ORIGINAL ARTICLE
JMBSJournal of Metabolic and Bariatric Surgery J Metab Bariatr Surg 2012;1(1):55-60
투고일: 2012년 3월 15일, 심사일: 2012년 5월 10일, 게재확정일: 2012년 5월 28일 책임저자: 박도중, 성남시 분당구 구미로 166번지
분당서울대학교병원 외과 우: 463-802
Tel: 031-787-7097, Fax: 031-787-4055, E-mail: [email protected]
*이 논문은 분당서울대학교병원 일반연구비(grant no 02-2010-038)에 의해 이루어진 것임.
당뇨비만 쥐 모델에서 루와이 위우회술과 위절제를 같이 시행한 루와이 위우회술 후 위장관 호르몬 변화의 비교 연구
1서울대학교 의과대학 외과학교실, 2분당서울대학교병원 외과
이주희2, 안상훈2, 손상용2, 이창민2, 박도중1,2, 김형호1,2
Comparison of Changes in Gastrointestinal Hormones after Conventional
Roux-en Y Gastric Bypass versus Near Total Gastrectomy with Roux-en Y Gastric Bypass in Diabetes and Obesity Rat Model
Ju Hee Lee2, Sang Hoon Ahn2, Sang-Yong Son2, Chang Min Lee2, Do Joong Park1,2, Hyung-Ho Kim1,2
Department of Surgery, 1Seoul National University College of Medicine, Seoul, 2Seoul National University Bundang Hospital, Seongnam, Korea Purpose: Roux-en Y gastric bypass (RYGBP) surgery is effective and used worldwide for treating morbid obese patients.
In Korea, RYGBP has not performed popularly due to relatively high incidence of gastric cancer because that procedure has a limitation of difficulty surveillance of remnant stomach after surgery. The aim of this study was to compare conventional RYGBP with RYGBP with near total gastrectomy (NTG) in terms of changes of gastrointestinal hormone and complications in diabetes and obesity rat model. Materials and Methods: Four ZDF/CrlCrlj-Leprfa/Leprfa (Fatty) rats were used (2 rats for each group). Changes in body weight, fasting glucose, and the serum concentrations of insulin, ghrelin, and peptide YY (PYY) were measured. Results: Body weight was decreased by 2 weeks after surgery in all rats, and maintained thereafter. All showed improved fasting glucose, but that was more improved in RYGBP with NTG group without statistically significance. Insulin declined by 69.1% and 42.8% in RYGBP and NTG with RYGBP group, respectively. Ghrelin increased by 46.5% and 27.45% and PYY by 19.58% and 24.56%. There was no operation related complication on necropsy at 4 weeks after surgery. Conclusion: Postoperative outcomes after NTG with RYGBP were comparable to those after RYGBP and glucose control after NTG with RYGBP seems to be better than that after RYGBP in this animal study. Future clinical studies in humans are warranted.
Key Words: Roux-en Y gastric bypass, Near total gastrectomy with Roux-en Y gastric bypass, Diabetes and obesity rat model, Ghrelin, Peptide YY
서론
비만 인구의 비율은 전세계적으로 급증하고 있는 추세이며 국
내의 경우 2007년도 국민건강 영양조사 중간결과 발표에 따르 면 19세 이상의 성인에서 체질량지수(body mass index, BMI) 가 25 (kg/m2) 이상인 인구는 31.7%로 10년간 5.7% 증가하였으
Fig. 1. (A) Roux-en Y gastric bypass. Distal stomach (white arrow).
(B) Roux-en Y gastric bypass with near total gastrectomy.
Gastrojejunostomy (big arrow), jejunojejunostomy (small arrow).
며, 체질량지수가 30 (kg/m2) 이상인 인구는 4.1%로 10년간 1.8% 증가하였다.(1) 비만 환자에게 있어서 비만 수술로 인한 적 절한 체중 감량은 삶의 질 개선, 비만과 관련된 동반질환 개선, 수 명 연장을 가져다 주는 것으로 이미 여러 문헌에서 발표되었다.
현재 복강경 루와이 우회술이 수술의 효율성과 안정성을 보편적 으로 만족시켜 세계적으로 가장 널리 시행되고 있는 수술이다.
