https://doi.org/10.14734/PN.2020.31.1.55 pISSN 2508-4887•eISSN 2508-4895
Wook Jin, MD,
Dong Woo Son, MD, PhD, Hye Jung Cho, MD, Eun Jin Kim, MD
Department of Pediatrics, Gachon University Gil Medical Center, Incheon, Korea
Thyroid dysfunction is common in preterm infants. Breastmilk-fed (BMF) preterm infants in Korea often develop hypothyroidism because of excessive maternal iodine ingestion. Recently in our neonatal intensive care unit, we encountered three pairs of BMF preterm twins showing discrepancies in thyroid function at 1 month of age. Their mothers consumed seaweed soup daily during that time.
Within each BMF pair, the amount of breastmilk intake was almost similar. However, thyroid function differed within twins. Urinary iodine concentrations were different within twins and not correlated with thyroid dysfunction. The clinical characteristics within each pair were not significantly different.
In conclusion, thyroid function would be different even between BMF premature twin siblings despite the same amount of iodine intake and the similar conditions that are currently known to affect thyroid function. Therefore, serial evaluation of thyroid function in BMF preterm infants would be crucial.
Key Words: Infant, premature, Twins, Thyroid gland, Breast feeding, lodine
Introduction
It is now a well-known fact that preterm neonates are at higher risk of hypothyroidism than term neonates.1 A second neonatal screening for thyroid function is currently recommended in the preterm neonate because of the increased risk of developing delayed thyrotropin eleva- tion (dTSH), which is defined as transient TSH level elevation occurring at 2-6 weeks of age.2 Under the recommendation, initial thyroid function screening is performed at 1 week of age, and rescreening at 1 month of age for preterm neonates in our neonatal intensive care unit (NICU).
Iodine is a crucial component of thyroid hormone synthesis, and iodine deficiency can lead to neurodevelopmental impairment.3 Therefore, adequate iodine intake is needed for preterm neonates.4 In contrast, excessive iodine intake can also lead to thyroid dysfunction.5 Excessive iodine exposure inhibits thyroid hormone synthesis by an autoregulatory mechanism known as the acute Wolff-Chaikoff effect.6
Korean mothers commonly consume seaweed soup to promote lactation, and the iodine content of their breastmilk is found to be much higher than that of mothers in other countries.7 An infant was reported to have hypothyroidism due to maternal iodine intoxication as a result of seaweed soup consumption.8 Likewise, breastmilk-fed (BMF) preterm infants in Korea often develop subclinical hypothyroidism because of excessive maternal iodine ingestion.4
In our NICU, there were some twins with different thyroid hormone test results despite the same amount of consumed breastmilk from their own mother, indicating the same intake of Received: 18 September 2019
Revised: 2 November 2019 Accepted: 11 November 2019 Correspondence to
Dong Woo Son, MD, PhD Department of Pediatrics, Gachon University Gil Medical Center, 21 Namdong-daero 774beon-gil, Namdong-gu, Incheon 21565, Korea Tel: +82-32-460-3224
Fax: +82-32-460-8382 E-mail: [email protected] Copyright© 2020 by The Korean Society of Perinatology
This is an Open Access article distributed under the terms of the Creative Com- mons Attribution Non-Commercial License (http://creativecommons.org/
license/by-nc/4.0/), which permits unrestricted non-commercial use, distribution, and reproduction in any
Thyroid Function of Preterm Twins Having
Breastmilk from Their Mothers Consuming
Seaweed Soup Might Be Variable between
Siblings: A Case Series
pairs of twins under a similar intake of iodine and compared their thyroid function.
