대한방사선의 학회지 1994: 30(2): 235-241
상악골 및 하악골 법 랑아세포종의 CT 와 MR 소견 1
나동규·한문희·김 명 진 2. 장기 현
목 적:상악글 및 하악골 법랑아세포종 (ameloblastoma) 의 특징적인 CT 및 MRI 소견을 알고자 후 향적 연구를하였다.
대상 및 방법·병리조직학적으로 확진된 법랑아세포종 11 예와 법랑아세포 악성종양 1 여|를 대상으로 하였고 법랑아세포종 7 예는 수술후 재발한 경우였다. CT는 11 명의 환자에서 시행되었으며 MRI 는 3명 의 환자에서 시행되었다.
결 과:종앙의 형태는 고형종앙, 단일 낭성 종앙, 흔합형이 각기 4예 였다. CT 및 MRI 소견상 앙성법랑 아세포종 11 예중 원형 혹은 타원형의 팽창형 증괴를 나타낸 례가 9예, 경계가 분명한 팽창성 골파괴 9여 1 , 종앙의 부분적 팽륭 6여 1 , 연부 조직의 부분적 침윤이 4예에서 관찰되었다. 법랑아세포 악성 종앙 1예는 불분명한 경계 및 심한 침습성을 나타냈다. 단일 낭성 종앙의 경우에는 매복치( unerupted teeth) 및 내부의 작은 걸절 (mural nodule)OI 관잘되었다. MRI 를 시행한 3여|는 Tl강조영상에서 주위 근육과 등강도의 신호 강도를 T2강조영상에서는 약 고강도의 신호 강도를 나타냈고 종앙 벽, 중격, 고 형 부위는 강한 초영 증강을 나타냈다. 원발성 종앙과 재발성 종앙과의 차이는 발견되지 않았다.
결 론 ; 법랑아세포종은 낭성, 고형, 혼합형의 다양한 3가지 형태를 나타냈으며 특징적으로 주위와 분명한 경계를 갖는 팽창형의 증괴와 국소적 침습성을 보였다. 또한 단일낭성 법랑아세포종의 경우 함 치성 낭종과의 감별이 어려웠으나 종앙 내부 결절이 중요한 감별점이 되었다. 원발성 종앙과 재발성 종앙 사이의 차이점은 발견되지 않았다.
서 를응 ‘-
본 연구의 목적은 CT 흑은 MRI를 시행하고 병리학적 으로 확진된 볍 랑아세 포종 (ameloblastoma) 빛 법 랑아세 포 악성종양 (ameloblastic carcinoma)을 대상으로 하여 법랑아세포종의 영상진단 방법으로는 단순촬영, 전산화 감별 진단에 펼요한 특정적 인 소견을 알고자 하였다.
단층촬영 (Computed Tomography, CT), 자기공명영상 (Magnetic Resonance Imaging, MRI)이 있으나 단순촬 영소견으로는 다른 양성 치성 종양 (benign odontogenic tumor) 과의 감별이 어려우며 수술시 종양의 파급된 정도 를 정확히 파악하기 어려운 반면 CT의 경우 종양의 특성 을 알 수 있으며 종양의 파급된 정도를 정확히 파악할 수 있다는 장점으로 인해 진단 및 치료방침 결정에 유용한 검 사방법으로 알려져 있다(1-3). 또한 MRI는 CT 에 비해서 종양의 발견 및 연부조직으로 침습한 종양의 윤곽을 파악 하는점 뿐아니라수술후소견과종양의 재발을구분함에 있어서 더욱 우수한 것으로 알려져 있다 (4 -6). 법랑아세포 종의 CT 소견에 관한 체계적인 보고는 그리 많지 않으며 저자들이 알기로는국내에서는아직 없다.
l 서울대학교 의과대학 방사선과학교실 2서룰대학교 치과대학 구강외과학교실
이 논문은 1993년 6월 10일 접수하여 1993 년 8월 31 일에 채택되었음
대상및방법
1988년 6월부터 1992년 6월까지 수술 및 생검을 통해 병 리조직학적으로 확진된 볍랑아세포종 11 예와 법랑아세포 악성종양 1 예를 대상으로 하였고,법랑아세포종의 조직학 적 구분으로는 포상형 (follicular type) 이 1 예, 총상형
(plexiform type) 이 3예, 포상형과 총상형이 흔합된 례가 7예, 법랑아세포 악성종양이 1 예였다. 종양의 위치는 상악 골이 2예, 하악골이 10예였으며 법랑아세포종 7예는 수술 후 재발한 경우였고, 법랑아세포 악성종양은 법랑아세포 종에서 수술후 재발한 종양으로 양성 종양에서 악성 종양 으로 변형된 경우로 생각된다. 환자들의 남녀 비율은 남자 6명 여자 6명 이었고, 연령 분포는 12세 -71세 였으며 평균 연령은 41 세 였다.
