다. 특히, 자주 모유 혹은 분유를 먹어 위산이 지속적으로 중화되는 영유아에서는 이에 의한 역류가 산도 검사로는 정 확히 측정될 수 없다.5-7 뿐만 아니라 제산제 치료에도 반응 이 없거나 비전형적인 증상을 보이는 경우에는 비산 역류에 의하여 민감도가 낮아지고, 치료 반응 정도를 평가하기 위 해 검사하는 경우에는 검사 전 제산제 복용을 중단하게 되 면 오히려 위산 분비가 더 증가되어 정확한 결과를 얻을 수 없다.2,8-12
최근 개발된 다채널 강내 임피던스-pH 검사(multichannel intraluminal impedance-pH metry, MII-pH)는 산 역류와 비산 역류를 모두 측정할 수 있어 위식도역류 및 식도 기능평가 에 새로운 검사법으로 대두되고 있다. 임피던스는 전압에 대한 전류의 비로 정의하며, 이 검사는 식도강 내 음식물이 유입될 때 여러 개로 구성된 전극 중에서 각각 두 전극 사 이에 발생한 전류에 대한 저항변화를 측정한다. 공기의 전 기전도율은 영에 가까우므로 임피던스는 증가되고, 침, 음 식물 등은 높은 전기전도율을 보이므로 임피던스는 감소하 는 원리를 이용하여 역류뿐만 아니라 역류된 물질의 성상도 알아낼 수 있다. 그리고 한 카테터 내에 여러 채널이 정렬되 어 있어 식괴의 이동 방향 및 역류의 높이도 알 수 있다.13-15 저자들은 이러한 장점을 지니고 있는 MII-pH 검사를 이 용하여 소아에서 pH probe만으로는 측정할 수 없는 비산 역 류가 차지하는 비율을 알아보고, 비산 역류의 중요성을 알 아보기 위하여 산 역류 및 비산 역류와 증상지수(symptom index)와의 관계에 대해 알아보고자 하였다.
대상 및 방법
1. 대상
2006년 3월부터 2007년 6월까지 18개월간 서울아산병원 소아과에서 위식도역류질환을 의심하여 24시간 MII-pH moni- toring (Sandhill Scientific, Inc., USA) 검사를 시행한 75명을 대상으로 후향으로 조사하였다.
24시간 MII-pH 검사를 시행한 총 75명의 환아들 중 남아 45명, 여아 30명이었고, 이들의 평균 연령은 19개월(범위 9 일-12세)이었다. 대상 환아들의 기저 질환에 대해 조사하였 고, 이 중 심폐계질환(13명), 신경계질환(13명), 선천 증후군 (10명), 미숙아(15명), 성장발달지연(6명), 그 외(4명)이었고,
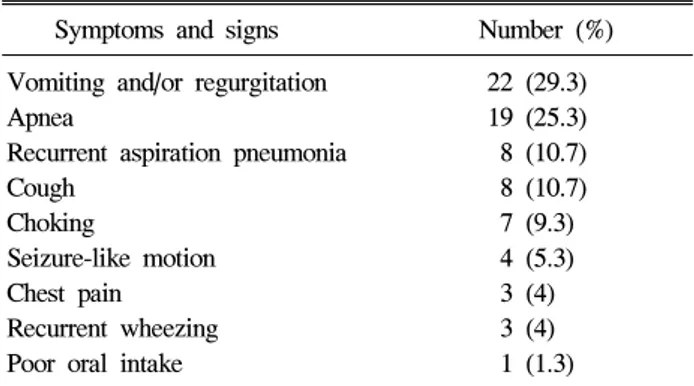
기저 질환 없는 경우는 14명이었다(Table 1). 대상 환아들의 증상은 다음과 같았다. 구토 및 역류(23명, 29%), 무호흡 및 산소포화도 저하(19명, 25%), 흡인 폐렴(8명, 11%), 기침(8 명, 11%), 질식(7명, 10%), 발작 유사 증상(4명, 5%), 흉통(3 명, 4%), 반복 천명(3명, 4%), 식욕부진(1명, 1%)이 있었다 (Table 2).
