= 증례보고 = 접수번호 : 50-08-10-13
만성 중심성 장액맥락망막병증으로 오인되어 치료한 고령에서 발생한 베스트병 환자 1예
조원빈⋅신현진⋅문준웅⋅김형찬 건국대학교 의학전문대학원 안과학교실
목적: 특이한 임상양상을 보이는 고령의 베스트병 환자를 경험하였기에 이를 보고하고자 한다.
증례요약: 6개월의 스테로이드 복용력이 있는 68세 여자환자가 양안의 시력저하를 주소로 내원하였다. 안저검사에서 양안 황반에 1.5 유두지름 크기의 둥글게 융기된 병변을 보였으며, 빛간섭단층촬영에서 장액망막박리가 관찰되었으며, 형광안저혈관조영 및 인도시아닌 그린 형광조영술에서 망막색소상피박리 소견을 보여 맥락막신생혈관이 동반된 만성 중심성 장액맥락망막병증으로 진단하였다. 광역학요 법(PDT)과 유리체강내 아바스틴 주입술(IVB)의 병합치료를 시행하였으나 호전이 없었으며, 나중에 시행안 안전위도 검사에서 심하게 저 하된 소견을 보여 베스트병으로 진단하였다. Spectral domain 빛간섭단층촬영에서 망막색소상피의 갈라짐 및 그 사이의 저반사 소견을 보였다.
결론: 특이한 임상양상을 보이는 고령의 환자에서 심하게 저하된 안전위도 검사결과로 베스트병 진단을 내릴 수 있었고, spectral domain OCT에서 망막색소상피 갈라짐이 관찰되었으며, PDT 및 IVB 병합치료는 효과가 없었다.
<대한안과학회지 2009:50(8):1275-1281>
■ 접 수 일: 2008년 10월 20일 ■ 심사통과일: 2009년 5월 19일
■ 책 임 저 자: 김 형 찬
서울시 광진구 화양동 4-12번지 건국대학교병원 안과
Tel: 02-2030-5270, Fax: 02-2030-5273 E-mail: [email protected]
노른자모양 황반이영양증(vitelliform macular dystrophy) 은 1905년 Friedrich Best가 질병의 진행에 따른 각 단계를 기술하여 처음 보고 하여 흔히 베스트병이라고 부른다.1베 스트병은 VMD2 유전자의 돌연변이로 인해 망막색소상피 기저형질막의 칼슘-염소 채널 단백질인 베스트로핀 기능의 이상으로 망막색소상피를 통한 수분 이동의 장애가 생겨 장액망막박리 혹은 망막색소상피박리 등이 생길 수 있다.2 다양한 표현형을 갖는 상염색체 우성으로 유전되며, 안전위 도(electro-oculogram, EOG)는 특징적으로 정상 이하로 떨어지는데 발현되지 않은 무증상의 유전자 보인자 (carrier) 의 경우에도 정상 이하의 안전위도 검사결과를 보인다.3
베스트병의 안저소견은 그 진행단계에 따라5 단계로 나눌 수 있으며, 질병의 진행에 따라 점진적인 시력저하가 나타 나는 것이 보통이나, 맥락막신생혈관(choroidal neovascu- larization)이 동반되어 급격한 시력저하를 가져오는 경우 도 있다.4베스트병에 합병된 맥락막신생혈관의 치료로 광 역학요법(photodynamic therapy, PDT), 레이저광응고술, 유리체강내 아바스틴 주입술(intravitreal bevacizumab injection, IVB)이 효과적이었다는 보고는 있으나 아직까지
입증된 치료방법은 없다.5,6저자들은 양안 만성 중심성장액 맥락망막박리(chronic central serous chorioretinopathy) 로 오인하여 PDT 및 IVB를 시행하였던 고령의 노인에서 생긴 베스트병 환자를 경험하였기에 이를 보고하고자 한다.