CT 촬영은 11명의 환자에서 시행하였으며 자기공명영 m
ι
대한밤사선의학회지 1994; 30(2) : 235-241
Table 1. Summary of the Cases
Case Age/Sex Site Histology Type Growth pattern Margin Primary /recurrence Others 12/F maxilla mixed unlcystlc expansile smooth,cl ear P mural nodule
homogeneous focal bulging unerupted tooth
2 14/F mandible plexiform unicystic expansile smooth,clear P mural nodule homogeneous
3 40/F mandible plexiform unicystic expansile smooth,clear R homogeneous focal bulging focal invasion
4 39/F mandible mixed unicystic expansile sm ooth ,cl ear R homogeneous
5 58/M maxilla mixed solid expansile smooth,clear P
homogeneous
6 341M mandible mixed solid expansile smooth,clear P tooth floating
heterogeneous focal bulging focal invasion
7 62/F mandible foll icular solid sl. expansile* sm ooth ,cl ear R heterogeneous round mass
8 57/M mandible mixed mixed** expansile smooth,clear R
heterogeneous focal bul ging focal invasion
9 22/F mandible plexiform mixed expansile smooth ‘이 ear P unerupted tooth
heterogeneous focal bulging
10 72/M mandible mixed mixed expansile smooth,clear R
heterogen eou s
11 46/F mandible mixed mixed expansile smooth,clear R
heterogeneous focal bulging focal invasion
12 311M mandible carcinoma solid infiltrative i rregul ar R lung metastasis
hetetogeneous aggreslve
InvaSlon
*sl. expansile=slight expansile **mixed=solid and cystic
상 (MR I)은 3명의 환자에서 시행하였다. 법랑아 세포종 2예에서는 CT와 MRI를 함께 시행하였고 1 예에서는 MRI만 시행되었다.CT 촬영은 11명의 환자에서 GE 9800 및 GE 8800 장치를 이용하여 통상적인 방법으로 조영제 주입후의 축상 및 관상영상을 얻었으며, MRI는 3명의 환 자에서 2.0 Tesla 초전도형 장치 (Goldstar Spectro-20000) 를 이용하여 spin echo 방법으로 반복시간 (repeti ti on time, TR) 500msec, 에코시간 (echo time, TE) 30- 50msec의 T1강조영상과 TR/ TE 2000/30-40 양자농도 강조영 상 빛 TR / TE 20000/80 T2강조영 상을 축상영 상 으로 얻었고, 체중 1kg당 0.1mmol의 Gd-DTPA (Magnevist, Schering) 를 정맥 주사한 후 축상영상 및 관 상영상의 T1 강조영상을얻었다.
CT를 시행한 11예에서 종양의 CT 소견을 종양의 모양,
경계, 균질성 정도를 중심으로 분석하였으며 각 종양의 형 태를 낭성 (cystic), 고형 (s이id) , 흔항형 (mixed)으로 분류 하였다. 또한 MRI를 시행한 3예에서는 종양의 신호 강도 및 조영증강 정도를 분석하였으며 각 종양에서 조직학적 유형 에 따른차이 및 재발된 종양과원발성 종양과의 차이 유무를알아보았다.