2. 검사기구
6개의 임피던스 채널(impedance channel, 3, 4.5, 6, 7.5, 9, 10.5 cm, Sandhill Scientific)과 1개의 pH 감지기(sensor)가 원 위부 6번째 채널 내에 존재하는 도자를 이용하여 검사를 시 행하였다.15 pH 감지기는 식도내압검사를 시행하여 식도하 부괄약근(lower esophageal sphincter, LES)의 상방 3-5 cm 부 위에 위치하도록 하였다.
이신혜 외 3인. 위식도 역류가 의심되는 소아에서 Multichannel Intraluminal Impedance-pH Metry의 유용성 11
Table 2. Major Symptoms and Signs of 75 Patients Suggesting Gastroesophageal Reflux
Symptoms and signs Number (%) Vomiting and/or regurgitation 22 (29.3)
Apnea 19 (25.3)
Recurrent aspiration pneumonia 8 (10.7)
Cough 8 (10.7)
Choking 7 (9.3)
Seizure-like motion 4 (5.3)
Chest pain 3 (4)
Recurrent wheezing 3 (4) Poor oral intake 1 (1.3)
Fig. 1. Relationship of detected multichannel intraluminal impe- dance reflux events versus pH reflux events.
3. 전처치 및 환자 교육
위장운동촉진제, 제산제 및 양성자펌프억제제(Proton Pump Inhibitor, PPI)는 검사 시작 전에 각각 48시간, 72시간 및 7일 간 중단하도록 교육하였다. 보호자들은 증상이 있을 때 버 튼을 누르고 서면으로 기록하도록 하였으며 자세와 수유 여 부, 특정 사건들도 함께 기록하도록 하였다.
4. 결과치 분석
검사 결과의 분석은 BioVIEW analysis software (Sandhill Scientific)를 사용하여 시행하였다. 산 역류(acid reflux)는 pH
<4 이하로 5초 이상 유지되는 역류로 정하였고, 총 역류의 횟수와 산 역류(acid reflux) 및 비산 역류(nonacid reflux)의 횟수를 총 검사시간과 식후 2시간(postprandial time)으로 구 분하여 조사하였다. 역류 물질의 성상과 검사 중 발생한 증 상의 빈도를 확인하고 역류와의 연관성을 Symptom Index (SI)와 Symptom Sensitivity Index (SSI)를 이용하여 평가하였 다. 역류와의 연관된 증상은 역류 발생 전후 5분 이내 발생 한 증상으로 정의하였고, 1분 이내 발생한 동일한 증상은 분석에서 제외하였다. SI는 증상 발현 시 역류 동반할 가능 성을 나타내며, SSI는 역류 발생 시 증상 발현될 가능성을 나타내며 다음과 같이 구한다.16,17
Symptom Index=No. of reflux-related symptom/total No. of symptom
Symptom Sensitivity Index=No. of reflux-related symptom/
total No. of reflux
보고된 문헌을 참고하여 SI>50%, SSI>10%인 경우를 이 상소견으로 판단하였다.16,17
대상 환아의 연령과 성별, 기저 질환, 위식도 역류와 관련 한 주증상을 조사하였다.
5. 통계 및 분석
통계 처리 및 데이터 분석은 SPSS version 12.0을 이용하 여 교차분석, 카이제곱 검정 및 Fisher의 정확 검정을 이용 하였고, p<0.05일 때 유의한 차이가 있는 것으로 해석하였 다.