이 방법은 몸무게의 감소뿐만 아니라 당뇨, 혈압 등의 비만 관련 합병증의 치료에도 탁월한 효과가 입증되어 왔다.(2,3) 이런 치 유 효과는 수술 후 위장관 호르몬(Ghrelin, PYY, GLP-1 등)의 변화가 큰 역할을 하는 것으로 알려져 있다.(4) 그러나 남은 위를 내시경 등의 검진 방법으로 경과를 관찰하기 어렵다는 단점이 있 다. 이런 단점이 우리나라 같은 위암 발생률이 높은 지역에서는 루와이 우회술 시행의 제한점이 될 수 있다.
본 연구를 통해 남은 위의 절제를 같이 시행하는 경우와 전통 적 루와이 우회술을 시행한 후 호르몬의 변화와 수술 후 합병증 발생을 비교하여 비만이나 비만 관련 합병증을 갖고 있는 환자를 대상으로 시행하는 수술 방법의 더 나은 접근 방법을 확립하고자 하였다.
재료 및 방법
1. 실험 동물의 준비와 수술
식이 유도 당뇨, 비만 쥐(ZDF/CrlCrlj-Leprfa/Leprfa (Fatty) rats)를 이용하여 실험을 시행하였다. 6주령 수컷 4마리를 분양 받은 후, 당뇨와 비만 유도를 위해12주까지 특수 사료(Purina
#5008)을 먹여 사육한 후, 증상(polyphagia, polydipsia, po- lyuria)으로 당뇨가 형성됨을 확인하고 실험을 시행하였다. 이 동물 실험은 분당서울대학교병원 동물 실험위원회의 승인을 받 았으며, 실험지침을 준수하였다.
각각 두 마리씩 두 그룹으로 나누어 두 마리에서 Xu 등(5)이 기 술한 방법을 수정하여 루와이 우회술을, 나머지 두 마리에서는 루와이 우회술과 동시에 남은 위의 절제술을 시행하였다. 수술 전날 밤 금식시킨 후 마취 전 무게를 측정하고, isoflurane (1.5-3.0%)을 이용하여 전신마취를 시켰다. 예방적 항생제로 Cefazolin 50 mg/kg을 피하 주사한 후, 수술 부위를 povi- done-iodine solution으로 소독한 뒤 복부 정중선 절개를 하여 개복하였다. 루와이 우회술을 위해 우선 endoscopic linear staplers (Echelon flex 60-3.5; Ethicon Endo-Surgery, Cin- cinnati, OH, USA)을 이용하여 전체 위의 20% 용적이 남게 위를 절단하였다. 다음으로 40 cm biliopancreatic limb, 15 cm Roux-en Y limb, 25 cm common channel을 형성하기 위해 소장을 절단하였다. 위-공장 문합술과 공장-공장 문합술은 5-0 단일성 흡수 봉합사를 이용하여 시행한 후 3-0 비 흡수성 봉합사
로 복부 정중선을 봉합한 후 수술을 종료하였다(Fig. 1A). 두 마 리에서는 상기 루와이 우회술에 남은 위 절제술을 동시에 시행하 였다(Fig. 1B). 모든 쥐에서 수술 후 다음날은 금식한 후 수술 후 2일째부터 물을 섭취하도록 하였다. 그 다음날부터 사료를 분쇄 하여 물과 섞어 공급하였고, 4일째부터 일반 사료를 공급하였다.
2. 공복시 혈당, 체중, 혈청 인슐린, 그렐린 및 PYY 측정 공복 시 혈당은 8시간 금식시킨 후 수술 전과 수술 후 1주 간격 으로 꼬리를 잘라 혈당 측정용 스틱과 glucometer를 이용하여 측정하였다. 체중도 수술 전과 수술 후 1주 간격으로 측정하였 다.