결 과
종양의 중심 위치는 상악골의 경우 2예 모두 대구치 부 위 (molar area)에 있였고 하악골에서 발생한 경우는 10예 중 대구치-하악지 부위 (molar-ramus area) 가 3예, 하악지 (ramus of mandible) 가 1 예, 하악골 전체를 침범한 경우 가 1예 였으며 하악골 부분절제술후 재발한 5 예에서는 종 양이 저작근강 (masticator space) 을 중심으로 협부 (buc
cal space) 혹은 측두강 (temporal space) 로 파급되어 위치 하는 소견을 보였다. 종양의 크기는 직경은 2-7cm사이였 으며 평균 직경은 3.8cm이었다. 양성 법랑아세포종 11예 중에서 단일낭성 (unicystic) 은 4예, 고형 종양은 3여], 낭성 과 고형부분을 함께 보인 흔합형 종양이 4예였다. 양성 법 랑아세포종 11 예중 CT를 시행한 10예의 CT 소견은 단일 냥성 종양 4예중 2예에서 내부에 작은 결절 (mural nod- ule) 이 있었고, 단일낭성 종양 2여l 와 흔합형 종양 l 예에서 매복치 (unerupted tooth) 가 관찰되었으며, 단일낭성 종양 의 낭성 부위의 음영은 뇌척수액과 비슷한 저음영을 나타 냈고 내부의 결절부위는 주위 근육과 비슷한 음영을 나타 냈다 (Fig. 1,2). 흔합형 종양에서는 냥성 부분은 뇌 척수액 과 비슷한 음영을 그리고 고형 부분은 근육과 같은 음영을
i
…
a b
a
보였고, 4 예중 3예에서 종양 내부에 불규칙한 모양의 중격 이 관찰되 였다(Fig. 3). 또한 고형 종양은 주위 근육과 비 슷한 음영을 나타냈다 (Fig. 4, 5). 양성 법랑아세포종 11예 중 단일냥성 종양 4여l 및 고형종양 1 예는 대체로 균질하였 으며, 고형종양 2예와 흔함형 4예는 불균질한 소견을 나타 냈다. 종영:의 모양은 볍랑아세포종 11 예 모두 팽창성의 원 형 흑은타원행의 모양을나타냈고 6예에서 부분적인 팽륭 (bulging) 이 동반되었으며, 종양의 경계는 모두 대체로 매 끄럽고 분명한 경계를 보였으나 11 예중 4예에서는 종영내 의 한 부분에서 연부조직을 침윤하는 경계가 불명확한 부 위가 관찰되였다. 또한 하악골 절제술후 재말한 2 예를 제 외하고 나머지 9예에서 팽창성으로 골피질을 미란시켜 부 분적으로 골피질을 파괴시키는 소견을 나타냈고 주위 상악 골이냐부비동에 팽창성의 골파괴를나타냈으나파괴된 인 접 구조물과의 경계는 분명하였다 (Table 1) 볍랑아세포 악성종양은양성 법랑아세포종과는다르게 경계가매우불 규칙하였고 주위 연부조직으로 침윤하는 모양을 나타냈으 며, 두개골 및 뇌를 직접 침융하는 소견을 보였고 폐로 헐
나동규 외 . 상악골 및 하악골 법랑아세포종
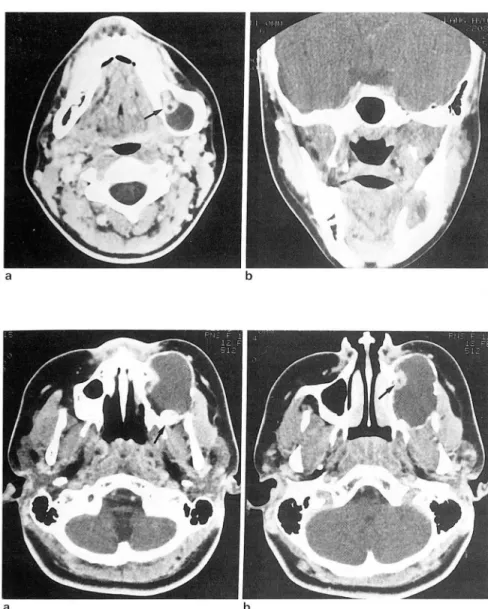
Fig. 1. case 2
14-year-old-girl with cystic mandibular ameloblastoma. Post-contrast axial CT scan(a) shows an expansile cystic mass in body portion 01 the left mandible with homogeneous low density. There is a small enhancing nodule in the medial as- pect 01 the lesion(arrow). A local destruc- tion 01 the medial cortex is demonstrated on coronal image(b)
Fig. 2. case 1
12-year-old-girl with cystic maxillary am- eloblastoma. Post-contrast axial CT scan (a) shows an expansile cystic mass in mo- lar area 01 the left maxilla. There is an molar unerupted tooth within the tumor (arrow). Cortical thining and local cortical destruction is demonstrated in the lateral aspect 01 the lesion and there is an en- hancing nodule in the medial aspect 01 the lesion(arrow)(b). Enhancing mural nodule was helpl미 in distinguishing ameloblastoma Irom dentigerous cyst
행성 전이를 나타냈다 (Fig.6)
MRI를 시행한 3예는 고형 종양이 1여l 흔합형이 2예 였 는데, 종양의 신호 강도는 T1 강조영상에서 고형부분은 주 위 근육과 같거나 약간 높은 신호깡도를 나타냈고 낭성부 위는 근육보다 낮은 신호강도를 보였으며 3예 모두 고형부 분, 종잉:벽, 내부 중격 부위는 조영제에 의해서 강한 조영 증강을 나타냈다. T2 강조영상에서는 고형 부분은 약한 고 신호강도를 보였고 낭성부위는 매우 강한 신호강도를 나타 냈다 (Fig. 3, Fig. 5).