증례보고
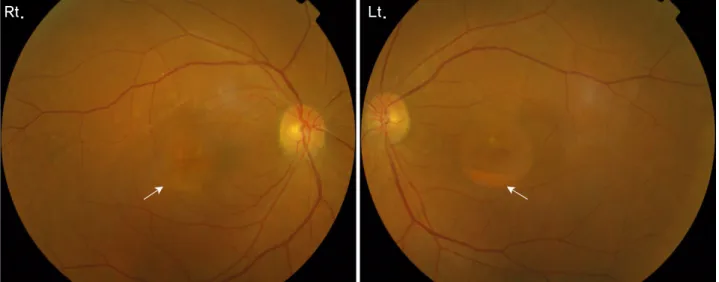
68세 여자환자로 수개월 전부터 시작된 양안의 시력저하를 주소로 내원하였다. 과거력에서 당뇨와 고혈압은 없었으며, 관절염으로 스테로이드를 장기간 복용한 병력이 있었으나 안과적 가족력은 없었다. 초진 시 교정시력은 우안 0.7, 좌안 0.6이었으며, 경미한 백내장 소견 외에 전안부 이상 소견은 없었다. 안저검사에서 양안에 경계가 분명한 약 1.5 유두지 름 크기의 중심와를 침범한 둥근 모양의 융기된 병변이 보 였다. 병변 하부에는 노란 망막하 침착물에 의한 수면(fluid level)이 관찰되었다(Fig. 1). 빛간섭단층촬영(stratus OCT;
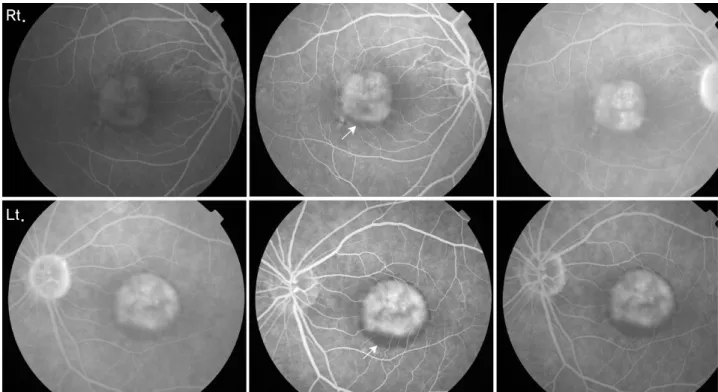
Carl Zeiss Meditec, Inc, Dublin, California, USA)에서 양안 모두 중심와오목은 소실되어 있고 고반사로 나타나는 망막 색소상피층과 감각신경망막 사이의 저반사 공간이 보이는 장액망막박리 소견을 보였으며, 노란 망막하 침착물은 감각 신경망막 하부의 고반사로 관찰되었다(Fig. 2). 형광안저혈 관조영(fluorescein angiography, FAG)에서 초기부터 경계 가 뚜렷한 균일한 과형광이 후기까지 지속되어 망막색소상 피박리에 의한 형광고임 소견을 보였으며, 노란색 망막하 침착물은 차단형광에 의한 저형광 소견을 보였다(Fig. 3).
Rt. Lt.
Figure 1. Fundus findings show a well-circumscribed, circular area of macula elevation in both eyes. Subretinal exudates with fluid levels in the inferior part of the lesion are seen in both eyes, more marked in the left eye (arrows).
Right
Left
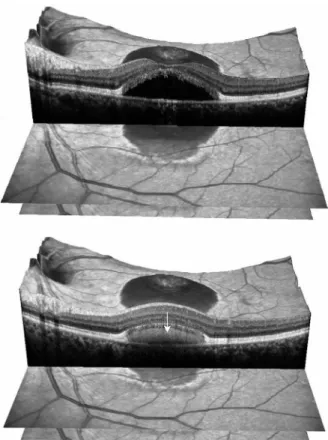
Figure 2.Optical coherenece tomography findings of both eyes show serous retinal detach- ment. High reflectivity areas corresponding to the outer retinal pigment epithelium band (arrows) are visible under the low reflective space. High reflectivity areas corresponding to subretinal exudates are also seen (arrow heads).
Rt.
Lt.
Figure 3. Fluorescein angiography findings of both eyes reveal well-defined hyperfluorescence in the early phase and persistent hyperfluoresence in the late phase, corresponding to pigment epithelial detachment. Blocked fluorescence due to subretinal exudates are also seen in both eyes, especially in the left eye (arrows).
Rt.
Lt.
Figure 4.Indocyanine green angiography findings of both eyes reveal well-demarcated early hyperfluorescence and persistent hyperfluorescence in the late phase, corresponding to pigment epithelial detachment. Large choroidal vessels (arrows) are visible under pigment epithelial detachment due to relatively clear fluid.
인도시아닌그린 혈관조영술(indocyanine green angiography, ICGA)에서 경계가 분명한 비교적 투명한 과형광이 초기부
터 관찰되어 후기까지 지속되어 망막색소상피박리 소견이 관찰되었다(Fig. 4). 이상과 같이 FAG 및 ICGA에서는 망
Left
Figure 5. Optical coherence tomography findings of the left eye at 1 month after photodynamic therapy plus intravitreal bevacizumab shows the same features as in the previous one.
