291
외래 호흡기계 질환에서 항생제 사용에 대한 후향적 평가방안
김동숙1·배그린1·김수경1·이학선1·김윤진1·이숙향2*
1건강보험심사평가원 연구조성실, 2아주대학교 약학대학
(2012년 9월 26일 접수·2012년 11월 21일 수정·2012년 11월 23일 승인)
Retrospective Drug Utilization Review of Antibiotics for Respiratory Tract Infection(RTI) in Ambulatory Outpatient Care
Dong-Sook Kim1, Green Bae1, Su-Kyeong Kim1, Hak-Seon Lee1, Yoon Jin Kim1, and SukHyang Lee2*
1Department of Research, Health Insurance Review & Assessment Service, Seoul 137-927, Korea
2College of Pharmacy, Ajou University, Suwon 443-749, Korea
(Received September 26, 2012·Revised November 21, 2012·Accepted November 23, 2012)
As respiratory tract infections (RTI) account for about 60% of all antibiotic prescriptions in outpatient care setting, there are significant concerns about emerging resistance that are largely due to the excessive or inappropriate use of antibacte- rial agents for viral respiratory infections. This study was aimed to develop retrospective drug utilization review (DUR) program of antibiotics for RTIs using Delphi methods. Retrospective DUR criteria of antibiotics for RTIs were identified based on clinical practice guidelines and opinion of experts. Expert panel members were clinical doctors and pharmacists and Delphi method was applied by survey on 16 members of panels. The claim data from Korean Health Insurance Review & Assessment (HIRA) were used to examine trends in outpatient antibiotic prescription between Janunary to December of 2008. As results, Quality index for RTI was assessed for the claim type, antibiotics use of quantity, dura- tion, number and cost. Antibiotic prescription rate for RTIs, Defined Daily Dose (DDD), and duration of antibiotics use were more recognized as significant quality index by experts' opinion. Use of first line agents suggested by guidelines was low and duration of antibiotics use was shorter compared to the recommendations. Antibiotics were over prescribed for RITs. However, dose and duration of antibiotics were under-used.
□ Key words - Respiratory Tract Infections (RTI), Antibiotics, Drug Utilization Review (DUR)
호흡기계 감염(respiratory tract infections, RTIs)은 일반의 (general practitioner, GP)가 외래 항생제 처방 대상 질환의 75%를 차지하고1), 상기도감염(upper respiratory tract infection, URI), 급성 기관지염(acute bronchitis)이 전체 항생제 처방 질 환의 21%를 차지한다.2)미국에서도 일차의료에서 전체 처방 약물 중 항생제 처방이 차지하는 비중은 12~14%로 보고되고 있다.2)
국내에서도 2008년 1월~12월 의료보험 청구 자료에서 외 래 진료 후 항생제 처방 명세서를 분석한 결과,호흡기계 질 환은 내원일수의 92.8%(명세서의 93.1%)로 대부분을 차지했 고, 분석대상 호흡기계 질환(J00~J06, J20~J22)은 내원일수의 61%(명세서의 60.3%)를 차지했다.3)
임상연구 결과를 체계적으로 고찰한 Arroll 등(2009)은 상 기도감염에 대한 항생제 사용의 편익이 불충분하다고 보고하 였고4), Reveiz 등(2010)은 급성 후두염(acute laryngitis)에서 항생제 사용에 대한 체계적 문헌고찰에서, 2개 연구가 조건 을 충족시켰고, 항생제가 급성 후두염 치료에서는 편익이 없 는 것으로 제시하였다.5) Ahovuo-Saloranta A 등(2009)은 급 성 부비동염(acute maxillary sinusitis)에서 항생제 효과에 대 한 체계적 문헌고찰을 수행한 결과, 7일 이상 급성 부비동염 에서 미미한 치료효과가 있으나, 항생제 없이 치료받은 대상 자의 80%가 2주 안에 개선되었다고 밝혔다.6) Smith 등 (2010)은 급성 기관지염에서 항생제 처방이 더 좋은 결과를 가져올 수 있다고 제시하였으나7), Staykova T 등(2009)은 소 아의 급성 세기관지염에서는 항생제 처방을 지지할 근거를 찾지 못했다고 하였다.8) Spinks 등(2010)은 인후통(sore throat)에서 항생제 사용의 편익을 검토한 결과, 27개의 연구 가 기준을 충족시켰고, 상대적 편익은 있으나, 절대적 편익 은 적은(modest) 편이었다.9) 그러나 이러한 질환의 경우 항 Correspondence to : 이숙향
아주대학교 약학대학
경기도 수원시 영통구 원천동 산 5번지 Tel: +82-31-219-3443, Fax: +82-31-219-3435 E-mail: suklee@ajou.ac.kr
생제 효과가 미미하거나 의학적 이득이 없음에도 불구하고 처방되고 있다.2) 국내외 호흡기계 질환에 대한 항생제 사용 지침에서는 급성 부비동염(sinusitis)에서는 항생제를 처방하 지 않고, 만성 부비동염이나 합병증의 위험이 있을 경우 처 방하도록 하고 있다. 인두염(pharyngitis)에서도 바이러스성 인두염에 대해서는 항생제를 쓰지 않고, 세균성에 대한 임상 적 근거가 있을 경우 항생제를 처방하도록 하고 있다. 기관 지염(bronchitis)은 대부분이 바이러스성이므로, 항생제를 처 방할 필요가 없다.11-21)
이에 따라, 2001년부터 의사의 청구내역에 대한 후향적 평 가의 필요성이 제기되었고 약제급여 적정성 평가 사업을 실 시하게 되었다. 건강보험시심사평가원에서는 약제급여 적정 성 평가를 통해 항생제 총량과 급성상기도감염에 대한 항생 제 처방을 관리하고 있으나10), 보다 구체적으로 상병별, 항 생제별 적정성 향상을 위한 세부관리 기준이 마련되어 있지 못하며, 바이러스성 호흡기 감염에도 불필요한 항생제 사용 이 높은 것으로 나타났다. 특히, 세팔로스포린계 3세대나 퀴 놀론계과 같이 부적정 사용으로 인한 내성 등 사회적 비용 문제가 더욱 클 수 있으므로, 이를 적정하게 관리할 세부 기 준 및 관리방안이 연구될 필요가 있다.
본 연구는 외래 호흡기계 질환에서 사용하는 항생제에 대 한 후향적 평가방안을 모색하고자 하였다. 이를 위해 델파이 기법을 이용하여 공식적 합의를 도출하였고, 이 결과를 적용 해 후보지표값별로 국내 항생제 사용량을 분석하였다.