원발성 종양과재발성 종양의 차이점은없였는데 종양의 형태에 있어서 단일 낭성의 경우가 원발성 종양 2례, 재발 성 종양 2예였고, 고행 종양도 각기 2예로 동일하였고 흔함 형은 각기 l 예 및 3예로 양측 모두 다양한 형태를 나타냈 다. 또한 종양의 모양, 경계, 균질성 및 음영, 신호강도에 있어서도 분영한 차이점을 찾지 못했으며 종양의 조직학적 구분에 따른차이점도발견되지 않았다.
•
237 -
대 한 방 사 선 의 학 회 지 1994: 30(2): 235- 241
a
c
a
b
d
b
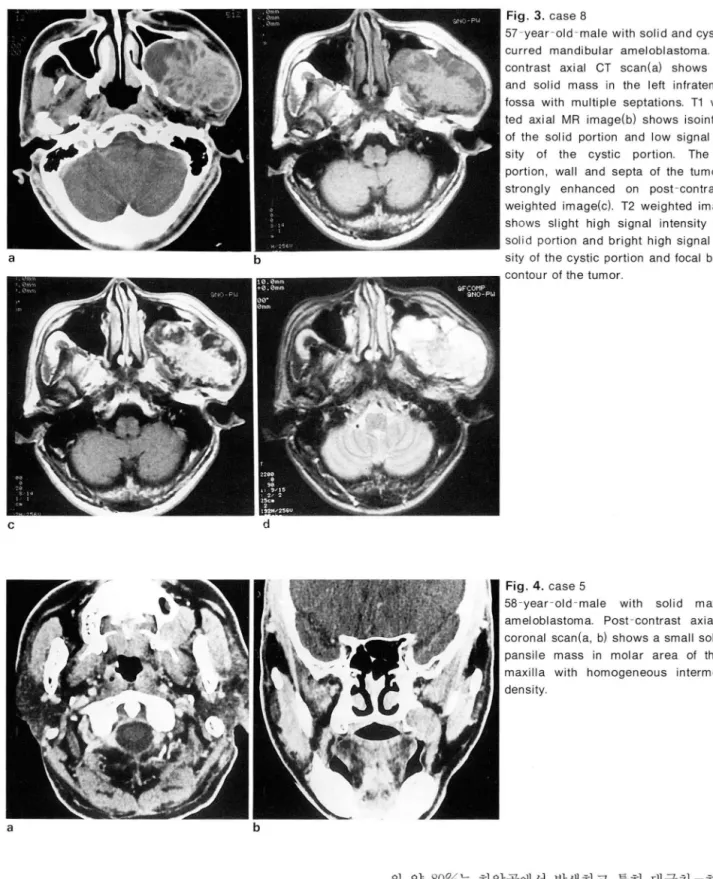
Fig. 3. case 8
57-year-old-male with solid and çystic re curred mandibular ameloblastoma. Post- contrast axial CT scan(a) shows cystic and solid mass in the left infratemporal fossa with multiple septations. T1 weigh- ted axial MR image(b) shows isointensity of the sol id portion and low signal inten- sity of the cystic portion. The solid portion, wall and septa of the tumor are strongly enhanced on post-contrast T1 weighted image(c). T2 weighted image(d) shows slight high signal intensity of the solid portion and bright high signal inten- sity of the cystic portion and focal bulging contour of the tumor
Fig. 4. case 5
58-year-old-male with solid maxillary ameloblastoma. Post-contrast axial and coronal scan(a, b) shows a small solid ex- pansile mass in molar area of the left maxilla with homogeneous intermediate density
의 약 80%는 하악골에서 발생 하고 특히 대구치 -하악지 고 찰 (molar-ramus) 부위에서 많이 발생하며, 연령층은 주로 20
세와 40세 사이에 분포하고 수술후 재발이 잘되는 것으로 법랑아세포종은 에나벨기 (enamel organ) 의 잔여조직 보고되어있다 (7-11).