결 과
1. 산 역류와 비산 역류의 빈도
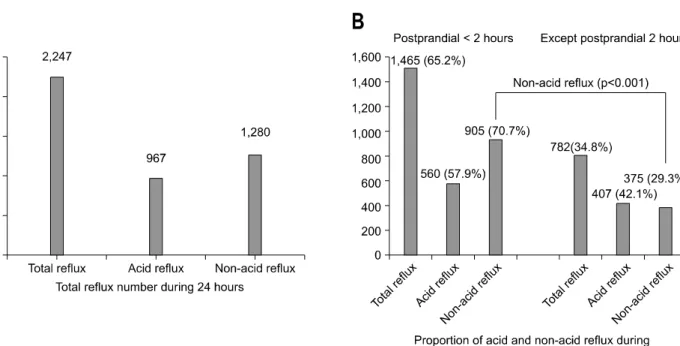
24시간 MII-pH monitoring 검사 시 총 2,247회의 역류가 측정되었고, 이 중 산 역류는 967회(43%), 비산 역류는 1,280회(57%)였다(Fig. 1). Fig. 1의 각 점들은 한 사람에게서 MII-pH와 pH 검사한 경우 측정된 역류 횟수를 나타낸다. 모 든 점들이 45도 대각선 선 위에 위치하는 것은 모든 사람에 게서 pH 도자만으로 검사하는 것보다 pH-MII로 병합하여 검사한 경우 더 많은 역류를 측정할 수 있다는 것을 시사한 다. 식후 2시간 이내 발생한 역류가 1,465회 측정되었고 이 는 총 역류의 65%를 차지하였고, 식후 역류 중 산 역류는 560회(38%), 비산 역류는 905회(62%)였다. 비산 역류는 식 후 2시간 이내가 70.7%를 차지하였고, 식후 2시간 이후는 29.3%로 감소하였다(Fig. 2).
2. 위식도역류와 증상과의 관계 분석
검사 중 총 374회의 증상이 기록되었고, 기침(32.1%)이 가 장 흔하였고, 그 외에 트림(20.1%), 역류(19.2%), 약물복용과 관련된 구토, 기침 등의 증상(16.3%), 산소포화도 저하 (8.8%), 통증(2.7%), 경련(0.8%) 등이었다. 역류와 증상과 연 관성을 평가하기 위해 SI, SSI를 구하고 SI>50%, SSI>10%
인 경우를 양성으로 간주하였다. 대상자 중 14명에서 24시
12 The Korean Journal of Gastroenterology: Vol. 52, No. 1, 2008
Fig. 2. (A) Total reflux number and proportion of acid and non-acid reflux events during 24 hours. (B) The number and proportion of acid and non-acid reflux events in length of time. The proportion of non-acid reflux decreases from 70.7% during 2 hours from the last meal to 29.3% beyond 2 hours postprandially.
Table 3. Number of Patients with Positive Symptom Indices
pH probe MII-pH p-value
No. patients with positive SI* (%) 5/61 (8.2) 19/61 (31.1) 0.003 No. patients with positive SSI† (%) 9/61 (14.7) 16/61 (26.2) 0.178 No. patients with positive SI and SSI (%) 2/61 (3.3) 8/61 (13.1) 0.095
* Symptom Index = No. of reflux-related symptom/total No. of symptom.
†Symptom Sensitivity Index = No. of reflux-related symptom/total No. of reflux.
간 검사 동안 증상 발생이 없었고, 나머지 61명 중 27명에서 SI가 0%였다. SI 50% 이상으로 양성인 경우는 19명이었고, 역류와 연관된 증상의 총 횟수는 109회(29.1%)였다. 그 증상 으로는 역류(8.3%), 트림(8.0%), 산소포화도 저하(3.5%), 통 증(2.7%), 기침(2.1%)이었다. pH 도자만으로 검사한 경우와 MII-pH 병합한 검사의 SI는 8.2%와 31.1%이었고(p=0.003), SSI는 14.7%와 26.2%였다(p=0.178) (Table 3).
고 찰
위식도역류란 위의 내용물이 하부식도괄약근을 지나 식 도 혹은 구강 내로 역류하는 것을 말하며, 1세 미만의 영아 에서 흔히 볼 수 있다.