연구대상 및 방법
평가지표(안) 개발 과정
평가지표(안)을 개발하기 위해 주요 외국의 진료지침과 외
국의 질지표를 검토하고, 문헌고찰 결과에 따라 항생제를 적 절히 사용할 질환, 용량, 투여기간 등에 대한 지표(안)를 개 발하였다. 또한, 심사평가원 심사위원, 관련 보건의료 전문가 등으로 자문단을 구성하였고, 전문가 조사를 통해 지표를 선 정하였다.
전문가 패널 구성 및 델파이 조사
학계의 자문을 구하여 16명의 전문가 패널을 선정하였다.
구성은 호흡기계 질환을 진료하는 전문과목을 중심으로 5개 학회(소아과학회, 결핵 및 호흡기학회, 이비인후과학회, 가정 의학과학회, 대한감염학회)의 각 1인씩, 5개 개원의 협회(소 아과, 내과, 이비인후과, 가정의학과, 일반의) 각 1인씩, 학계 전문가 2인, 임상약학 전문가 2인, 건강보험심사평가원 심사 위원 2인으로 구성되었다.
Nominal group method 1, 2라운드는 우편조사방식으로 진 행하였다. 1라운드에서 10명이상의 패널이 동의할 경우 그 항목에 대해서는 완료하고, 그렇지 않은 항목에 대해서는 2 라운드로 진행하고, 2라운드에서는 1라운드에서 나타난 결과 를 정리하여 전문가 패널에게 제공하였고, 2라운드에서도 1 라운드와 마찬가지로 진행하였다.
연구결과
외국의 지침 및 지표 검토
항생제 남용으로 내성이 증가하게 되자, 각국에서는 항생 제 내성을 억제하고자, 호흡기계 질환을 중심으로 항생제의 적정사용에 대한 지침을 발표하였다. 항생제 적정사용 지침 은 호흡기계 질환 중 바이러스성 질환에서 있어서 불필요한 항생제 사용을 감소하는 것, 항생제 치료가 필요한 감염질환 Fig. 1. Process of Developing the Evaluation Plan.
의 경우 원인균에 적합한 항생제를 선택하는 것을 주로 다 루고 있다.
의사를 대상으로 하는 외국의 호흡기 감염질환에 대한 지 침을 검토한 결과는 아래와 같다. 미국의 Centers for Disease Control and Prevention(CDC)은 여러 관련부처와 협력하여 적 절한 항생제 사용과 관련한 지침을 제공하고 있다. 미국의 CDC와 학회 등에서 입원 영역에서는 감염방지를 위한 지침 을 제공하고 있고, 외래영역의 상기도 감염에 있어서 적절한 항생제 사용과 관련한 지침을 제공하고 있다. 성인의 급성상기
도감염, 비특이적 상기도감염, 급성 비부비동염(rhinosinusitis), 급성 인두염(pharyngitis), 합병증이 없는 급성 기관지염 (bronchitis)에 대한 적절한 항생제 사용원칙, 기침 진단 및 관 리에 대한 American College of Chest Physicians (ACCP) 지 침을 제공하고 있다. 소아에 대해서는 소아 상기도 감염에 대 한 항생제 사용 원칙, 기침 진단 및 관리, 삼출성 중이염 진 단 및 관리, 인두염, 급성 부비동염(sinusitis), 기관지염, 감기 에 대한 항생제 사용 원칙 지침을 제공하고 있다.11),12)
영국의 National Institute for Clinical Excellence(NICE)에서 Table 1. Guidelines on the Use of Antibiotics for Respiratory Tract Diseases in Other Countries (Regarding Immediate Prescription)
Disease Korea1) U.S2) Canada3) U.K4) Australia5)
Acute otitis media (Children)
48-72 hours, Wait and see without
prescribing antibiotics △
<6 months ◎ 6 months - 2 years △a)
2 years or older △
<24 months ◎ 2 years or older △ b)
<24 months ◎ Aural discharge ◎
2 years or older △c) <6 months ◎ 6 months -2 years △
2 years or older △
*otitis media with effusion ×
*otitis media with effusion ×
*otitis media with effusion ×
Sinusitis △d) △e) *Acute: ×
*Adult, chronic △
*Acute: ×
*Immediate prescription if the disease affects the whole body or there is a risk of complication △
△
Pharyngitis △f) △ △ Delayed prescription
△f) △
Bronchitis
/Nonspecific cough × ×g) × × ×
Bronchiolitis
/Nonspecific URI N/A × N/A × ×
◎: Immediate prescription, △: Prescribe when it is confirmed, it is bacterial or there is clear clinical evidence, ×: Antibiotics is not recommended.
Note: 1) Korea
- Kim SW. Upper Respiratory Infections in Audult. J Korean Med Assoc 2010; 53(1): 10-19.28) 2) U.S
- Diagnosis and management of otitis media in children. National Guideline Clearinghouse Guideline Synthesis 2010.11)
- Wong DM, Blumberg DA, Lowe LG. Guidelines for the use of antibiotics in acute upper respiratory tract infections. Am Fam Physician 2006; 74:
956-66.12) 3) Canada
- Guideline for the diagnosis and treatment of acute otitis media in children.. 2001.18) - Guideline for the diagnosis and management of acute bacterial sinusitis. AMA 2001.19) - Guideline for the diagnosis and management of acute pharyngitis. 2010.20)
- Guideline for the management of acute bronchitis.2001
- Guideline for the management of acute exacerbation of chronic bronchitis(AECB). 2001.21) 4) U.K
- National Institute for Health and Clinicl Excellenc(NICE). Respiratory tract infections - antibiotic prescribing. NICE clinical guideline 69. July 2008.13) - Diagnosis and management of childhood otitis media in primary care.14)
- Management of sore throat and indication for tonsillectomy.15)
- Respiratory tract infections-antibiotic prescribing: Prescribing of antibiotics for self-limiting respiratory tract infections in adults and children in primary care. NICE. 2008.16)
- Guidance for the care of NHS patients in Leeds. 2008.17) - CKS website (http://cks.nhs.uk)29)
5) Australia
- Clinical audit: management of specific respiratory tract infection30)
a) For 6-month ~ 2-year children, even though it is not confirmed, if symptoms are serious, antibiotics is prescribed. For 2-year or older children, when it is confirmed and is accompanied by symptoms, antibiotics is prescribed.
b) For 2-year or older children, when it is confirmed and is accompanied by symptoms, antibiotics is prescribed.
c) Prescribe after 72 hours
d) If it is acute and bacterial, and symptoms are not improving or serious. prescribe antibiotics.
e) If it is acute and bacterial, and symptoms are not improving for 10 days or serious. prescribe antibiotics.
f) Acute pharyngitis includes quinsy and acute pharyngotonsillitis.
g) For children, wait and see for 14 days and then prescribe antibiotics.