흑은 치성 낭종(odontogenic cyst) 에서 발생하는 양성 종 종양의 단순촬영소견으로는 부채꼴모양 (scalloped mar- 양으로서, 치성 종양 (odontogenic tumor)중 약 10%로 치 gin) 의 골피질 팽창, 다방성 (multiloculation) 의 비누거품 아종(odontoma) 다음으로 두번째 많은 종양이며 악골 종 (soap bubble) 모양, 치근 흡수 (resorption)등이 있으나 양의 1%를 차지하는 것으로 알려져 있다.(7, 8). 또한 종양 비특이적인 소견으로 진단적 가치가 높지 못하며 (12, 13),
a b
c d
a b
법랑아세포종의
CT
소견에 대하여는 종양이 골피질을 팽 창시키며 부분적인 골피질의 파괴를 동반하는 것으로, 그 리고 단일냥성,다낭성, 고형, 혼합형의 다양한 형태를 나타 내는 것으로 보고되어 있으나 CT소견에 대한 연구보고는 많지 않다(1-3). 본 연구에서는 종양이 냥성, 고형, 흔합형 의 3가지 형 태 및 균칠성 에 있어서 다양한 소견을 나타냈 으며 CT소견상 대체로 경계가 분명하고 주위 골을 미란시 키거나 부분적으로 파괴시키는 중심성 팽창형의 종양으로239
나동규 외 상악글 및 하악골 법랑아세포종
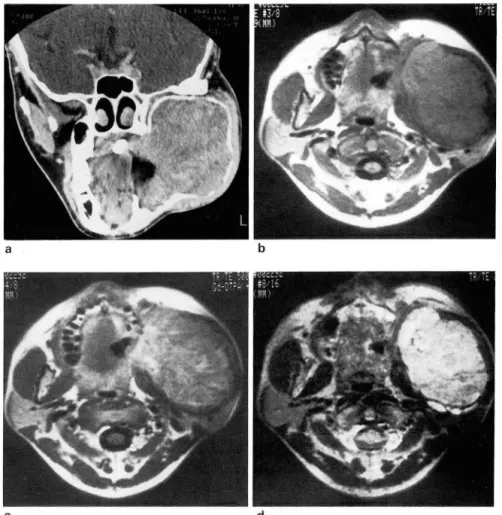
Fig. 5. case 6
34-year-old-male with solid mandibular ameloblastoma. Post-contrast coronal CT scan(a) shows huge expansile slight het.
erogeneous solid mass in molar-ramus area of the left mandible. Extensive bal.
looning of bony cortex and focal cortical destructions are demonstrated. T1 weigh- ted axial MR image shows isointense sig- nal intensity of the mass(b) and post-con- trast T1 weighted image shows hetero- geneous enhancement of the mass(c). T2 weighted image(d) shows heterogeneous high signal intensity of the mass and focal bulging contour of the tumor
Fig. 6. case 12
31-year-old-n1ale with presumed amelo- blastic carcinoma
Post-contrast axial CT scan shows ag- gressive invasion of the maxilla and ir- regular infiltration of the deep soft tissue by the tumor(a). The destuction of the skull coronal image(b)
관찰되었고 일부에서는 부분적인 팽윤과 종양의 한 부위에 서 주위 조직으로 침윤하는 경계가 불명확한 국소적 침습 성이 관찰되었다. 종양은 대체로 주위조직과 경계가 분명 하였으나 심한 팽창성 파괴 및 부분적 침습 소견이 관찰되 였는데, 임상적으로는 고형 혹은 다낭성 종양이 단일냥성 종양보다 국소적 침습이 더욱 심하고 재발율이 높은 것으 로 알려져 있고 (8, 9, 14), 본 연구에서도 종양 크기가 크고 심한 국소적 인 확장 및 침습을 보인 4예는 모두 고형 혹은
대 한 방사 선 의 학회 지 1994; 30(2) : 235- 241
혼합형의 종양이었다. 단일낭성종양은 임상적드로 다른 형 태보다 덜 침습적인 형태를 보이며, 젊은 연령층과 하악골 에 가장 많이 발생하고 재발율이 상대적으로 낮은 것으로 알려져 있다. 또한 단일냥성종양은 종종 대구치의 매복치 와 낭종내의 결절이 동반되고 대개 함치성냥종 (dentiger ous cyst) 과 유사한 모양을 나타내는 것으로 보고되어 있 고(8, 15), 일부 법랑아세포종은 함치성 낭종의 상피세포에 서 낭종내 결절로 발생하는 것으로 알려져 있다 (16)
.