Left
Figure 6.Optical coherence tomography findings of the left eye at the last visit show the same features as in the previous ones.
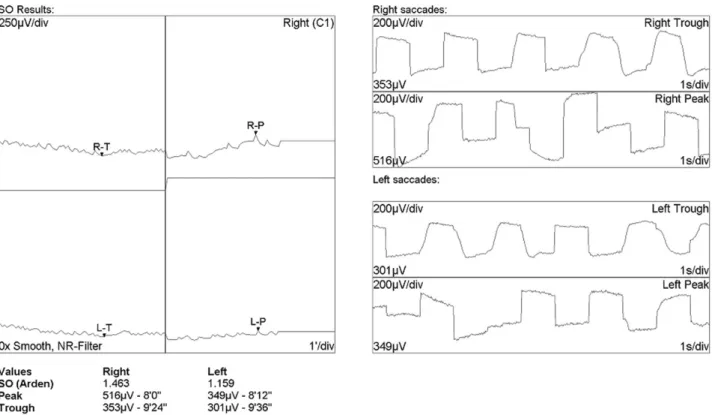
Figure 7. An electro-oculogram is abnormal with an Arden ratio of 1.463, 1.159 in both eyes, respectively. A diagnosis of Best’s disease is established.
막색소상피박리 소견을 보이나, 안저검사 및 OCT에서 양 안 장액망막박리 소견을 보이고 망막하 침착물에 의한 수 면이 관찰되며, 고령의 노인에서 오랫동안 스테로이드를 복 용한 병력으로 보아 저자들은 만성 중심성장액맥락망막병증 으로 진단하였고, 형광안저혈관조영에서 나타나지는 않았 지만 맥락막 신생혈관이 합병된 것으로 진단하였다. 좌안에 PDT 및 IVB를 병합치료 하였고, 그 후 1달 간격으로 2번 더 모두 3회 IVB를 시행하였다. PDT 및 IVB 병합치료 후
1개월, 3개월째 시행한 시력, 안저검사 및 OCT에서는 초진 시와 비교해서 변화가 없었다(Fig. 5, 6). 일반적으로 만성 중심성장액맥락망막병증에서 생긴 맥락막신생혈관의 경우 위와 같은 치료에 의해 맥락막신생혈관이 완전 퇴행되지는 않아도 망막하액의 감소가 있는 것이 보통이나 본 증례에 서는 전혀 치료에 반응을 하지 않았다. 따라서 확진을 위해 전기생리학적 검사를 시행하였고 망막전위도는 양안 정상 이었으나 안전위도 검사에서는 아덴비(Arden ratio)가 우안 1.463, 좌안 1.159로 나타나 양안 모두 1.5 이하로 심하게
Figure 8. Spectral domain optical coherence tomo- graphy findings of the left eye at the last visit show a clearly visible retinal pigment epithelium split and a low reflective space between split retinal pigment epithelium layers. High reflectivity can be seen between split retinal pigment epithelium layers, corresponding to subretinal exudates (arrows).
감소되어 베스트병으로 진단할 수 있었다(Fig. 7). 마지막 외래방문 시 시행한 시력, 안저검사, OCT에서 초진 시와 같은 소견을 보였다. 그러나 이때 처음으로 시행한 spectral domain (SD) OCT 검사에서 이전의 time domain (TD) OCT와 달리 망막색소상피층의 갈라짐 및 저반사 공간을 보였고 망막하 침착물은 망막색소상피층 갈라짐 사이의 고 반사를 보였다(Fig. 8).
고 찰
베스트병의 진단은 전형적인 안저소견, 상염색체우성으로 유전되는 가족력, 전형적인 발병시기 및 진행양상, 감소된 안전위도 등으로 내릴 수 있다. 그 중에서도 감소된 안전위 도 소견이 결정적인 진단 기준이다.3발병시기는 보통 3세 에서 15세 사이이며, 안저소견이 비슷하지만 나이 들어서 생기는 노른자모양 황반이영양증(adult-onset vitelliform macular dystrophy, AVMD)과 감별진단을 해야 한다.