는 감염관리, 호흡기 감염에 대한 지침을 제공하고 있고13)-17), 스코틀랜드의 Scottish Intercollegiate Guideline Network (SIGN)에서는 소아의 기관지염, 소아의 중이염, 인후염 및 성인의 하기도 감염에 관한 지침을 제공하고 있다. NICE는 일차 및 지역사회 관리에서 감염관리, 보건의료인 관련성 감 염예방, 호흡기 감염에 대한 항생제 처방을 제공하고 있고, SIGN은 소아에서의 기관지염, 일차의료 영역에서 소아의 중 이염 진단 및 관리, 인두통(sore throat) 관리와 편도선 절제 술 적응증, 성인의 하기도 감염에 대한 관리에 대한 지침을 제공하고 있다.
캐나다의 Alberta Medical Association에서는 Toward Optimized Practice 웹사이트를 통해, 급성 세균성 부비동염 (sinusitis) 진단 및 관리, 급성 기관지염 관리, 급성 인두염 (pharyngitis) 진단 및 관리, 만성폐쇄성폐질환(chronic obstructive pulmonary disease, COPD)의 악화방지, 급성 중이염 진단 및 관리, 지역사회 획득 폐렴의 진단 및 관리(성인, 소아), 장기요 양원(nurshing home)에서의획득성 폐렴에 대한 진단 및 관리 등 질환별로 임상진료지침을 제공하고 있다.18)-21)
호주의 Office for Aboriginal and Torres Strait Islander Health(OATSIH)에서는 중이염에 대한 권고사항을 제공하고, 주정부인 New South Wales Health Department에서도 소아 의 중이염에 대한 가이드라인, 소아의 인후염에 대한 가이드 라인, 소아의 상기도 감염에 대한 지침을 제공하고 있다.
영국, 프랑스는 항생제의 적정 사용을 관리하기 위해, 의 사를 대상으로 항생제 사용을 모니터링한 결과를 제공하고 있고, 이를 인센티브 지급에 활용하기도 한다. 호주, 캐나다 에서는 적절한 의약품을 사용할 수 있도록 교육 자료를 제 공하고 있었고, 캐나다, 미국에서는 호흡기계 질환에서 항생 제 처방에 대해 평가 지표를 산출해 제공하며, 후향적 DUR (Drug Utilization Reveiw) 혹은 인센티브 지급에 활용하기도 한다. 외국의 호흡기계 질환에 대한 항생제 지표를 정리한 결과는 Table 3과 같다.
영국 Prescribing Support Unit(PSU)에서는 국내와 유사하 게 항생제의 품목수, 비용 제네릭 항생제 처방률 등의 지표 와 권고 항생제 사용에 대한 비율을 진료소(practice) 혹은 일반의(GP)에게 제공하고 있다.22,23) 프랑스 건강보험공단의 Table 2. First Choice of Antibiotics and Its Dose for Respiratory Tract Diseases
Disease Korea1) U.S2) Canada3) U.K4) Australia5)
Acute otitis media (Children)
• Amoxicillin, high dose a)
• Amoxicillin/clavulanate • Amoxicillin, high dose b)
• Amoxicillin/clavulanate *Antibiotics within 6 weeks ×
• Amoxicillin • Amoxicillin • Amoxicillin
• Amoxicillin/clavu- lanate
*penicillin allergy
(Type 1 hypersensitivity reac- tion)
• Erythromycin
• Clarithromycin
• Azithromycin
*penicillin allergy(not Type 1) Cefnir,Cefpo-
doxime,Cefuroxime
*Parenteral :Ceftriaxone
*penicillin allergy(Type 1 hypersensitivity reaction)
• Clarithromycin
• Azithromycin c)
*penicillin allergy (not Type 1) Cefnir,Cefpo- doxime,Cefuroxime
*parenteral :Ceftriaxone
β-lactam allergy
• EM-sulfisoxazole
*Antibiotics within 6 weeks
○, Improvement within 48- 72 hours X, relapse
• Amoxicillin/clavulanate
• Clarithromycin
*penicillin allergy Erythromycin
penicillin allergy
• cefuroxime
• cefaclor
Acute sinusitis
• Penicillin V
• Penicillin G benzathine
• Amoxicilin
• Ampicillin
• Amoxicillin • Amoxicillin d) • Amoxicillin e)
• Doxycyclin(>12 years)
• Macrolides (EM, clarithromy- cin)
Amoxicillin Amoxicillin/clavu- lanate