혈청 인슐린, 그렐린과 PYY 측정을 위해 수술 전에는 마취 하 에 꼬리 정맥에서 혈액을 채취하였으며, 4주째에는 8시간 금식 시킨 후 희생시키기 전에 전신 마취하에 대정맥에서 채취하였 다. 채취한 샘플은 EDTA 용기에 수집하여 바로 혈청을 원심 분 리하였으며, 검사 전까지 −70oC에서 보관하였다. 모든 혈액 채 취가 끝난 후 혈청 인슐린, 그렐린과 PYY 수치 측정을 위해 인슐 린 ELISA 키트(Mercodia Rat Insulin ELISA, Uppsala, Sweden), 그렐린 ELISA 키트(Rat/Mouse Ghrelin (total) ELISA, Millipore Corporation, Billerica, MA, USA), PYY ELISA 키트(Rat PYY EIA Kit, Sceti K.K., Tokyo, Japan)을 이 용하여 각각 이중으로 중복 측정하여 평균치를 구하였다.
3. 통계분석
두 그룹 간의 비교는 Mann-Whitney U test를 이용하였다.
결과
평균 수술 시간은 루와이 우회술 군이 70분, 위절제술 군이 75 분이었다. 수술 전 평균 체중은 루와이 우회술 군과 위절제술 군
Table 1. Pre- and postoperative levels of weight and fasting glucose in the Roux-en Y bypass (RYGBP) and Roux en Y bypass with near total gastrectomy (NTG) groups
RYGBP NTG P
Weight
Preoperative 333.5 333.5 1.000
1 week 284.5 280.5 1.000
2 weeks 260.5 262.5 0.683
3 weeks 255 266.5 0.439
4 weeks 254.5 281 0.439
Fasting glucose
Preoperative 538 493.5 0.439
1 week 229 135 0.121
2 weeks 210.5 153 0.121
3 weeks 202.5 141 0.121
4 weeks 212.5 139.5 0.121
Fig. 2. Postoperative weight changes between two groups. Fig. 3. Fasting glucose was more improved in Roux en Y gastric bypass with near total gastrectomy group, but there were no significant differences between two groups.
모두 333.5 g (range, 327-340 g)이었다. 수술 후 모든 쥐가 체 중 감소를 보였으며, 수술 후 2주까지 급격히 감소한 후 이후 안 정화되었다. 각 그룹 수술 전후 평균 체중의 변화를 보았을 때 루 와이 우회술 군이 더 많은 체중 감소를 보였으나(Fig. 2) 통계적 차이는 보이지 않았다(Table 1).
수술 전 공복시 혈당은 모든 쥐에서 400 mg/dl (range, 438-600 mg/dl) 이상이었으며, 수술 후 1주에 측정했을 때 급 격한 감소하였다. 두 그룹간의 수술 전후 공복시 혈당을 비교하 였을 때, 유의한 차이는 없었으나(Table 1), 수술 일주일 후부터 희생시킬 때까지 루와이 우회술 군은 모두 200 이상을 유지한 반 면, 위절제술 군은 모드 140 이하로 유지되었다(Fig. 3).
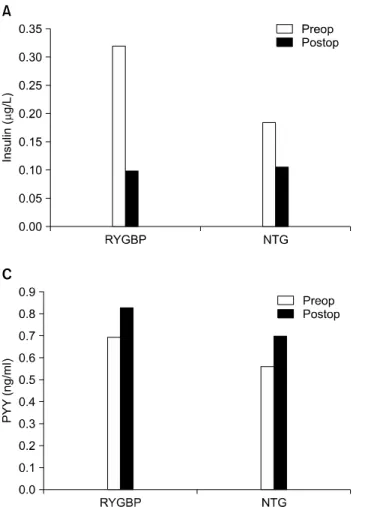
수술 전 평균 인슐린 농도는 루와이 우회술 군은 0.3186μg/L 였고, 위절제술 군은 0.18415μg/L였다. 수술 후 4주째 모든 쥐 에서 혈중 인슐린 농도는 감소하였으며, 루와이 우회술 군은 69.1%, 위절제술 군은 42.8% 감소하였으며, 수술 후 인슐린 농
도는 루와이 군이 0.09825μg/L과 위절제술 군이 0.1054μg/L 로 두 그룹에서 비슷하였다(Fig. 4A). 그렐린과 PYY는 모든 쥐에 서 수술 후 증가하였으며, 그렐린은 수술 후 루와이 우회술 군이 46.5%, 위절제술 군이 27.45% 증가하였으며, PYY는 수술 후 루 와이 우회술 군이 19.58%, 위절제술 군은 24.56% 증가하였다 (Fig. 4B, C).