AVMD는 베스트병과 달리 30세에서 50세 사이에 발병하 는데 병변의 크기가 보통 1 유두직경보다 작고 전형적인 진 행양상을 보이지 않으며, 진행 후기에 반흔 대신 망막색소 상피위축을 보이는 것이 보통이다. 특히 안전위도에서 베스 트병에서와 달리 정상 소견을 보인다.7 본 환자의 경우 초 진 시 베스트병을 의심할 수도 있었으나 우선 환자 나이가 고령이고 최근의 시력저하를 주소로 내원하였기 때문에 배 제하였다. 비슷한 안저소견을 보일 수 있는 AVMD는 병변 크기가 더 작고 FAG 에서 특징적으로 나타나는 가운데 저 형광을 둘러싸고 있는 주위의 과형광 소견이 없으므로 배 제하였다. 안전위도 검사도 초진 시에는 베스트병을 진단에 서 배제하였고, AVMD에서는 정상 안전위도 소견을 보이 므로 시행하지 않았다. 그 대신 오랫동안 스테로이드를 복 용한 병력이 있으며, OCT에서 장액망막박리가 관찰되었고, FAG 및 ICGA에서 망막색소상피박리 소견을 보여 만성 중 심성장액맥락망막병증에 합병된 맥락막신생혈관으로 진단 하였다. 나이관련황반변성에 합병된 맥락막신생혈관에 의 해 생길 수 있는 망막색소상피박리는 ICGA에서 혼탁한 삼 출에 의해 저형광 소견을 보이므로 진단에서 배제하였다.
본 증례에서 보듯이 ICGA에서 하부의 맥락막 구조물들이 보일 수 있는 비교적 투명한 망막색소상피박리는 혼탁하지 않은 망막하액이 생기는 중심성장액맥락망막병증에서 볼 수 있는 소견이다.8그러나 ICGA에서도 명확한 맥락막신생 혈관은 관찰되지 않아 과형광부위를 보이는 병변 전체에 PDT를 시행하였고, 병합요법으로 IVB를 하였다. 맥락막신 생혈관이 합병된 만성 중심성장액맥락망막병증의 치료로서 PDT 혹은 IVB의 효과가 최근에 많이 보고되었으나9,10 본 증례에서는 치료 후에도 전혀 호전이 없었고 확진을 위해 시행한 안전위도에서 심하게 저하된 소견을 보여 베스트병 진단을 내리게 되었다.
베스트병에서 생기는 침착물의 성분 및 위치에 대해서는 아직 명확히 밝혀진 바가 없다. Spaide et al11은 OCT를 통 해 망막하 공간과외망막층 표면에 위치한다고 하였고, 조직 학적 검사에 따르면 광범위한 lipofuscin이 망막색소상피 내에 위치하며 섬유성 물질이 망막색소상피 아래와 맥락막 층에 위치한다고 하였다.12최근에는 기존의 OCT보다 속도 가 50배 이상 빨라지고 해상력을 5 m까지 높인 SD OCT가 개발되어 시세포 및 망막색소상피층의 구조물들을 자세히 관찰할 수 있게 되었다. 초진 시 시행한 TD OCT에서 장액 망막박리 소견으로 생각한 것은 비교적 뚜렷한 RPE에 해당 하는 고반사가 관찰되었기 때문이었다. 그러나 마지막 방문 시 처음 시행한 SD OCT 검사에서 명확한 망막색소상피의 갈라짐(split) 및 그 사이의 저반사 공간이 관찰되었고, 망 막하 침착물이 있는 부위는 망막색소상피 갈라짐 사이의 고
반사 소견을 보여 이전의 TD OCT와는 다른 양상을 보였다.
본 증례에서 보듯이 베스트병에서 침착물의 정확한 위치를 알고자 할 때 SD OCT가 큰 도움이 될 수 있다. 그리고 초 진 시 SD OCT를 시행해서 망막색소상피층의 갈라짐과 침 전물을 확인할 수 있었다면 장액망막박리가 생기는 만성 중심성장액맥락망막병증은 배제할 수 있고 베스트병 진단 에 도움이 될 수 있지 않았을까 생각한다. 베스트병에서 맥 락막신생혈관이 합병되었을 때에는 PDT 혹은 IVB로 해부 학적, 기능적 호전을 보일 수 있으나5,6본 환자에서는 맥락 막신생혈관은 없었으며, 베스트병에서 생긴 망막색소상피 의 갈라짐 혹은 박리는 PDT 및 IVB 모두 효과가 없는 것을 알 수 있었다.
결론적으로 고령에서 생긴 베스트병 환자에서 만성 중심 성장액맥락망막병증에 합병된 맥락막신생혈관으로 오진하 여 PDT 및 IVB를 시행했으나 효과가 없었던 특이한 증상 및 경과를 보인 환자를 경험하였기에 보고하는 바이다.
참고문헌
1) Best F. Uber eine hereditaere makulaaffection; Beitraege zurverer- bungslehre. Zschr Augenheilk 1905;13:199-212.