Case
1. Our routine thyroid function evaluations for premature infants in our NICU
In our NICU, a thyroid function test (TFT), including free thy- ro xine (fT4), triiodothyronine (T3), and thyrotropin (TSH), was performed routinely at 1 week and 1 month of age. When the re sults of TFT were abnormal, we gathered the clinical factors that can affect thyroid function, such as existence of patent ductus arteriosus (PDA), development of respiratory distress syndrome (RDS) requiring surfactant treatment, necrotizing en- terocolitis (NEC) (Bell stage ≥IIA), intraventricular hemorrhage (IVH) (grade ≥3). Also, the use of medications that can affect thyroid function (e.g., dopamine, glucocorticoid, furosemide, phenobarbital, insulin, and vancomycin) was collected. Urinary iodine concentration (UIC) was measured in a BMF infant when TFT results were abnormal. In case of BMF twin, UIC was also measured in another sibling if TFT results were found to be ab- normal in one of the siblings. A spot urine sample was collected via a urine bag and added into the collecting tube to obtain a sufficient volume for testing during night time. Then, the urine samples were sent to a certified laboratory. Thyroid ultrasono- graphy was performed when TFT results were found to be ab- normal. In case of twin, thyroid ultrasonography was performed in another sibling when TFT results were found to be abnormal in one of the siblings.
2. The cases
Among preterm infants born at ≤34-week gestation and admitted to the NICU of Gachon University Gil Hospital between January 2019 and July 2019, three twins showed different thyroid dysfunction between siblings while ingesting mainly breastmilk of their own mothers. The mothers had never been diagnosed with thyroid disease. All mothers of the three twins were reported to have been consuming seaweed soup daily. We considered that the amount of iodine intake correlates with the amount of breastmilk intake. All twins were mostly BMF, and premature formula milk was provided when there was a brief shortage of
breastmilk supply because of delayed delivery. Each twin was named twin A, twin B, and twin C. Numbers 1 and 2 were assigned to distinguish the first child and the second child.
1) Twin A
Twin A was a monozygotic diamniotic twin. Gestational age (GA) of twin A was 30 1/7 weeks. Twin A was appropriate for GA (AGA), even though they had 28.9% weight discrepancy.
Apgar scores at 5 minutes were 9 in both infants. They did not have any history of PDA, RDS, NEC, or IVH (Table 1). There was no history of dopamine, glucocorticoid, furosemide, phenobar- bital, insulin, and vancomycin administration.
Infant A-1 was not able to start breastfeeding before the initial screening, unlike infant A-2. In cumulative breastmilk ingestion until the second TFT, there was not much difference between siblings (infants A-1 and A-2, 2,546.6 vs. 2,449.1 mL/kg; 3.8%
discrepancy) (Table 1).
The initial TFT results of both infants at 6 days of life (DOL) were normal. The second TFT was performed at 1 month of age.
In infant A-1, fT4 level was decreased to 0.53 ng/dL (normal, 0.9-1.78 ng/dL), and TSH level increased to 56.781 μIU/mL. In infant A-2, fT4 level was 1.12 ng/dL, and TSH level was 13.047 μIU/mL (Table 1, Fig. 1). Thyroid ultrasonography performed after the second TFT showed normal size and location of thyroid glands in both infants. UIC increased in both infants (infants A-1 and A-2, 1,747 vs. 2,388 μg/L [normal, 42-350 μg/L], 26.8%
discrepancy) (Table 1).
2) Twin B
Twin B was a dizygotic diamniotic twin. They were born through an in-vitro-fertilization. GA of twin B was 32 0/7 weeks. They were AGA. Apgar scores at 5 minutes were 9 in both infants.
They did not have any history of PDA, RDS, NEC, or IVH. There was no history of dopamine, glucocorticoid, furosemide, pheno- barbital, insulin, and vancomycin administration.
Both infants started breastfeeding before the initial screening.
There was not much difference in breastmilk ingestion until the initial TFT between siblings (infants B-1 and B-2, 32.5 vs. 34.9 mL/kg). In cumulative breastmilk ingestion by the second TFT, there was not much difference between siblings (infants B-1 and B-2, 2,477.6 vs. 2,164.6 mL/kg, 12.6% discrepancy).