네 마리 모두 수술 후 4주째까지 생존하였으며, 4주 후 희생시 켰을 때 약간의 장유착을 제외하고 문합부 협착이나 누출, 소장 의 확장과 괴사 같은 다른 합병증은 발견되지 않았다.
고찰
비만 수술방법은 크게 제한수술(restrictive procedure)과 흡 수장애 수술(malabsorptive procedure)로 나눌 수 있다. 현재 시행되고 있는 수술 중에 제한수술의 대표적인 것으로는 위밴드 술(Gastric Banding)을 들 수 있고, 흡수장애 수술로 대표적인 것은 췌담류 전환술(Bilopancreatic Diversion, BPD)을 들 수 있다. 루와이 위 우회술(Roux en Y gastric bypass)은 위의 근위 부에 작은 위낭을 만들고, 공장의 대부분을 우회시키는 것으로 상기 두 술식의 중간쯤의 형태로서 그 장단점을 함께 한다고 생 각할 수 있다. 1970년대 처음 개발된 이후 여러 가지 변형과 개선 이 이루어지면서 현재와 같은 수술법이 되었다.(6) 루와이 위 우 회술은 효과가 뛰어나고 수술의 합병증이 비교적 낮아, 비만 환 자에서 표준술식(Gold Standard)으로 인정받고 있다. 1990년 대 미국에서 Vertical banded gastroplasty (VBG)와 함께 가장 많이 하는 수술이었는데 VGB는 복강경 위밴드술이 나온 이후에 없어지게 되었으나 루와이 위 우회술은 80% 이상의 환자에 사용 될 정도로 미국에서 표준 수술로 자리 잡았다.(7) 게다가 동반 질
Fig. 4. Changes of insulin (A), Ghrelin (B), and PYY (C) levels.
Insulin declined by 69.1% and 42.8% in RYGBP and NTG with RYGBP group, respectively. Ghrelin increased by 46.5% and 27.45% and PYY by 19.58% and 24.56%.
환으로 제2형 당뇨병이 있던 비만 환자에게서 루와이 위 우회술 이후 체중 감소와 더불어 제2형 당뇨병의 개선 및 완전 관해에 대 한 많은 연구가 보고 되고 있어 대사 수술(metabolic surgery)로 서도 자리 잡고 있다.(2,3) 우리나라의 경우 2005년 대한민국의 20세 이상 성인 비만 유병률은 31.8%였고 매년 비만환자가 증가 하고 있으며 최근 수술적 치료를 고려해야 하는 고도 비만 환자 도 증가되고 있다.(8) 하지만, 우리나라의 경우 위암 발생률이 높 아 수술 후 남은 위의 검진이 불가능한 루와이 우회술은 비만 환 자에서의 적용에 문제점의 하나로 인식되고 있다. 그래서 위암 에서의 많은 위절제술의 경험을 갖고 있는 상부위장관 외과의들 의 경우, 루와이 우회술시 남은 원위부 위의 절제를 동시에 시행 하는 방법이 비만한 한국인에서 적용하기에 적절하지 않을까라 는 의문을 제시하게 되었다. 이에 남은 원위부 위의 절제가 합병 증을 증가시키지 않고 체중의 감소나 당뇨의 호전 등의 효과는 루와이 우회술과 같은지를 보기 위한 연구들이 필요하겠다. 이 를 평가하기 위해 본 실험을 수행하였고, 비록 증례수가 적고 동 물 실험이기는 하지만 원위부 위절제을 동시 시행한 경우도 합병 증 없이 같은 수의 쥐에서 생존이 가능하였으며, 체중의 감소나 공복시 혈당의 호전, 호르몬의 변화 등에서 루와이 우회술 군과
차이가 없음을 관찰할 수 있었다.