2) Marmorstein AD, Marmorstein LY, Rayborn M, et al. Bestrophin, the product of the Best vitelliform macular dystrophy gene (VMD2), localizes to the basolateral plasma membrane of the retinal pigment epithelium. Proc Natl Acad Sci U S A 2000;97:
12758-63.
3) Deutman AF. Electro-oculography in families with vitelliform dystrophy of the fovea. Detection of the carrier state. Arch Ophthalmol 1969;81:305-16.
4) Deutman AF, Hoyng CB, van Lith-Verhoeven. Macular dys- trophies / vitelliform dystrophy. In: Ryan SJ, Schachat AP, eds.
Retina, 4th ed. Baltimore: Elsevier Mosby, 2006; v. 2. chap. 64.
5) Andrade RE, Farah ME, Costa RA. Photodynamic therapy with verteporfin for subfoveal choroidal neovascularization in best disease. Am J Ophthalmol 2003;136:1179-81.
6) Leu J, Schrage NF, Degenring RF. Choroidal neovascularisation secondary to Best’s disease in a 13-year-old boy treated by intra- vitreal bevacizumab. Graefes Arch Clin Exp Ophthalmol 2007;
245:1723-5.
7) Miyake Y, Shiroyama N, Horiguchi M, et al. Bull’s-eye maculo- pathy and negative electroretinogram. Retina 1989;9:210-5.
8) Yannuzzi LA, Flower RW, Slakter JS. Central serous Chorio- retinopathy. In: Craven L, eds. Indocyanine green angiography, 1st ed. St. Louise: Mosby Co, 1997; v. 1. chap. 22.
9) Chan WM, Lam DS, Lai TY, et al. Treatment of choroidal neovas- cularization in central serous chorioretinopathy by photodynamic therapy with verteporfin. Am J Ophthalmol 2003;136:836-45.
10) Chan WM, Lai TY, Liu DT, Lam DS. Intravitreal bevacizumab (avastin) for choroidal neovascularization secondary to central serous chorioretinopathy, secondary to punctate inner choroido- pathy, or of idiopathic origin. Am J Ophthalmol 2007;143:977-83.
11) Spaide RF, Noble K, Morgan A, Freund KB. Vitelliform macular dystrophy. Ophthalmology 2006;113:1392-1400.
12) O’Gorman S, Flaherty WA, Fishman GA, Berson EL. Histo- pathologic findings in Best’s vitelliform macular dystrophy. Arch Ophthalmol 1988;106:1261-8.
=ABSTRACT=
Best Disease With Old-age Onset Misdiagnosed as Chronic Central Serous Chorioretinopathy: A Case Report
Won Bin Cho, MD, Hyun Jin Shin, MD, Jun Woong Moon, MD, Hyung Chan Kim, MD, PhD
Department of Ophthalmology, Konkuk University Medical Center, Konkuk University School of Medicine, Seoul, Korea
Purpose: To report a case of Best’s disease with old-age-onset with unusual clinical features.
Case summary: A 68-year-old woman with a six-month history of using oral steroids complained of decreased vision in both eyes. Fundus examination revealed a circular area of macular elevation measuring approximately 1.5 disc diameter size in both eyes. Optical coherence tomography (OCT) showed serous retinal detachment, but pigment epithelial detachment was seen only on fluorescein angiography and indocyanine green angiography. The patient received a diagnosis of chronic central chorio- retinopathy with choroidal neovascularization. Photodynamic therapy (PDT) and intravitreal bevacizumab (IVB) injections were prescribed as treatment, but were ineffective. For a definitive diagnosis, we performed an electro-oculogram (EOG) and the result was abnormal with an Arden ratio below 1.5 in both eyes. A final diagnosis of Best’s disease was established. Spectral domain OCT findings at the last visit showed a clearly visible RPE split and a low reflective space between the split RPE layers, as well as a high reflectivity corresponding to the subretinal material.
Conclusions: We report a case of Best’s disease with old-age onset with unusual clinical features and abnormal EOG findings.
Spectral domain OCT was helpful in evaluating the disease. Treatment with PDT and IVB was not effective.
J Korean Ophthalmol Soc 2009;50(8):1275-1281
Key Words: Best disease, Bevacizumab, Photodynamic therapy
Address reprint requests to Hyung Chan Kim, MD, PhD
Department of Opthalmology, Konkuk University Medical Center, Konkuk University School of Medicine
#4-12 Hwayang-dong, Gwangjin-gu, Seoul 143-729, Korea
Tel: 82-2-2030-5270, Fax: 82-2-2030-5273, E-mail: [email protected]