penicillin allergy
• EM,clindamycin, 1G cepha
β-lactam allergy
• Clindamycin
• TMP/SMX
• Macrolides
β-lactam allergy
• EM-sulfisoxazole
• TMP/SMX
penicillin allergy Cefuroxime, Cefaclor Doxycyclin (>8 years)
Acute pharyngitis
• Penicillin V
• Penicillin G benzathine
• Amoxicilin
• Ampicillin penicillin allergy
• EM,clindamycin, 1G cepha
• Penicillin V (Veetids)
• Penicillin G benzathine
• Penicillin V
• Amoxicilin (Under 10 years)
β-lactam allergy
• Clindamycin
• Amoxicillin/clavulanate
• Penicillin V • Penicillin V
• Benzathine penicillinf)
Bronchitis
*When acute bronchitis lasts more than 10 days
• Amoxicillin
• macrolides
*Acute exacerbation of chronic bronchitis
• macrolides
• β-lactamase inhibitor
• 2G, 3G oral cepha
• azithromycin
*Acute exacerbation of chronic bronchitis
• Amoxicillin 500 mg β-lactam allergy
• Doxycycline
• Tetracycline
• TMP/SMX
• Amoxicillin 500 mg
• Doxycycline
*Acute exacerbation of chronic bronchitis
• Amoxicillin β-lactam allergy
• Doxycycline
진료정보시스템(SIAM)에서도 항생제 처방률을 의사별로 통 보하고 있고24), 호주의 National Prescription Service Limited (NPS)는 의사에게 비특이적 상기도감염에서 항생제 처방, 급 성 중이염에서 항생제 처방에 대한 지표를 의사 스스로 산출 하도록 처방지표를 정의하고 있다.25)미국 National Committee for Quality Assurance(NCQA)의 Intergrated Healthcare Associa- tion(IHA) California Pay for Performance(P4P) Program에서는 2009년 상기도감염 소아의 항생제 처방, 급성 기관지염이 있는 성인에 대한 항생제 처방을 지표로 가감지급을 하고 있다26). 반면, 캐나다의 Alberta drug utilization program은 후향적 DUR 프로그램으로서 급성 인두염, 급성 부비동염, 만성 부 비동염, 급성 중이염에서 권고 항생제를 처방하고 있는지를 살펴보고 있다.27)
후보지표에 대한 델파이 조사 결과
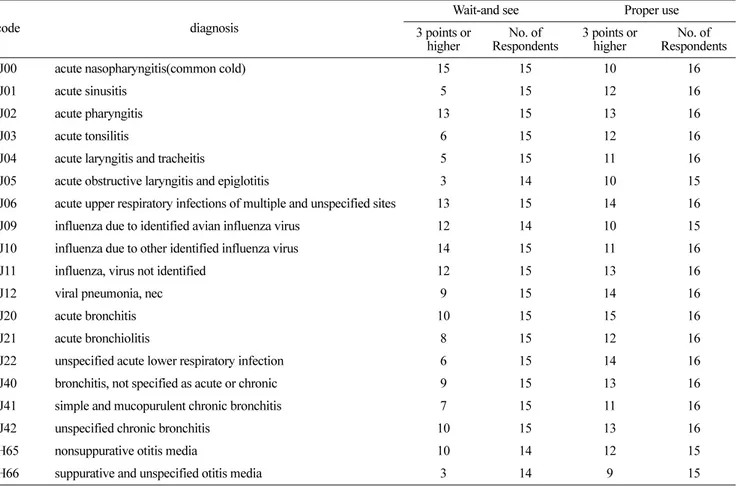
16명의 전문가를 대상으로, Table 4와 같이 호흡기계 질환 별로 항생제를 평가하는 것이 필요한지 질문하였다. 호흡기 계 질환에 대해 항생제를 처방하지 않고 관찰하는 것이 필 요한지, 항생제를 적절하게 사용하는 것이 중요한지에 대해 5점 척도로 질의한 결과, 급성 코인두염(감기), 바이러스가 확인되지 않은 인플루엔자, 급성 인두염, 다발성 및 상세불 명 부위의 급성 상기도감염에 대해서 항생제를 처방하지 않 고 관찰하는 것에 대해 3점이상 응답자가 15명, 14명, 13명, 13명으로 대부분이 관찰하는 필요성을 인지하고 있었다. 반 면, 급성 폐쇄성 후두염(크루프) 및 후두개염, 비화농성 및 상세불명의 중이염에 대해서는 항생제 처방 없이 관찰하는 것에 대해서 3점이상 답한 응답자는 3명으로 항생제가 필요 하다고 판단하는 수준이 높았다. 급성 부비동염, 급성 후두
염 및 기관염, 상세불명의 급성 하기도 감염에 대해서도 3점 이상 답한 응답자가 5명으로 나타났다.
항생제의 적절사용에 대해서는 다발성 및 상세불명 부위의 급성 상기도 감염, 달리 분류되지 않은 바이러스성 폐렴, 상 세불명의 급성 하기도 감염에 대해서 3점이상 응답자가 14 명이었고, 대부분이 호흡기계 질환에서 항생제의 적절사용을 평가하는 것에 대해 동의하고 있었다.
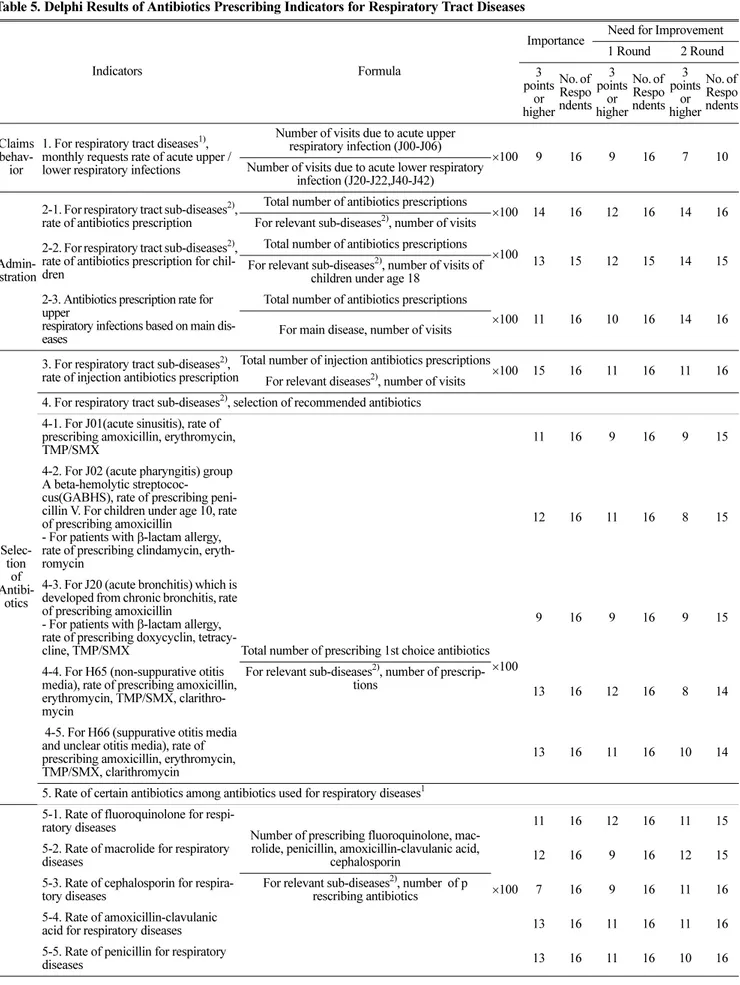
후보지표별 전문가 조사 결과, 문제의 중요성과 개선 필요 성에 대해서 3점 이상 응답자가 9명이상이 많아, 대체로 후 보지표별 평가지표의 적절성에 대해 동의하고 있는 것으로 나타났다. 특히 질환별 항생제 처방, 일일사용량(Defined Daily Dose, DDD)를 기준으로 한 사용량, 항생제 투여일수 에 대해서는 대부분이 평가의 필요성에 대해 높게 인지하고 있었다. 다만, 항생제 중 cephalosporin의 비중에 대해서는 문제의 중요성이 낮아, 2세대 이상으로 범주를 국한할 필요 가 있겠다.