비만의 조절기전에는 여러 가지 호르몬과 펩티드가 관련 되어 있으며 그 중 그렐린(ghrelin)을 비롯하여 렙틴(leptin), poly- peptide YY3-36 (PYY3-36), glucagon-like peptide-1 등이 있는 것으로 알려져 있다.(4) 루와이 위우회술 후 일어나는 체중감량 에 대해 내분비 기전에 대해 많은 연구가 진행되고 있으나 아직 정확한 이유는 설명되어지지 않고 있다. 이 중 그렐린은 알려진 유일한 식욕 촉진 호르몬이며 비만 환자에서 루와이 우회술 후 감소하여 수술 후 체중 조절에 관여하는 것으로 많은 연구자들이 보고하고 있다.(9-11) 반면에, 본 동물 실험에서는 루와이 우회 술과 위절제술 군 모두 수술 후 4주째 측정한 그렐린이 수술전보 다 모두 증가되었다. 하지만 모든 쥐에서 체중 감소가 이루어졌 으며, 이는 66명의 비만환자에서 루와이 우회술 전후 그렐린을 측정하였을 때 6개월째 44%, 12개월째 62% 그렐린이 증가되었 다고 보고한 Holdstock 등(12)의 결과와 상응한다. 또한 Cummings 등(9)은 식이와 운동 등에 의해 체중 조절에 성공한 비만환자들에서는 그렐린 농도가 체중 감소 전보다 증가되었었 다고 보고하고 있다. 체중 조절에 그렐린의 역할에 대해서는 좀 더 많은 연구와 논의가 필요하겠다.
비만의 또 다른 기전으로는 PYY가 관여되어 있는 것으로 알 려져 있다. PYY는 식후 장의 L 세포에서 분비되며,(13,14) PYY 의 분비는 배고픔을 줄이고 포만감을 증가시킨다.(15) PYY를 주 사한 경우 정상 체중 환자뿐 아니라 비만 환자에서도 칼로리 섭 취를 줄이고 배고픔을 감소시켰다는 보고가 있다.(16,17) 게다 가 공복 시와 식후 PYY의 농도가 정상인 환자에서는 높은 반 면,(17) 비만한 환자에서는 감소되어 있었다고 보고되고 있어서 비만의 원인의 하나로 제시되기도 했지만,(18) 그렇지 않은 보고 도 있어 더 많은 연구가 필요한 상황이다.(19,20) 일반적으로 루 와이 우회술 후 PYY 농도는 수술 전보다 증가하는 것으로 알려 져 있다.(21,22) 또한 루와이 수술 후 몇 해 동안 증가 되어 있어 장기간 체중을 유지하는데도 관여하는 것으로 생각 되고 있 다.(21-24) 본 연구에서도 수술 후 모든 쥐에서 증가된 소견을 보 여 이전의 보고들과 같은 결과를 보였다. 또한 수술 후 2주 후부 터 감소된 체중이 유지됨을 확인하여, 여러 동물 실험들의 결과 와 마찬가지로 이 호르몬이 식욕 감퇴를 유발하여 감소된 체중을 유지하는 역할을 하고 있다는 것을 확인할 수 있었다.(25-27)
비만 수술 후 제 2형 당뇨의 개선 및 완전 관해는 Buchwald 등 (28)에 의하면 VGB, 위밴드술, 루와이 우회술, 췌담도 전환술의 순서로 71.6%, 47.9%, 83.7%, 98.9%로 보고되었다. 최근, 당뇨 병이 개선되는 시기가 수술 후 며칠 이내, 즉 체중 감소가 별로 없 는 시기에 생긴다는 것에 주목하였고, 이에 십이지장과 근위 공 장의 우회가 당뇨를 호전시킨다는 “foregut theory”와 회장으 로의 소화되지 않은 음식물의 통과가 L 세포를 자극하여 장 펩티 드의 분비를 증가시킨다는 “hindgut theory”가 제안되어 왔 다.(29) 본 연구에서도 원위부 위의 절제 여부와 상관 없이 우회 술을 시행했기 때문에 두 그룹의 모든 쥐에서 수술 후 초기(수술 후 1주)부터 수술 전보다 공복시 혈당이 호전됨을 관찰할 수 있 었고, 여러 동물이나 사람에서의 연구에서처럼 수술 후 인슐린 이 감소함을 관찰하여 수술 후 인슐린 저항성이 호전됨을 짐작할 수 있었다.(25,26,30) 하지만 증례 수가 적고 당뇨 조절 평가의 표준화된 방법인 oral glucose tolerance tes가 아니라 단순 공 복 혈당만을 측정 비교하였으며, 두 그룹의 수술 전 인슐린 농도 에 차이가 있어 두 그룹의 당뇨 진행 정도가 다를 것이라는 점이 두 그룹을 비교하는 본 연구의 제한 점이 되겠다.