영유아기의 위식도역류가 중요한 이유는 그 빈도가 흔하 고 또한 이에 의해서 발생하는 증상이 다양하다는 것에 있 다고 하겠다.18-21 역류 혹은 구토가 위식도역류의 가장 흔한
증상이며 이로 인해 구토의 양이 많으면 영아의 성장 장애 가 초래된다. 역류 식도염에 의해서 보채고, 때로는 먹으려 하지 않고, 빈혈이 관찰되기도 한다. 또한 호흡기 증상으로, 질식, 흡인 폐렴 등이 발생하고, 천식, 기관지폐이형성증, 반 복폐렴, 무호흡증에서 위식도역류의 빈도가 증가하는 것으 로 알려져 있다. 간혹 신경학적인 이상으로 오인되는 San- difer's 증후군을 보이기도 한다.18-21
소아 및 영유아에서는 전술한 바와 같이 발현된 증상에 의거하여 위식도역류질환에 대한 검사와 치료를 시행하게 된다. 북미소아소화기영양학회에서는 반복적인 구토 증상 과 체중증가불량, 자극과민, 심한 울부짖음, 수면장애, 수유 및 호흡 장애문제를 동반할 경우 진단 검사를 시행하도록 하고 있다.20,22 이번 연구에서 검사를 시행한 75명의 환아들 도 구토, 역류, 기침, 산소포화도 저하, 반복적인 폐렴, 천명, 흉통 등의 증상이 있었고, 이들 대부분이 위식도역류 의심 하에 제산제, 양성자펌프억제제 등을 복용하였으나 증상 호
Lee SH, et al. Usefulness of Multichannel Intraluminal Impedance-pH Metry in Children with Suspected GERD 13
전이 없었다. 뿐만 아니라 몇몇 환아들은 위식도역류질환 진단 후 위루술을 시행받았으나 증상 지속되어 검사 시행하 였다.
이전에 저자들이 pH 검사만으로 연구하여 식후에 산 역 류가 높은 것을 보고한 바가 있다.1 이번 연구에서는 그동안 표준검사로 알려진 pH monitoring으로 검사한 경우(967회) 보다 MII-pH monitoring 검사를 시행한 경우(2,247회) 더 많 은 역류를 측정할 수 있었고, 측정된 2,247회 역류 중 1,465 회 역류가 식후 2시간 이내 발생하였고, 이들 대부분이 비 산 역류였다(70.7%). Adria와 Judith 등에 의하면, 비산 역류 는 마지막 식사 시간에 가까울수록 더 많은 비중을 차지하 며 이는 특히, 더 자주 먹는, 더 어린 영아에서 그 비중이 더 높았다.3,6,13 여러 보고에서 기존의 제산 치료 등에 잘 반 응하지 않거나, 비특이적인 증상을 가진 위식도역류질환 등 은 비산 역류와 관계있다고 보고하고 있다. 그러므로 특히 소아에서는 기존의 표준검사로 알려진 pH monitoring 검사 로는 비산 역류를 측정할 수 없어 증상과 역류의 연관성을 정확히 밝힐 수 없다.23-27
증상과 역류의 연관성을 알아보기 위해 SI와 SSI를 이용 하였고 MII-pH 검사에서 각각 31.1%와 26.2%였다. 이는 Rosen과 Nurko의 연구에서 33%와 25%로 나온 것과 비슷하 였고, Adria와 Judith 등이 보고한 66.6%와 53.3%보다는 낮
았다.13,28 그러나 이번 연구에서 pH 검사만 한 경우의 SI와
SSI (8.2%, 14.7%)를 비교하면 MII-pH 병합한 경우 증상과 역류와 연관성을 더 잘 밝힐 수 있었다. 즉, Rosen과 Nurko 의 연구에서 언급한 바와 같이, 산 역류보다 비산 역류가 증 상 유발과 더 관계가 있기 때문에 MII-pH 병합 검사를 이용 하여 역류와 증상과의 임상적인 연관성을 더 잘 나타낼 수 있는 것이다.28
이 외에도 MII-pH 검사는 기존의 pH 검사의 제한점을 극 복할 수 있는 대체 검사로 대두되고 있다.29 앞에서 기술한 바와 같이 비산 역류를 측정할 수 있고, 제산제 치료 등에 반응하지 않는 위식도역류질환 진단 및 치료에 이용할 수 있다. 그리고 식도 내강에 위치시킨 도관의 여러 채널의 임 피던스 측정을 함으로써 역류의 높이, 방향, 성상, 속도 등 도 알 수 있어 위장관 기능의 생리, 병태생리를 알 수 있다.