후보지표 값 산출
평가지표는 청구행태, 항생제 투여여부, 선택, 사용량, 투 여기간 및 품목수, 비용으로 구분하여 산출하였다. 항생제 투여여부는 항생제 사용이 권고되지 않는 급성 편도염, 급성 인두염, 급성 기관지염, 화농성 중이염에서 항생제 비처방 혹은 지연처방 전략, 혹은 항생제 처방없이 관찰하는지 판단 하고자, 항생제 처방률을 살펴보았다. 항생제 선택은 Table 3 에 제시한 항생제 권고기준과 캐나다 앨버타의 후향적 DUR 기준을 사용하였다. 항생제 사용량, 투여기간, 비용은 명세서 (처방전) 단위로 산출하였다. 분석자료는 2008년 외래 호흡 기계 질환으로 병원을 방문해 진료받고 청구한 내역을 활용 Table 3. Antibiotics Prescribing Indicators in Other Countries
U.K1) France2) Australia3) Canada4)
(Retrospective DUR) U.S5)6)
Index
Cost and number of antibiotics, generic prescription rate, rate of
"approved antibiotics" against all antibiotics, list of antibiotics with an increasing prescription rate (amoxycillin, erythromycin, trimethoprim, penicillin V), Quinolones-cost or use reduction, rate of cephalosporin against penicillin
Antibiotics prescription rate
Prescription of antibiotics for nonspecific upper respiratory infection
Prescription of recommended antibiotics for acute pharyngitis
Prescription of antibiotics for a child with upper respiratory infection Prescription of recom-
mended antibiotics for acute sinusitis and chronic sinusitis
Prescription of antibiotics for an adult with acute bronchitis
Prescription of antibiotics for acute otitis media
Prescription of recom- mended antibiotics for acute otitis media
Rate of 2-month - 12-year children with oozing otitis media that do not receive antibiotics prescription Note: 1) PSU(Prescribing Support Unit); Asworth et al., 200222); Campbell et al., 200023)
2) France, SIAM24) 3) Australia, NPS25)
4) Canada, Alberta drug utilization program27)
5) U.S., NCQA(National Committee for Quality Assurance)'s IHA(Intergrated Healthcare Association) California Pay for Performance Program Measurement Year 2009 P4P Draft Manual26)
6) AHRQ(Agency for Healthcare Research and Quality)31)
하였다. 상병이나 질환분류시 분석대상 호흡기계 상병 외의 호흡기계 타상병을 포함하는 경우는 제외하였다.
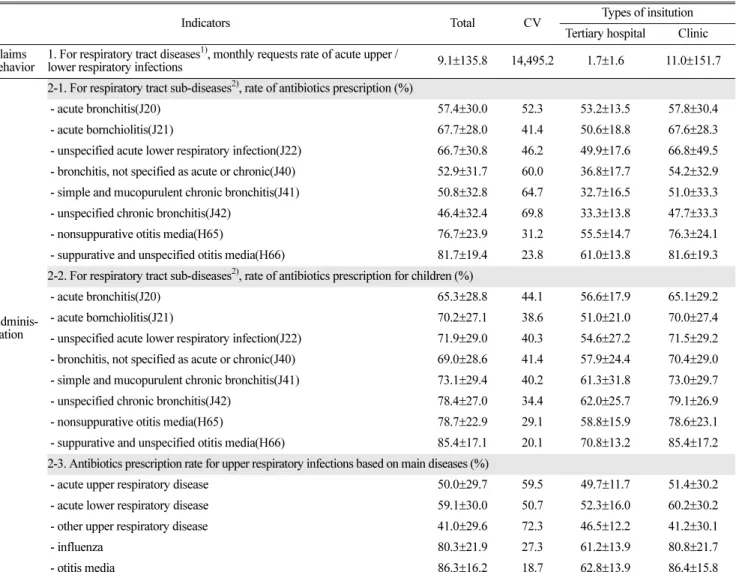
지표 2-2의 세부상병별 소아의 항생제 처방률은 외래 호흡 기계 질환을 주상병 혹은 부1상병으로 청구된 내역자료를 이용하여 산출하였다. 급성 기관지염(J20)에서 상급종합병원 의 경우 56.6%인데 비해, 병원 67.8%, 종합병원 67.6%, 의 원급 61.5%로 높게 나타났다. 급성 세기관지염(J21)에서도 상급종합병원이 51%인데 비해, 병원급이 79.9%로 가장 높 았고, 의원급 70%, 종합병원 69%로 병원급의 항생제 처방 률이 높게 나타났다.
지표 2-3의 주상병 기준 호흡기 감염 질환 분류별 항생제 처방률은 급성상기도감염에서 항생제 처방률은 종합병원이 53.3%로 가장 높게 나타났는데, 약제급여 적정성 평가에서 2008년 4/4분기 기준으로 의원급이 55.5%로 가장 높고, 병 원이 46.2%인데 비해서 큰 차이를 보이고 있다. 이는 분석 대상 호흡기계 상병 외의 호흡기계 타상병을 제외하였기 때 문인 것으로 판단된다.
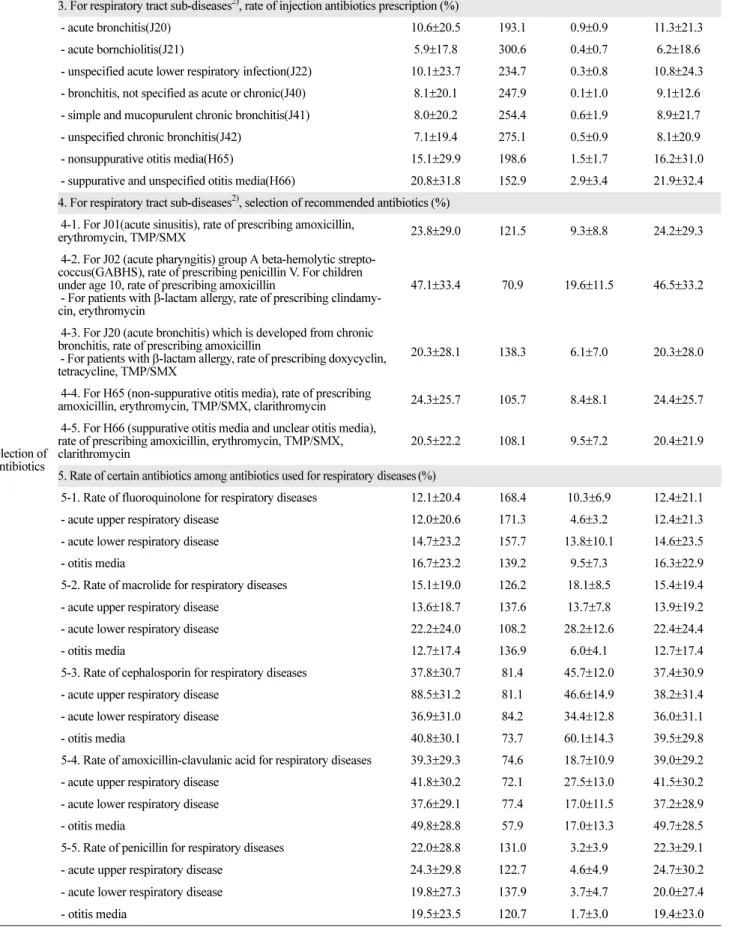
지표 4의 권고 항생제 선택에 대해서는 상급종합병원에서 가장 낮았고, 보건기관이 대체로 높게 나타났다. 급성 부비 동염의 경우 권고 항생제인 amoxicillin, erythromycin, TMP/
SMX 처방이 23.8%였고, 급성기관지염의 amoxicllin,
doxycycline, tetracycline, TMP/SMX 처방비율은 20.3%, 중이 염의 amoxicillin, erythromycin, TMP/SMX 처방비율은 약 20~24%로 낮았으나, 급성 인두염에서는 penicillinV, penicillinG benzathine, amoxicillin, clindamycin, erythromycin 처방비율이 47.1%였다. 그러나 β-lactam allergy가 있는 경우 사용해야 하는 clindamycin, erythrmycin을 allergy 여부를 판 단하지 않은 채 처방했을 가능성이 높으며, 전반적으로 권고 항생제 처방이 낮은 것으로 판단된다.지표 5의 특정 항생제 처방 비중에 있어서, fluoroquinolone의 비중이 급성 상기도 감염에서조차 12%로 높을 뿐만 아니라, 의원급에서 상급종 합병원 4.6%에 비해 12.4%로 상당히 빈번하게 처방하는 것 으로 나타났다. Macrolide도 비슷한데, 급성 상기도 감염에서 13.6%로 높고, 의원급이 13.9%로 더 높은 수준이었다. 반면, penicillin의 경우 급성상기도감염에서 의원급의 경우 24.7%
로 상급종합병원 4.6%에 비해 대체로 높은 수준이었다.