본 연 구에서는 4예의 단일 낭성종양 중에서 2예에서만 낭종내 결절이 관찰되였는데 1예에서는 매복치가 동반된 경우로 병 리소견상 함치성 냥종내에셔 볍랑아세포종이 발생한 예 였다. 실제 저자들이 경험한 함치성 낭종 2예에서 CT소견 상 매복치가 동반된 단얼낭종으로 나타났는데 단일낭성 법 랑아세포종과의 감별이 어려웠으며 낭종내 결절이 함치성 낭종과의 중요한 감별점이 될 것으로 생각된다 (6, 16, 17) (Fig 2). 법랑아세포 악성종양은 대조적으로 주위 조직으 로 매우 심한 캠습도를 나타냈으며 경계도 불규칙하였는데CT
소견상 다른 악성육종과 비슷한 소견을 나타냈다. 법 랑아세포 악성종양은 일반적으로 악성 법랑아세포종 (malignant ameloblastoma) 과 구멸하여 사용하는데 볍랑아세 포악성종양은조직학적인 악성종양의 소견이 있는경우이 며 악성 법랑아세포종은 조직학적으로 양성 법랑아세포종 과 비슷한 양성의 소견을 보이나 전이를 일으킨 경우를 말 하고 법랑아세포 악성종양은 임상적으로 일반 볍랑아세포 종보다 침습도가 높고 폐와 주위 임파절로 전이를 잘하는 것으로 보고되어있다 (8, 18).
법랑아세포종의 MR 소견으로서는 Weissman등이 상악 골에 생긴 악성 종양과 비슷한 침습성을 보인 종양을 보고 한 바 있다(19). 또한 Minami등은 종양이 고형 성분과 낭 성 성분을 함께 포함하는 혼합형태를 나타내고, 불규칙한 두터운 벽, 유두형 돌출모양, 다방성 및 조영제에 의해 종 양내 고형성분 및 중격부위가 강한 조영증강을 나타내는 것으로 보고한 바 있다 (6). 본 연구에서는 MRI를 시행한 흔합형 종양 2예 모두 불규칙한 두터운 종양벽과 유두형 돌출이 관찰되었으나혼합형 종양 2예중 1 예에서는종양벽 이 일부에서는 매끄럽고 앓은 부위가 한 종양내에 혼합되 어 나타났고 MRI를 시행한 고형 종양 l예에서는 뚜렸한 종양벽 이 관찰되 지 않았다. 또한 흔합형 종양 2여l 에서 모 두 다방성의 소견과 조영제에 의한 중격부위와 고형성분의 강한 조형증강이 관찰되어 일치된 소견을 나타냈다. 그러 나 종양벽에 관하여는
CT
소견을 분석할때 낭성 종양의 경우 종양벽은 부분적으로 골피질이 파괴된 부위에서 매끄 럽고 앓은 벽으로 관찰되었으며, 혼합형 종양의 경우 1 예 에서는 매끄럽고 않은 벽을 나타냈고 다른 례에서는 불규 칙한 두터운 종양벽이 흔합되어 관찰되어 다양한 소견을 나타내였고, 고형 종양에서는 분명한 종양벽이 관찰되지 않아 종양벽은종양의 형태에 따라다양한 소견을보이는 것으로 생각된다. 또한 Minami등은 종양이 작고 종양 주 위 의 골피 질이 보존되 어 있을때 CT가 MRI보다 효과적 이었고 종양이 주위 연부조직을 광범위하게 침습하였을때 종양의 윤곽과 침습 범위를 파악함에 있어서 또한 수술후 종양의 재발과수술후조직변화를구별하는데 MRI가CT 보다 효과적이다고 보고하였으며(
6)
, 본 연구에서도 주위 연부조직으로 침습한 종양의 윤곽을 파악하는데에 MRI 가 CT보다 우수하였다.결론적으로 법랑아세포종은 냥성,고행,흔합형의 다양한 3가지 형태를 나타냈으며 특정적으로 주위와 분명한 경계 를갖는팽창형의 종괴와국소적 침습성을보였다.또한단 일낭성 법랑아세포종의 경우 함치성 낭종과의 감별이 어 려웠으나 종양 내부 결절이 중요한 감별점이 되었고 원발 성 종양과 재발성 종양사이의 차이점은 발견되지 않았다.