그러나 소아에서는 검사 결과에 대한 정상 참고치가 아직 확립되어 있지 않으며, 검사 결과의 해석 및 분석 모두 완전 자동화되지 않고 각각의 결과를 직접 확인해야 하는 등 수 작업이 필요한 단점이 있다. 하지만 MII-pH 검사의 임상적 인 사용이 증가하고 있어 곧 소아의 정상 참고치도 밝혀질 것이며, 컴퓨터 프로그래밍의 발전으로 결과 해석 및 분석 모두 완전 자동화될 것으로 여겨진다.10,14,29
역류와 증상과의 연관성을 밝히기 위해 MII 검사와 위장 관 압력측정검사(manometry)나 수면검사(polysomnography)
와 같은 다른 검사들과도 병합하여 사용할 수 있다. 특히, 수면 검사를 병합하여 영유아의 무호흡, 천명 등 호흡기 증 상과 수면 장애 등이 역류와 연관관계 여부를 알아내는 데 유용하게 사용할 수 있다.14
결론으로, MII-pH 검사법을 이용하여 산 역류 및 비산 역 류를 보다 더 정확히 측정할 수 있고, 특히 비산 역류를 더 잘 측정함으로써 증상과의 연관성도 더 정확히 반영할 수 있고, 이런 환자에게 비산 역류를 치료하여 증상호전을 기 대할 수 있다. 그러므로 MII-pH 병합검사는 영유아 및 소아 에서 위식도역류 진단, 치료에 반응 없는 경우 및 비전형적 인 증상 보이는 경우 pH 검사보다 더 유용하며, 식도 및 위 장관 운동 및 질환에 대해 궁극적인 평가가 가능하게 될 것 이다.
요 약
목적: 위식도 역류 진단에 있어 식도 pH monitoring이 가 장 많이 이용되고 있다. 그러나 비산 역류를 찾아내기에는 민감도가 떨어져 그 한계점이 논란이 되고 있다. pH-Multi- channel Intraluminal Impedance (MII) 검사법을 이용하여 영 유아, 소아의 위식도 역류 가운데 산성 역류와 비산성 역류 의 비율을 밝히고, 이러한 역류 현상과 증상의 연관성 (symptom index)에 대해 알아보고자 하였다. 대상 및 방법:
2006년 3월에서 2007년 6월까지 18개월간 서울아산병원 소 아과에서 위식도역류질환을 의심하여 검사 의뢰된 총 75명 의 환아들을 대상으로 24시간 pH-MII monitoring 검사를 시 행하였다. pH monitoring만으로 검사한 경우와 pH-MII monitoring으로 검사한 경우 각각의 검사에서 산성 또는 비 산성 역류의 횟수와 symptom index (SI), symptom sensitivity index (SII)를 조사하였다. 결과: pH-MII monitoring 검사 시 2,247회의 역류가, pH monitoring만으로 검사하였을 경우 967회의 역류가 측정되었다. 이 중 산 역류는 43% (967), 비 산 역류는 57% (1,280)를 차지하였다. 그리고 비산 역류는 식후 시간에 가까울수록 더 많은 비중을 차지하였다(p
<0.001). 총 374회의 증상이 관찰되었고, SI는 24시간 pH- MII monitoring 검사(31.1%)가 pH monitoring만으로 검사 (8.2%)한 경우보다 더 높게 측정되었다. 결론: 위식도역류 중 비산 역류가 더 큰 비중을 차지하므로 24시간 pH-MII monitoring 검사가 영유아 및 소아에서 위식도역류질환 진단 에 pH monitoring 검사보다 더 유용하다.