일일상용량(DDD)을 기준으로 한, 18세 이상 환자의 사용 량은 대체로 1미만으로 1일 상용량보다 적은 것으로 나타났 으며, 과소용량으로 투여되는 문제점이 나타났다.
호흡기 감염 질환에서 항생제 투여일수는 급성 기관지염은 2.9일로 호흡기 감염에 투여되는 항생제 사용기간 권고일수 인 7-10일에 못 미치는 것으로 나타났다.
Table 4. Delphi Results of Antibiotics Prescription for Respiratory Tract Diseases
code diagnosis
Wait-and see Proper use
3 points or higher
No. of Respondents
3 points or higher
No. of Respondents
J00 acute nasopharyngitis(common cold) 15 15 10 16
J01 acute sinusitis 5 15 12 16
J02 acute pharyngitis 13 15 13 16
J03 acute tonsilitis 6 15 12 16
J04 acute laryngitis and tracheitis 5 15 11 16
J05 acute obstructive laryngitis and epiglotitis 3 14 10 15
J06 acute upper respiratory infections of multiple and unspecified sites 13 15 14 16
J09 influenza due to identified avian influenza virus 12 14 10 15
J10 influenza due to other identified influenza virus 14 15 11 16
J11 influenza, virus not identified 12 15 13 16
J12 viral pneumonia, nec 9 15 14 16
J20 acute bronchitis 10 15 15 16
J21 acute bronchiolitis 8 15 12 16
J22 unspecified acute lower respiratory infection 6 15 14 16
J40 bronchitis, not specified as acute or chronic 9 15 13 16
J41 simple and mucopurulent chronic bronchitis 7 15 11 16
J42 unspecified chronic bronchitis 10 15 13 16
H65 nonsuppurative otitis media 10 14 12 15
H66 suppurative and unspecified otitis media 3 14 9 15
Table 5. Delphi Results of Antibiotics Prescribing Indicators for Respiratory Tract Diseases
Indicators Formula
Importance Need for Improvement 1 Round 2 Round 3
points or higher
No. of Respo ndents
3 points
or higher
No. of Respo ndents
3 points
or higher
No. of Respo ndents
Claims behav-
ior
1. For respiratory tract diseases1), monthly requests rate of acute upper / lower respiratory infections
Number of visits due to acute upper respiratory infection (J00-J06)
×100 9 16 9 16 7 10
Number of visits due to acute lower respiratory infection (J20-J22,J40-J42)
Admin- istration
2-1. For respiratory tract sub-diseases2), rate of antibiotics prescription
Total number of antibiotics prescriptions
×100 14 16 12 16 14 16
For relevant sub-diseases2), number of visits 2-2. For respiratory tract sub-diseases2),
rate of antibiotics prescription for chil- dren
Total number of antibiotics prescriptions
×100 13 15 12 15 14 15
For relevant sub-diseases2), number of visits of children under age 18
2-3. Antibiotics prescription rate for upper
respiratory infections based on main dis- eases
Total number of antibiotics prescriptions
×100 11 16 10 16 14 16
For main disease, number of visits
Selec- tion
of Antibi-
otics
3. For respiratory tract sub-diseases2), rate of injection antibiotics prescription
Total number of injection antibiotics prescriptions
×100 15 16 11 16 11 16
For relevant diseases2), number of visits 4. For respiratory tract sub-diseases2), selection of recommended antibiotics 4-1. For J01(acute sinusitis), rate of
prescribing amoxicillin, erythromycin, TMP/SMX
Total number of prescribing 1st choice antibiotics
×100
11 16 9 16 9 15
4-2. For J02 (acute pharyngitis) group A beta-hemolytic streptococ- cus(GABHS), rate of prescribing peni- cillin V. For children under age 10, rate of prescribing amoxicillin
- For patients with β-lactam allergy, rate of prescribing clindamycin, eryth- romycin
12 16 11 16 8 15
4-3. For J20 (acute bronchitis) which is developed from chronic bronchitis, rate of prescribing amoxicillin
- For patients with β-lactam allergy, rate of prescribing doxycyclin, tetracy- cline, TMP/SMX
9 16 9 16 9 15
4-4. For H65 (non-suppurative otitis media), rate of prescribing amoxicillin, erythromycin, TMP/SMX, clarithro- mycin
For relevant sub-diseases2), number of prescrip- tions
13 16 12 16 8 14
4-5. For H66 (suppurative otitis media and unclear otitis media), rate of prescribing amoxicillin, erythromycin, TMP/SMX, clarithromycin
13 16 11 16 10 14
5. Rate of certain antibiotics among antibiotics used for respiratory diseases1 5-1. Rate of fluoroquinolone for respi-
ratory diseases
Number of prescribing fluoroquinolone, mac- rolide, penicillin, amoxicillin-clavulanic acid,
cephalosporin
×100
11 16 12 16 11 15
5-2. Rate of macrolide for respiratory
diseases 12 16 9 16 12 15
5-3. Rate of cephalosporin for respira- tory diseases
For relevant sub-diseases2), number of p
rescribing antibiotics 7 16 9 16 11 16
5-4. Rate of amoxicillin-clavulanic
acid for respiratory diseases 13 16 11 16 11 16
5-5. Rate of penicillin for respiratory
diseases 13 16 11 16 10 16
Table 5. Delphi Results of Antibiotics Prescribing Indicators for Respiratory Tract Diseases(continued)
Antibi- otics
Use
6. Dose for patients with age 18 or older based on the DDD(Defined Daily Dose)
Sum of defined daily doses
×100 13 16 11 16 10 16
For relevant sub-diseases2), number of prescribing antibiotics with age 18 or older
patients Admin-
istra- tion days and number
7. Number of administration days for respiratory diseases1)
Number of administration days
×100 14 16 13 16 15 16
For relevant sub-diseases2), number of visits for diseases2)
8. Number of antibiotics for respiratory diseases1)
Number of antibiotics
×100 12 16 12 16 11 16
For relevant sub-diseases2), number of visits for diseases2)
Cost moni- toring
9. Cost of each antibiotics for respira- tory diseases1)
Cost of antibiotics
11 16 9 16 8 16
For relevant sub-diseases2), number of antibiotics
10. Cost of antibiotics against adminis- tration days for respiratory diseases1)
Cost of antibiotics
12 16 9 16 10 16
For relevant sub-diseases2), administration days of anti- biotics
Note: 1) Respiratory diseases are J00~J06, J20~J22, J40~J42, H65~H67 for main diseases and sub-diseases 1.