The initial TFT results of both infants at 6 DOL were normal.
3) Twin C
Twin C was a dizygotic diamniotic twin. GA of twin C was 30 1/7 weeks. They were AGA. Apgar scores at 5 minutes were 9 in infant C-1 and 10 in infant C-2. Twin C underwent ibuprofen enema at 3 DOL for PDA, and the PDAs were found closed for both patients at 6 DOL. They did not have any history of RDS, NEC, or IVH. There was no history of dopamine, glucocorticoid, furosemide, phenobarbital, insulin, and vancomycin administration.
Both infants started breastfeeding before the initial screening.
There was not much difference in breastmilk ingestion until the initial TFT between siblings (infants C-1 and C-2, 15.4 vs. 16.8 mL/kg). Infant C-1 had greater total amount of breastmilk fee- ding than infant C-2 (2,275.6 vs. 1,873.2 mL/kg, 17.7% discre- pancy).
The initial TFT results of both infants at 6 DOL were normal.
At the second TFT performed 1 month of age, fT4 level was 1.2 ng/dL and TSH level was 9.576 μIU/mL in infant C-1. In infant C-2, fT4 level decreased to 0.88 ng/dL, and TSH increased to 67.615 μIU/mL (Table 1, Fig. 1). Thyroid ultrasonography per- formed after the second TFT showed normal size and location of thyroid glands in both infants. UIC increased in all patients (infants C-1 and C-2, 1,586 vs. 1,337 μg/L) (Table 1).
The second TFT, which was performed at 1 month of age, showed fT4 level of 0.89 ng/dL and TSH level of 73.893 μIU/mL in infant B-1. In infant B-2, fT4 level was 1.25 ng/dL, and TSH level was 20.623 μIU/mL (Table 1, Fig. 1). Thyroid ultrasono- graphy performed after the second TFT showed normal size and location of thyroid glands in both infants. UIC increased in all patients (infants B-1 and B-2, 928 vs. 658 μg/L) (Table 1).
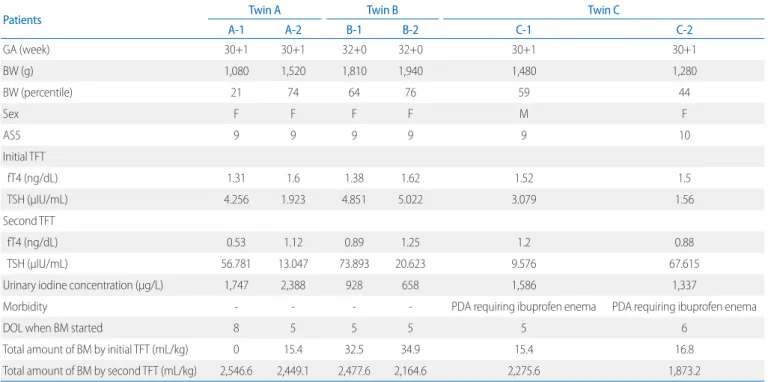
Table 1. Clinical Characteristics of Twins
Patients Twin A Twin B Twin C
A-1 A-2 B-1 B-2 C-1 C-2
GA (week) 30+1 30+1 32+0 32+0 30+1 30+1
BW (g) 1,080 1,520 1,810 1,940 1,480 1,280
BW (percentile) 21 74 64 76 59 44
Sex F F F F M F
AS5 9 9 9 9 9 10
Initial TFT
fT4 (ng/dL) 1.31 1.6 1.38 1.62 1.52 1.5
TSH (μIU/mL) 4.256 1.923 4.851 5.022 3.079 1.56
Second TFT
fT4 (ng/dL) 0.53 1.12 0.89 1.25 1.2 0.88
TSH (μIU/mL) 56.781 13.047 73.893 20.623 9.576 67.615
Urinary iodine concentration (μg/L) 1,747 2,388 928 658 1,586 1,337
Morbidity - - - - PDA requiring ibuprofen enema PDA requiring ibuprofen enema
DOL when BM started 8 5 5 5 5 6
Total amount of BM by initial TFT (mL/kg) 0 15.4 32.5 34.9 15.4 16.8
Total amount of BM by second TFT (mL/kg) 2,546.6 2,449.1 2,477.6 2,164.6 2,275.6 1,873.2
Abbreviations: GA, gestational age; BW, birth weight; AS5, APGAR score at 5 minutes; TFT, thyroid function test; fT4, free thyroxine; TSH, thyrotropin; PDA, patent ductus arteriosus; DOL, days of life; BM, breastmilk.