색인단어: 위식도역류질환, 식도 pH 검사, 다채널 강내 임 피던스-pH 검사, 산 역류, 비산 역류
14 대한소화기학회지: 제52권 제1호, 2008
참고문헌
1. Kim KM, Shim JY, Hong SJ, Influence of feeding and state of alertness on the incidence of gastroesophageal reflux in children. J Korean Pediatr Soc 1997;40:1419-1426.
2. Mitchell DJ, McClure BG, Tubman TR. Simultaneous mon- itoring of gastric and oesophageal pH reveals limitations of conventional oesophageal pH monitoring in milk fed infants.
Arch Dis Child 2001;84:273-276.
3. Wenzl TG. Evaluation of gastroesophageal reflux events in children using multichannel intraluminal electrical impedance.
Am J Med 2003;115(suppl 3A):161S-165S.
4. Vandenplas Y, Belli D, Boige N, et al. A standardized proto- col for the methodology of esophageal pH monitoring and in- terpretation of the data for the diagnosis of gastroesophageal reflux. Society statement of a working group of the European Society of Pediatric Gastroenterology and Nutrition. J Pediatr Gastroenterol Nutr 1992;14:467-471.
5. Sifrim D, Holloway R, Silny J, Tack J, Lerut A, Janssens J.
Composition of the postprandial refluxate in patients with gastroesophageal reflux disease. Am J Gastroenterol 2001;96:
647-655.
6. Del Buono R, Wenzl TG, Ball G, Keady S, Thomson M.
Effect of Gaviscon Infant on gastro-oesophageal reflux in in- fants assessed by combined intraluminal impedance/pH. Arch Dis Child 2005;90:460-463.
7. Wenzl TG, Silny J, Schenke S, Peschgens T, Heimann G, Skopnik H. Gastroesophageal reflux and respiratory phenom- ena in infants: status of the intraluminal impedance technique.
J Pediatr Gastroenterol Nutr 1999;28:423-428.
8. Suys B, De Wolf D, Hauser B, Blecker U, Vandenplas Y.
Bradycardia and gastroesophageal reflux in term and preterm infants: is there any relation? J Pediatr Gastroenterol Nutr 1994;19:187-190.
9. Sutphen JL, Dillard VL. Effect of feeding volume on early postcibal gastroesophageal reflux in infants. J Pediatr Gastro- enterol Nutr 1988;7:185-188.
10. Skopnik H, Silny J, Heiber O, Schulz J, Rau G, Heimann G.
Gastroesophageal reflux in infants: evaluation of a new intra- luminal impedance technique. J Pediatr Gastroenterol Nutr 1996;23:591-598.
11. Malfroot A, Dab I. Pathophysiology and mechanisms of gas- troesophageal reflux in childhood asthma. Pediatr Pulmonol 1995;(suppl)11:55-56.
12. Han DH, Lee JS, Kim YD, et al. Usefulness of multichannel intraluminal impedance-pH metry in patients with suspected GERD presenting with typical or atypical symptoms. Korean
J Neurogastroenterol Motil 2006;12:25-30.
13. Condino AA, Sondheimer J, Pan Z, Gralla J, Perry D, O'Connor JA. Evaluation of infantile acid and nonacid gas- troesophageal reflux using combined pH monitoring and im- pedance measurement. J Pediatr Gastroenterol Nutr 2006;42:
16-21.