2) Based on 2-digit diseases in the fifth revision of Korea's standard cause of death classification 3) Recommended antibiotics use standards in table 4 are the same as table 2.
* Index 6 is excluded from the 2nd investigation
** Standard deviation or dispersion are used to see data distribution. However, as they increase if the mean becomes bigger, to correct this, the fluctuation index is calculated by dividing dispersion by mean.
Table 6. Result of Antibiotics Prescribing Indicators for Respiratory Tract Diseases
Indicators Total CV Types of insitution
Tertiary hospital Clinic Claims
behavior
1. For respiratory tract diseases1), monthly requests rate of acute upper /
lower respiratory infections 9.1±135.8 14,495.2 1.7±1.6 11.0±151.7
Adminis- tration
2-1. For respiratory tract sub-diseases2), rate of antibiotics prescription (%)
- acute bronchitis(J20) 57.4±30.0 52.3 53.2±13.5 57.8±30.4
- acute bornchiolitis(J21) 67.7±28.0 41.4 50.6±18.8 67.6±28.3
- unspecified acute lower respiratory infection(J22) 66.7±30.8 46.2 49.9±17.6 66.8±49.5 - bronchitis, not specified as acute or chronic(J40) 52.9±31.7 60.0 36.8±17.7 54.2±32.9 - simple and mucopurulent chronic bronchitis(J41) 50.8±32.8 64.7 32.7±16.5 51.0±33.3
- unspecified chronic bronchitis(J42) 46.4±32.4 69.8 33.3±13.8 47.7±33.3
- nonsuppurative otitis media(H65) 76.7±23.9 31.2 55.5±14.7 76.3±24.1
- suppurative and unspecified otitis media(H66) 81.7±19.4 23.8 61.0±13.8 81.6±19.3
2-2. For respiratory tract sub-diseases2), rate of antibiotics prescription for children (%)
- acute bronchitis(J20) 65.3±28.8 44.1 56.6±17.9 65.1±29.2
- acute bornchiolitis(J21) 70.2±27.1 38.6 51.0±21.0 70.0±27.4
- unspecified acute lower respiratory infection(J22) 71.9±29.0 40.3 54.6±27.2 71.5±29.2 - bronchitis, not specified as acute or chronic(J40) 69.0±28.6 41.4 57.9±24.4 70.4±29.0 - simple and mucopurulent chronic bronchitis(J41) 73.1±29.4 40.2 61.3±31.8 73.0±29.7
- unspecified chronic bronchitis(J42) 78.4±27.0 34.4 62.0±25.7 79.1±26.9
- nonsuppurative otitis media(H65) 78.7±22.9 29.1 58.8±15.9 78.6±23.1
- suppurative and unspecified otitis media(H66) 85.4±17.1 20.1 70.8±13.2 85.4±17.2 2-3. Antibiotics prescription rate for upper respiratory infections based on main diseases (%)
- acute upper respiratory disease 50.0±29.7 59.5 49.7±11.7 51.4±30.2
- acute lower respiratory disease 59.1±30.0 50.7 52.3±16.0 60.2±30.2
- other upper respiratory disease 41.0±29.6 72.3 46.5±12.2 41.2±30.1
- influenza 80.3±21.9 27.3 61.2±13.9 80.8±21.7
- otitis media 86.3±16.2 18.7 62.8±13.9 86.4±15.8
Table 6. Result of Antibiotics Prescribing Indicators for Respiratory Tract Diseases(continued)
Selection of Antibiotics
3. For respiratory tract sub-diseases2), rate of injection antibiotics prescription (%)
- acute bronchitis(J20) 10.6±20.5 193.1 0.9±0.9 11.3±21.3
- acute bornchiolitis(J21) 5.9±17.8 300.6 0.4±0.7 6.2±18.6
- unspecified acute lower respiratory infection(J22) 10.1±23.7 234.7 0.3±0.8 10.8±24.3 - bronchitis, not specified as acute or chronic(J40) 8.1±20.1 247.9 0.1±1.0 9.1±12.6 - simple and mucopurulent chronic bronchitis(J41) 8.0±20.2 254.4 0.6±1.9 8.9±21.7
- unspecified chronic bronchitis(J42) 7.1±19.4 275.1 0.5±0.9 8.1±20.9
- nonsuppurative otitis media(H65) 15.1±29.9 198.6 1.5±1.7 16.2±31.0
- suppurative and unspecified otitis media(H66) 20.8±31.8 152.9 2.9±3.4 21.9±32.4 4. For respiratory tract sub-diseases2), selection of recommended antibiotics (%)
4-1. For J01(acute sinusitis), rate of prescribing amoxicillin,
erythromycin, TMP/SMX 23.8±29.0 121.5 9.3±8.8 24.2±29.3
4-2. For J02 (acute pharyngitis) group A beta-hemolytic strepto- coccus(GABHS), rate of prescribing penicillin V. For children under age 10, rate of prescribing amoxicillin
- For patients with β-lactam allergy, rate of prescribing clindamy- cin, erythromycin
47.1±33.4 70.9 19.6±11.5 46.5±33.2
4-3. For J20 (acute bronchitis) which is developed from chronic bronchitis, rate of prescribing amoxicillin
- For patients with β-lactam allergy, rate of prescribing doxycyclin, tetracycline, TMP/SMX
20.3±28.1 138.3 6.1±7.0 20.3±28.0
4-4. For H65 (non-suppurative otitis media), rate of prescribing
amoxicillin, erythromycin, TMP/SMX, clarithromycin 24.3±25.7 105.7 8.4±8.1 24.4±25.7 4-5. For H66 (suppurative otitis media and unclear otitis media),
rate of prescribing amoxicillin, erythromycin, TMP/SMX, clarithromycin
20.5±22.2 108.1 9.5±7.2 20.4±21.9
5. Rate of certain antibiotics among antibiotics used for respiratory diseases(%)
5-1. Rate of fluoroquinolone for respiratory diseases 12.1±20.4 168.4 10.3±6.9 12.4±21.1