Fig. 1. The figure showed the changes in thyroid function test results from the initial tests checked at 1 week of age to the second test checked at 1 month of age. Each segment represented the changes (right to the left) of the results of each infant. All infants had a decrease in fT4 level and increase in TSH level at the second thyroid function test. TSH, thyrotropin; fT4, free thyroxine.
cations such as dopamine, glucocorticoid, furosemide, and phe- nobarbital are known to affect thyroid function.15 Furthermore, iodine in topical antiseptic agents and contrast media can affect thyroid function of preterm neonates.16 In our NICU, iodine anti- septic agent has not been used for many years, so any effect of topical iodine antiseptic agents could be ruled out. Additionally, those medications that might affect thyroid function were not administered to the three twins.
It is known that the size of the thyroid gland affects thyroid hormone synthesis and storage capacity.15 We performed thy- roid ultrasonography, and all patients’ thyroid glands were nor- mal in size and location.
Each sibling of twin A and B had similar iodine intake according to the total amount of breastmilk intake. As mentioned above, iodine antiseptic agent is not used in our NICU, so any other source of iodine could not be expected. Infant C-1’s iodine in- take was higher than that of infant C-2 according to the total amount of breastmilk intake. UIC of infant C-1 was higher than that of infant C-2. However, the second TFT results of infant C-2 showed hypothyroidism, while infant C-1 was euthyroid.
Generally, median UIC is considered a good indicator and recom- mended barometer of iodine intake in the population other than infants.17 We found that the relationship between UIC and the total amount of breastmilk intake might be variable in infants.
The UIC results of each twin showed no possible correlation to the total amount of breastmilk intake. Furthermore, the number of laboratory results was too small to perform any analysis.
Further studies would be required to determine the association between UIC and the amount of breastmilk intake in twin studies.
One Korean study on preterm infants reported that excessive iodine intake induced subclinical hypothyroidism, which showed a good positive correlation between UIC and TSH levels.4 They used UIC instead of creatinine-corrected-UIC because UIC/
creatinine ratio was known to be unreliable.4 Thus, we use UIC in clinical situations in our NICU. In our case-series, only twin B showed higher TSH level in an infant with higher UIC, while the other two twins did not. We could not show any correlation bet- ween thyroid function and UIC (Fig. 2). Likewise, one study with term newborns in 2010 failed to show any correlation between neonatal TSH and neonatal UIC.18 Further studies, especially with preterm twins, are required to determine the association between UIC and thyroid function.
Discussion
Our NICU is attempting to accomplish exclusive breastmilk feeding since 2019 under the recommendation of the American Academy of Pediatrics.9 Since the attempt, the number of preterm neonates with abnormal TFT results in our NICU increased. Ex- cessive iodine content in breastmilk in Korean mothers leading to higher levels of ingested iodine is considered the main reason for this outcome. Breastmilk iodine in Korean mothers was re- ported at the average level of 2,170 μg/L (reference range, 802- 8,671), which indicates that iodine excess is common in Korean mothers.7 Despite the equal amount of consumed breastmilk from their own mother, thyroid function of some twins in our NICU showed a significant difference. We report three twins with different thyroid functions between siblings with similar iodine intake. To our knowledge, this is the first study that com- pared thyroid function between twins with similar amounts of consumed breastmilk from their own mother.