14. Wenzl TG. Investigating esophageal reflux with the intra- luminal impedance technique. J Pediatr Gastroenterol Nutr 2002;34:261-268.
15. Tutuian R, Vela MF, Shay SS, Castell DO. Multichannel in- traluminal impedance in esophageal function testing and gas- troesophageal reflux monitoring. J Clin Gastroenterol 2003;37:
206-215.
16. Wiener GJ, Richter JE, Copper JB, Wu WC, Castell DO. The symptom index: a clinically important parameter of ambula- tory 24-hour esophageal pH monitoring. Am J Gastroenterol 1988;83:358-361.
17. Breumelhof R, Smout AJ. The symptom sensitivity index: a valuable additional parameter in 24-hour esophageal pH recording. Am J Gastroenterol 1991;86:160-164.
18. Hong SJ, Shim JY, Kim BS, Park KY, Kim KM. Prevalence of gastroesophageal reflux in infants with recurrent wheezing.
J Asthma Allergy Clin Immunol 1999;19:576-583.
19. Vandenplas Y, Belli D, Benhamou P, et al. A critical apprais- al of current management practices for infant regurgitation-- recommendations of a working party. Eur J Pediatr 1997;156:
343-357.
20. Rudolph CD, Mazur LJ, Liptak GS, et al. Guidelines for evaluation and treatment of gastroesophageal reflux in infants and children: recommendations of the North American Society for Pediatric Gastroenterology and Nutrition. J Pediatr Gastroenterol Nutr 2001;32(suppl)2:S1-S31.
21. Vandenplas Y, Ashkenazi A, Belli D, et al. A proposition for the diagnosis and treatment of gastro-oesophageal reflux dis- ease in children: a report from a working group on gas- tro-oesophageal reflux disease. Working Group of the Euro- pean Society of Paediatric Gastro-enterology and Nutrition (ESPGAN). Eur J Pediatr 1993;152:704-711.
22. Corvaglia L, Ferlini M, Rotatori R, et al. Starch thickening of human milk is ineffective in reducing the gastroesophageal reflux in preterm infants: a crossover study using intraluminal impedance. J Pediatr 2006;148:265-268.
23. Bredenoord AJ, Weusten BL, Sifrim D, Timmer R, Smout AJ. Aerophagia, gastric, and supragastric belching: a study using intraluminal electrical impedance monitoring. Gut 2004;
53:1561-1565.
24. Vela MF, Tutuian R, Sifrim D, et al. Comparison of pH-me-
이신혜 외 3인. 위식도 역류가 의심되는 소아에서 Multichannel Intraluminal Impedance-pH Metry의 유용성 15
try versus combined multichannel intraluminal impedance and pH (MII-pH) for symptom association studies in symptomatic acid suppressed GERD patients. Gastroenterology 2004;124:
A524.
25. Tutuian R, Castell DO. Rumination documented by using combined multichannel intraluminal impedance and mano- metry. Clin Gastroenterol Hepatol 2004;2:340-343.
26. Vela MF, Camacho-Lobato L, Srinivasan R, Tutuian R, Katz PO, Castell DO. Simultaneous intraesophageal impedance and pH measurement of acid and nonacid gastroesophageal reflux:
effect of omeprazole. Gastroenterology 2001;120:1599-1606.
27. Sifrim D, Dupont L, Blondeau K, Zhang X, Tack J, Janssens
J. Weakly acidic reflux in patients with chronic unexplained cough during 24 hour pressure, pH, and impedance moni- toring. Gut 2005;54:449-454.
28. Rosen R, Nurko S. The importance of multichannel intra- luminal impedance in the evaluation of children with persis- tent respiratory symptoms. Am J Gastroenterol 2004;99:2452- 2458.
29. Nurko S, Rosen R. Use of multi-channel intraluminal im- pedance (MII) in the evaluation of children with respiratory symptoms: a new phenomenon? J Pediatr Gastroenterol Nutr 2005;41:166-168.