- acute upper respiratory disease 12.0±20.6 171.3 4.6±3.2 12.4±21.3
- acute lower respiratory disease 14.7±23.2 157.7 13.8±10.1 14.6±23.5
- otitis media 16.7±23.2 139.2 9.5±7.3 16.3±22.9
5-2. Rate of macrolide for respiratory diseases 15.1±19.0 126.2 18.1±8.5 15.4±19.4
- acute upper respiratory disease 13.6±18.7 137.6 13.7±7.8 13.9±19.2
- acute lower respiratory disease 22.2±24.0 108.2 28.2±12.6 22.4±24.4
- otitis media 12.7±17.4 136.9 6.0±4.1 12.7±17.4
5-3. Rate of cephalosporin for respiratory diseases 37.8±30.7 81.4 45.7±12.0 37.4±30.9
- acute upper respiratory disease 88.5±31.2 81.1 46.6±14.9 38.2±31.4
- acute lower respiratory disease 36.9±31.0 84.2 34.4±12.8 36.0±31.1
- otitis media 40.8±30.1 73.7 60.1±14.3 39.5±29.8
5-4. Rate of amoxicillin-clavulanic acid for respiratory diseases 39.3±29.3 74.6 18.7±10.9 39.0±29.2
- acute upper respiratory disease 41.8±30.2 72.1 27.5±13.0 41.5±30.2
- acute lower respiratory disease 37.6±29.1 77.4 17.0±11.5 37.2±28.9
- otitis media 49.8±28.8 57.9 17.0±13.3 49.7±28.5
5-5. Rate of penicillin for respiratory diseases 22.0±28.8 131.0 3.2±3.9 22.3±29.1
- acute upper respiratory disease 24.3±29.8 122.7 4.6±4.9 24.7±30.2
- acute lower respiratory disease 19.8±27.3 137.9 3.7±4.7 20.0±27.4
- otitis media 19.5±23.5 120.7 1.7±3.0 19.4±23.0
Table 6. Result of Antibiotics Prescribing Indicators for Respiratory Tract Diseases(continued)
Antibiotics Use
6. Patient episodes with prescribing antibiotics for respiratory diseases1) (DDD/1,000 /population/day)
- acute bronchitis(J20) 0.84±0.31 36.8 0.87±0.15 0.84±0.28
- acute bornchiolitis(J21) 0.83±0.31 36.8 0.81±0.21 0.83±0.30
- unspecified acute lower respiratory infection(J22) 0.83±0.27 32.0 0.89±0.22 0.83±0.26 - bronchitis, not specified as acute or chronic(J40) 0.83±0.28 33.7 0.83±0.20 0.83±0.28 - simple and mucopurulent chronic bronchitis(J41) 0.82±0.28 34.2 0.75±0.29 0.82±0.28 - unspecified chronic bronchitis(J42) 0.82±0.30 36.6 0.78±0.18 0.82±0.30
- nonsuppurative otitis media(H65) 0.81±0.29 35.2 0.64±0.14 0.81±0.28
- suppurative and unspecified otitis media(H66) 0.82±0.30 36.2 0.62±0.15 0.82±0.30
Administration days and
number
7-1. Number of administration days for respiratory diseases1) (day)
- acute bronchitis(J20) 2.9±1.4 48.7 4.4±1.3 2.9±1.3
- acute bornchiolitis(J21) 2.7±1.2 43.7 4.5±3.2 2.7±0.9
- unspecified acute lower respiratory infection(J22) 3.0±1.7 56.8 6.7±4.3 2.9±1.3 - bronchitis, not specified as acute or chronic(J40) 3.3±2.2 66.5 7.2 ± 3.9 3.3±2.1 - simple and mucopurulent chronic bronchitis(J41) 4.5±4.5 100.2 9.2±6.4 4.5±4.4
- unspecified chronic bronchitis(J42) 4.7±4.3 92.7 10.4±6.5 4.6±4.3
- nonsuppurative otitis media(H65) 3.0±1.6 51.8 4.7±1.2 3.0±1.4
- suppurative and unspecified otitis media(H66) 3.0±1.7 57.6 4.1±1.4 3.0±1.6 7-2. Number of administration days for respiratory diseases1) (day)
- acute upper respiratory disease 3.0±1.3 43.4 4.5±1.0 2.9±1.2
- acute lower respiratory disease 3.1±1.6 51.0 5.7±3.1 3.0±1.4
- other upper respiratory disease 3.4±1.7 49.4 7.4±1.4 3.3±1.5
- influenza 3.0±2.1 69.7 5.9±2.2 3.0±2.0
- otitis media 3.0±1.6 53.4 4.3±1.3 3.0±1.4
8. Number of antibiotics for respiratory diseases1) (단위: items)
- acute bronchitis(J20) 1.1±0.2 19.7 0.9±0.1 1.1±0.2
- acute bornchiolitis(J21) 1.0±0.2 18.8 0.8±0.1 1.1±0.2
- unspecified acute lower respiratory infection(J22) 1.1±0.2 22.4 0.9±0.1 1.1±0.2 - bronchitis, not specified as acute or chronic(J40) 1.0±0.3 24.4 0.8±0.1 1.1±0.2 - simple and mucopurulent chronic bronchitis(J41) 1.1±0.3 25.4 0.9±0.2 1.1±0.2
- unspecified chronic bronchitis(J42) 1.1±0.3 25.2 0.8±0.1 1.1±0.2
- nonsuppurative otitis media(H65) 1.1±0.3 25.6 0.8±0.1 1.2±0.3
- suppurative and unspecified otitis media(H66) 1.2±0.3 25.3 0.8±0.1 1.2±0.3
Cost monitoring
9. Cost of each antibiotics for respiratory diseases1) (KRW)
- acute upper respiratory disease 4,321±14,248 329.7 15,658±2,977 4,072±15,036 - acute lower respiratory disease 4,550±3,824 84.0 18,797±8,156 4,201±3,505 - other upper respiratory disease 4,790±3,998 83.5 23,892±8,392 4,396±3,284
- influenza 6,362±5,840 91.8 24,809±9,502 5,721±5,104
- otitis media 5,175±22,122 427.5 18,981±4,619 4,873±23,170
10. Cost of antibiotics against administration days for respiratory diseases1) (KRW)
- acute upper respiratory disease 1,355±2,842 209.7 2,401±218 1,322±3,005
- acute lower respiratory disease 1,376±603 43.8 2,350±419 1,335±578
- other upper respiratory disease 1,403±607 43.3 2,677±320 1,361±580
- influenza 1,887±876 46.4 2,944±441 1,831±845
- otitis media 1,528±2,825 184.9 2,411±399 1,503±2,964