There are several factors that affect thyroid function in pre- term infants. Adequacy of weight is considered a factor that influences TSH level. One study reported that TSH levels are higher in preterm small for gestational age (SGA) infants than in preterm AGA infants.10 Another Japanese study reported that SGA is a risk factor for the development of dTSH in infants with a birth weight (BW) ≤2,000 g.11 The three twins in this study were all preterm AGA infants. However, infants with lower BW showed a trend for higher TSH and lower fT4 levels than the other siblings in the second TFT. A Korean study reported that smaller BW is associated with treatment for hypothyroidism in very low birth weight infants.12 In our twins, the weight discre- pancy was as follows: 28.9% for twin A, 6.7% for twin B, and 13.5% for twin C. As the discrepancy rates for two twins were not that high, it is uncertain whether the weight difference would result in difference in thyroid function.
It has been reported that the development of RDS is associated with low thyroid hormone level of cord sera.13 Moreover, PDA was reported as a risk factor for the development of dTSH in newborns in the NICU.14 The three twins had no RDS. In twin C, both siblings at the same DOL had PDA that required medication.
Thus, PDA and medication would not lead to a difference in thyroid function in twin C. Vancomycin and insulin administration is considered a risk factor for the development of dTSH.14 Medi-
To prevent the development of hypothyroidism after exposure to excessive iodine, an escape from the acute Wolff-Chaikoff effect should occur.6 However, in preterm infants, the immature thyroid gland is unable to escape from the acute Wolff-Chaikoff effect, making them more susceptible to hypothyroidism due to excessive iodine intake.19 It is known that escape from the Wolff- Chaikoff effect seems to appear at a GA of ≥35 weeks among preterm infants.20 Only twin B was ≥35 weeks adjusted GA at the second TFT. The other two twins were 34 weeks adjusted GA. We are uncertain whether the variance in thyroid function in our three twins might be a result of the variable timing of the es- cape phenomenon development in individual premature infants.
The limitation of our study is that we were unable to obtain the iodine concentration of each mother’s breastmilk because there is no accessible laboratory for breastmilk iodine concentration (BIC) measurement. Routine measurement of BIC in every BMF preterm may not be practical. Under the circumstances that ex- clusive breastmilk feeding is widely recommended, more and more preterm infants would be affected by high iodine ingestion in Korea. It will be important to raise awareness that excessive iodine intake can cause hypothyroidism in preterm infants and recommendation guidelines of iodine ingestion, especially for Korean mothers nursing preterm infants should be considered.
We showed that thyroid function could be different even in preterm twins despite the same amount of iodine intake and under the same circumstances that are currently known to affect thyroid function. Therefore, serial evaluation of thyroid function in BMF preterm infants would be crucial.
Conflict of interest
No potential conflict of interest relevant to this article was reported.
References
1) Carrascosa A, Ruiz-Cuevas P, Clemente M, Salcedo S, Almar J. Thyroid function in 76 sick preterm infants 30-36 weeks: results from a longitu- dinal study. J Pediatr Endocrinol Metab 2008;21:237-43.
2) Kaluarachchi DC, Colaizy TT, Pesce LM, Tansey M, Klein JM. Congenital hypothyroidism with delayed thyroid-stimulating hormone elevation in premature infants born at less than 30 weeks gestation. J Perinatol 2017;37:277-82.
3) Li H, Richard K, McKinnon B, Mortimer RH. Effect of iodide on human choriogonadotropin, sodium-iodide symporter expression, and iodide uptake in BeWo choriocarcinoma cells. J Clin Endocrinol Metab 2007;92:
4046-51.
4) Chung HR, Shin CH, Yang SW, Choi CW, Kim BI. Subclinical hypothyroidism in Korean preterm infants associated with high levels of iodine in breast milk. J Clin Endocrinol Metab 2009;94:4444-7.