결론
저자들은 본 실험을 통해 비록 증례 수는 적지만 루와이 우회 술 군과 위절제술 군이 비슷한 체중의 감소, 체중감소와 관련된 호르몬과 인슐린의 변화를 보임을 관찰할 수 있었고, 위절제술 군이 합병증의 증가 없이 수술 후 공복시 혈당 감소에 더 유리하 다는 것을 관찰할 수 있었다. 루와이 우회술과 원위부 위의 절제
를 시행하는 것이 위암의 발생률이 높은 우리나라에서는 비만과 비만 관련 합병증으로 수술을 시행 받는 환자들을 위한 표준 술 식으로 제시될 수 있을 것이다. 향후 환자를 대상으로 한 임상 연 구가 필요하겠다.
참고문헌
1. Available at: http://knhanes.cdc.go.kr/Accessed March 13, 2009 2. Schauer PR, Burguera B, Ikramuddin S, Cottam D, Gourash W,
Hamad G, Eid GM, Mattar S, Ramanathan R, Barinas-Mitchel E, et al. Effect of laparoscopic Roux-en Y gastric bypass on type 2 dia- betes mellitus. Ann Surg 2003;238:467-484.
3. Sugerman HJ, Wolfe LG, Sica DA, Clore JN. Diabetes and hyper- tension in severe obesity and effects of gastric bypass-induced weight loss. Ann Surg 2003;237:751-756.
4. Beckman LM, Beckman TR, Earthman CP. Changes in gastro- intestinal hormones and leptin after Roux-en-Y gastric bypass procedure: a review. J Am Diet Assoc 2010;110:571-584.
5. Xu Y, Ohinata K, Meguid MM, Marx W, Tada T, Chen C, Quinn R, Inui A. Gastric bypass model in the obese rat to study metabolic mechanisms of weight loss. J Surg Res 2002;107:56-63.
6. Hur Y. A review of bariatric surgery procedures and outcomes.
Korean J Obes 2008;17:141-153.
7. Huang CK, Shabbir A, Lo CH, Tai CM, Chen YS, Houng JY.
Laparoscopic Roux-en-Y gastric bypass for the treatment of type II diabetes mellitus in Chinese patients with body mass index of 25-35. Obes Surg 2011;21:1344-1349.
8. Kim KK. Pharmacotherapy for obesity. J Korean Med Assoc 2011;54:409-418.
9. Cummings DE, Weigle DS, Frayo RS, Breen PA, Ma MK, Dellinger EP, Purnell JQ. Plasma ghrelin levels after diet-induced weight loss or gastric bypass surgery. N Engl J Med 2002;346:1623-1630.
10. Engström BE, Ohrvall M, Sundbom M, Lind L, Karlsson FA. Meal suppression of circulating ghrelin is normalized in obese in- dividuals following gastric bypass surgery. Int J Obes (Lond) 2007;31:476-480.
11. Tritos NA, Mun E, Bertkau A, Grayson R, Maratos-Flier E, Goldfine A. Serum ghrelin levels in response to glucose load in obese sub- jects post-gastric bypass surgery. Obes Res 2003;11:919-924.
12. Holdstock C, Engström BE, Ohrvall M, Lind L, Sundbom M, Karlsson FA. Ghrelin and adipose tissue regulatory peptides: ef- fect of gastric bypass surgery in obese humans. J Clin Endocrinol Metab 2003;88:3177-3183.
13. Murphy KG, Bloom SR. Gut hormones and the regulation of en- ergy homeostasis. Nature 2006;444:854-859.
14. Cummings DE, Overduin J. Gastrointestinal regulation of food intake. J Clin Invest 2007;117:13-23.
15. Vincent RP, Ashrafian H, le Roux CW. Mechanisms of disease: the role of gastrointestinal hormones in appetite and obesity. Nat Clin Pract Gastroenterol Hepatol 2008;5:268-277.