*~ C그 고 ~ ‘-C그 헌
1. Heltzanu Y, Mendelsohn DB, Cohen MA. Computed Tom
。graphy 01 Mandibular Ameloblastoma. J Comput Assist Tomogr. 1984; 8(2) : 220-223
2. Cohen MA , Hertzanu Y, Mendelsohn DB. Computed Tomogra.
phy in the Diagnosis and Treatment 01 Mandibular Ameloblastoma: Report 01 cases. J Oral Maxillofac Surg 1985; 43 : 796.801
3. Schultz SM, Twickler DE, Wheeler DE, Hogan TD. Amelo- blastoma Associated with 8asal Cell Nevus(Gorlin) Syndrom CT Findings. J Comput Assist Tomogr. 1987;11(5) :901-904 4. Heffez L, Malee MF, Vaiana J. The role 01 magnetic reson
ance imaging in the diagnosis and management 01 ameloblastoma. Oral Surg Oral Med Oral Pathol. 1988;65(1) 2-12
5. Belkin BA,Papageorge MB, Fakitsas J, Bankoff MS. A cmparative study 01 magnetic resonance imaging versus computed tomography lor the evaluation 01 maxillary and mandibular tumors. J Oral Maxillofac Surg. 1988; 46(12) 1039-1047
6. Minami M, Kaneda T, Yamamoto H et al. Ameloblatoma in the Maxillomandibular Region: MR Imaging. Radiology 1992
; 184 : 389-393
7. Regezi JA, Kerr DA, Courtney RI\A. Odontogenic tumors analysis 01706 cases. J Oral Surg. 1978; 36(1 0): 771-778 8. Shaler WG, Hine MK, Levy BM, Tomich CE. A Textbook of
Oral Pathology. 4th ed. Philadelphia: W. B. Saunders, 1983;
258-313
9. Regezi JA, Scicubba JJ. Oral Pathology: c/inical-pathologic correlation 1 st ed. New York: W. B. Saunders, 1989; 336-349 10. Tsaknis PJ, Nelson JF. The maxillary ameloblastoma: an
analysis 0124 cases. J Oral Surg. 1980; 38: 336-342
11. Sehdev MK, Huvos AG, Strong EW, Gerold FP, Willis GW Ameloblastoma 01 maxilla and mandible. Cancer 1974; 33 324-333
12. Mclvor J. The radiological leatures 01 ameloblastoma. Clin Radiol. 1974; 25: 237-242
13. Eversole LR, Rovin S. Differential radiographic diagnosis 01 lesions 01 the jawbones. Radiology 1972; 105: 277-284 14. Gardner DG, Pecak AM. The treatment 01 ameloblastoma
based on pathologic and anatomic principles. Cancer 1980; 46: 2514-2519
15. Robinson L, Martinez MG. Unicystic ameloblastoma: a prognostically distinct entity. Cancer 1977; 2278-2285
나동규 외 상악글 및 하악골 법랑아세포종
16. Small IA, Waldron CA. Ameloblastomas 01 Jaws. Oral Surg. oblastic carcinoma: a clinicopath이。gic study and assessment 1955; 8 : 281-297. 01 eight cases. Oral Surg Oral Med Oral Pathol. 1987; 64(5) 17. Aquino M, Muzquizy Limon R, Perez Cortez C, Galvan 570-576
Gonzalez A. Computed Tmography 01 dentigerous cyst(Report 19. Weissman JL, Synderman CH, Yousem SA, Curtin HD
。1a case). Pract Odorη。1. 1990;11:47-49 [English abstractl Ameloblastoma 01 the maxilla:CT and MR appearance. AJNR 18. Corio RL, Golblatt LI, Edwards PA, Hartman KS. Amel- 1993; 14: 223-226
Journal of the Korean Radiological Society, 1994; 30(2) : 235-241
The Maxillomandibular Ameloblastoma: CT & MR Imaging
Dong Gyu Na , M.D., Moon Hee Han , M.D. , Myung Jin Kim M.D.' , Kee Hyun Chang, M.D.