5) Leung AM, Braverman LE. Consequences of excess iodine. Nat Rev Endocrinol 2014;10:136-42.
6) Wolff J, Chaikoff IL, Goldberg RC, Meier JR. The temporary nature of the inhibitory action of excess iodine on organic iodine synthesis in the normal thyroid. Endocrinology 1949;45:504-13.
7) Moon S, Kim J. Iodine content of human milk and dietary iodine intake of Korean lactating mothers. Int J Food Sci Nutr 1999;50:165-71.
8) Shumer DE, Mehringer JE, Braverman LE, Dauber A. Acquired hypothy- roidism in an infant related to excessive maternal iodine intake: food for thought. Endocr Pract 2013;19:729-31.
9) Eidelman AI. Breastfeeding and the use of human milk: an analysis of the American Academy of Pediatrics 2012 Breastfeeding Policy State- ment. Breastfeed Med 2012;7:323-4.
10) Bosch-Giménez VM, Palazón-Bru A, Blasco-Barbero Á, Juste-Ruiz M, Rizo-Baeza MM, Cortés-Castell E. Multivariate analysis of thyrotropin in preterm newborns based on adequacy of weight for gestational age.
Thyroid 2017;27:120-4.
11) Uchiyama A, Watanabe H, Nakanishi H, Totsu S. Small for gestational age is a risk factor for the development of delayed thyrotropin elevation in infants weighing less than 2000 g. Clin Endocrinol (Oxf) 2018;89:431-6.
12) Lee JH, Kim SW, Jeon GW, Sin JB. Thyroid dysfunction in very low birth weight preterm infants. Korean J Pediatr 2015;58:224-9.
13) Abbassi V, Adams J, Duvall D, Phillips E. Prenatal thyroid function abnor- malities in infants with idiopathic respiratory distress syndrome. Pediatr Res 1984;18:926-8.
14) Zung A, Bier Palmon R, Golan A, Troitzky M, Eventov-Friedman S, Marom R, et al. Risk factors for the development of delayed TSH elevation in Fig. 2. The figure showed the distribution of the thyrotropin levels ac-
cording to the UIC of each infant. The thyrotropin levels failed to show any relationship with the UICs. However, the numbers of the dataset were too small for any analysis. TSH, thyrotropin; UIC, urinary iodine concentration.
neonatal intensive care unit newborns. J Clin Endocrinol Metab 2017;
102:3050-5.
15) Chung HR. Screening and management of thyroid dysfunction in pre- term infants. Ann Pediatr Endocrinol Metab 2019;24:15-21.
16) Thaker VV, Leung AM, Braverman LE, Brown RS, Levine B. Iodine-induced hypothyroidism in full-term infants with congenital heart disease: more common than currently appreciated? J Clin Endocrinol Metab 2014;99:
3521-6.
17) Andersson M, Karumbunathan V, Zimmermann MB. Global iodine status in 2011 and trends over the past decade. J Nutr 2012;142:744-50.
18) Hashemipour M, Nasri P, Hovsepian S, Hadian R, Heidari K, Attar HM, et
al. Urine and milk iodine concentrations in healthy and congenitally hypothyroid neonates and their mothers. Endokrynol Pol 2010;61:371- 6.
19) Theodoropoulos T, Braverman LE, Vagenakis AG. Iodide-induced hypo- thyroidism: a potential hazard during perinatal life. Science 1979;205:
502-3.
20) Salvatore D, Davies TF, Schlumberger MJ, Hay ID, Larsen PR. Thyroid physiology and diagnostic evaluation of patients with thyroid disorders.
In: Melmed S, Polonsky KS, Larsen PR, Kronenberg HM, editors.Williams textbook of endocrinology. 13th ed. Philadelphia: Elsevier Co; 2017. p.
333-68.