16. Batterham RL, Cowley MA, Small CJ, Herzog H, Cohen MA, Dakin CL, Wren AM, Brynes AE, Low MJ, Ghatei MA, et al. Gut hormone PYY(3-36) physiologically inhibits food intake. Nature 2002;418:
650-654.
17. Batterham RL, Cohen MA, Ellis SM, Le Roux CW, Withers DJ, Frost
GS, Ghatei MA, Bloom SR. Inhibition of food intake in obese sub- jects by peptide YY3-36. N Engl J Med 2003;349:941-948.
18. le Roux CW, Batterham RL, Aylwin SJ, Patterson M, Borg CM, Wynne KJ, Kent A, Vincent RP, Gardiner J, Ghatei MA, et al.
Attenuated peptide YY release in obese subjects is associated with reduced satiety. Endocrinology 2006;147:3-8.
19. Kim BJ, Carlson OD, Jang HJ, Elahi D, Berry C, Egan JM. Peptide YY is secreted after oral glucose administration in a gender-specific manner. J Clin Endocrinol Metab 2005;90:6665-6671.
20. Stock S, Leichner P, Wong AC, Ghatei MA, Kieffer TJ, Bloom SR, Chanoine JP. Ghrelin, peptide YY, glucose-dependent in- sulinotropic polypeptide, and hunger responses to a mixed meal in anorexic, obese, and control female adolescents. J Clin Endocrinol Metab 2005;90:2161-2168.
21. le Roux CW, Aylwin SJ, Batterham RL, Borg CM, Coyle F, Prasad V, Shurey S, Ghatei MA, Patel AG, Bloom SR. Gut hormone profiles following bariatric surgery favor an anorectic state, facilitate weight loss, and improve metabolic parameters. Ann Surg 2006;
243:108-114.
22. Rodieux F, Giusti V, D'Alessio DA, Suter M, Tappy L. Effects of gas- tric bypass and gastric banding on glucose kinetics and gut hor- mone release. Obesity (Silver Spring) 2008;16:298-305.
23. Morínigo R, Vidal J, Lacy AM, Delgado S, Casamitjana R, Gomis R.
Circulating peptide YY, weight loss, and glucose homeostasis af- ter gastric bypass surgery in morbidly obese subjects. Ann Surg 2008;247:270-275.
24. Karamanakos SN, Vagenas K, Kalfarentzos F, Alexandrides TK.
Weight loss, appetite suppression, and changes in fasting and postprandial ghrelin and peptide-YY levels after Roux-en-Y gas- tric bypass and sleeve gastrectomy: a prospective, double blind study. Ann Surg 2008;247:401-407.
25. Shin AC, Zheng H, Townsend RL, Sigalet DL, Berthoud HR.
Meal-induced hormone responses in a rat model of Roux-en-Y gastric bypass surgery. Endocrinology 2010;151:1588-1597.
26. Meirelles K, Ahmed T, Culnan DM, Lynch CJ, Lang CH, Cooney RN. Mechanisms of glucose homeostasis after Roux-en-Y gastric bypass surgery in the obese, insulin-resistant Zucker rat. Ann Surg 2009;249:277-285.
27. Lee SK, Jung H, Jeon HM, Kim EK. Effect of roux-en-Y gastric by- pass on body weight, ghrelin and PYY(3-36) in diet-induced obese rats. J Korean Surg Soc 2010;79:155-162.
28. Buchwald H, Avidor Y, Braunwald E, Jensen MD, Pories W, Fahrbach K, Schoelles K. Bariatric surgery: a systematic review and meta-analysis. JAMA 2004;292:1724-1737.
29. Cummings DE, Overduin J, Foster-Schubert KE. Gastric bypass for obesity: mechanisms of weight loss and diabetes resolution. J Clin Endocrinol Metab 2004;89:2608-2615.
30. Korner J, Inabnet W, Conwell IM, Taveras C, Daud A, Olivero- Rivera L, Restuccia NL, Bessler M. Differential effects of gastric bypass and banding on circulating gut hormone and leptin levels.
Obesity (Silver Spring) 2006;14:1553-1561.