Department of Radiology, Seoul National University College of Medicine
1 Department of Oral Surgery, Seoul National University College of Dentistry
Purpose: We retrospectively performed this study to evaluate the charac6teristic findings of maxilloman- dibular ameloblastomas on CT and MR imaging
Materias and Methods: We reviewed hist이。gically proved 12 cases of ameloblastomas, of which 7 cases were postoperative recurrent tumors. one of twelve cases was presumed ameloblastic carcinoma. Eleven cases were examined with CT and 3 cases with MR.
Results: The types were solid in 4, unicystic in 4, and mixed in the rest 4. CT and MRI of 11 ameloblastomas showed concentric expansile mass(n=11), cortical bone thinning and focal bone destruction by the tumors(n=9), well-margined, expansile destruction of surrounding sturctures(n=9), focal bulging of the tumors(n=6) and focal poorly-marginated invasion of tissue planes(n=4). Ameloblastic carcinoma showed ill-defined irregular margin, aggressive invasion of surrounding structures and hematogeneous lung metastasis
Unerupted teeth or mural nodules were found in unicystic ameloblastomas. AII three tumors examined by MRI showed isointensity to muscle on T1 weighted images and slight hyperintensity on T2 weighted images The wall, septa and solid portions of the tumors were strongly enhanced on MR imaging. There was no differ- ence in CT or MR finding between primary and recurrent tumors
Conclusion : Ameloblastomas showed solid, cystic or mixed pattern, and commonly well marginated expan- sile contour with local aggressiveness. Presence of mural nodules on CT in unicystic ameloblastoma with unerupted tooth was helpf비 in distinguishing ameloblastoma from dentigerous cyst
Index Words: Mandible, ameloblastoma Maxilla, ameloblastoma Mandible, CT studies Mandible, MR studies
Address reprint requests to : Dong Gyu Na, M.D., Department of Radiology, Seoul National University College of Medicine 28, Y ongon -dong, Chongno 검 0, Seoul, 110-744 Korea Tel. (02) 760-2519
- 241 -
1994 년도 학회산하 연구회 Conference 안내
1. 신경방사선과학 연구회
일 시 : 1994년 1월 19일 (수)
장 소 : 서울대학교소아병원 임상제1강의실
2 . 흉부방사선과학 연구회
일 시 : 1994년 2월 16 일 (수)
장 소 : 서울대학교소아병원 임상제1강의실
3.
복부방사선과학 연구회 일 시 : 1994년 3월 9일(수)장 소 : 서울대학교소아병원 임상제1강의실
4 . 근골격계방사선과학 연구회
일 시 : 1994년 4월 13일(수)
장 소 : 서울대학교소아병원 임상제 1 강의실
5.
심혈관 및 중재적방사선과학 연구회 일 시 : 1994년 5월 11 일 (수)장 소 : 서울대학교소아병원 임상제1강의실
6.
소아방사선과학 연구회 일 시 : 1994년 6월 8일(수)소 : 서울대학교소아병원 임상제1강의실 장
7.
버뇨, 생식기계방사선과학 연구회 일 시 : 1994년 7월 13일 (수)장 소 : 서울대학교소아병원 임상제1강의실
8.
신경방사선과학 연구회 일 시 : 1994년 9월 14일(수)장 소 : 서울대학교소아병원 임상제 l강의실
9 . 흉부방사선과학 연구회
일 시 : 1994년 10월 12 일 (수)
장 소:서울대학교소아병원임상제l강의실
10.
복부방사선과학 연구회 일 시 : 1994년 11월 9일 (수)장 소 : 서울대학교소아병원 임상제1강의실
1 1. 연구회 P annel 토의
일 시 : 1994년 12월 14 일 (수)
장 소 : 서울대학교소아병원 임상제1강의실