1)
서 론
, ,
, ,
.
: 2009 5 27 , : 2009 10 26
: ,
Tel : 054)770-8254, Fax : 054)770-8500 E-mail : [email protected]
1)
.
.
, .
대상 및 방법
신생아 경련과 예후에 관한 고찰
송 화 조은영 김애숙 이선주 이동석 최성민 김두권․ ․ ․ ․ ․ ․
= Abstract =
A Study of Clinical Features and Prognosis of Neonatal Seizures
Hwa Song, M.D., Eun Young Cho, M.D., Ae Suk Kim, M.D., Sun Ju Lee, M.D.
Dong Seok Lee, M.D., Sung Min Choi, M.D. and Doo Kwun Kim, M.D.
Department of Pediatrics, College of Medicine, Dongguk University, Gyeong-ju, Korea Purpose : Neonatal seizures are relatively common and the symptoms are clinically dif- ferent from those in older children and adults. The goal of this study is to help understand neonatal seizures by analyzing the etiology, clinical features, method of diagnosis and pro- gnosis of the affected patients in our hospital.
Methods : Twenty six cases with neonatal seizures who were admitted to the neonatal intensive care unit, Dongguk University Hospital from January 1999 to October 2008 were retrospectively reviewed. They were evaluated with risk factors, neurologic examinations, laboratory data, neuroimaging studies, EEG findings, seizure types, response to treatment, and outcomes.
Results : Subtle seizure came out to be the most common seizure type(9 patients: 34.6
%). The cause of neonatal seizures were hypoxic-ischemic encephalopathy(9 patients: 34.6
%), intracranial hemorrhage(8 patients: 30.8%), electrolyte imbalance(8 patients: 30.8%), meningitis(7 patients: 26.9%). Nineteen out of 25 patients showed abnormal lesion on neu- roimaging studies such as intracranial hemorrhage, periventricular leukomalacia, brain in- farction, etc. Abnormal EEG findings were noted in 19 patient(73.1%). Phenobarbital was tried as a first line antiepileptic drug and phenytoin was added if it failed to control seizures.
The overall outcome was relatively good except for those with abnormal EEG findings.
Conclusion : Neonatal seizures signify underlying diseases. Recognition of etiology is often helpful in prognosis and treatment. Neuroradiological and EEG findings are important in predicting neurologic outcomes in newborns with seizures.
Key Words : Neonatal seizures, EEG, Neurologic examinations, Prognosis
1999 1 2008 10
26
, ,
, , ,
, .
Rose
2)24 , 2-3 , 4-7 , 8
. Lombroso
3), ,
Volpe
4).
결 과
성비 및 출생 기록 1.
26 15 ,
11 . 31 6 41
38.3±2.9 37
3 . 2,500 g
20 (76.9%) 2,500 g 6 (23.1
%) . 26 6 (23.1%)
Moro 4 (15.4%), 2 (7.7%) (Table 1, 2).
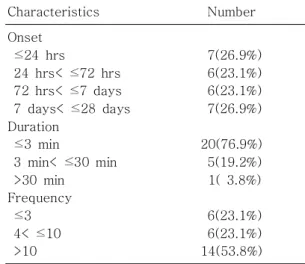
경련의 발생 시기 2.
26 24
7 (26.9%), 2-3 6 (23.1%),
4-7 6 (23.1%), 7 (26.9
%) . 3
20 (76.9%) , 3 30
5 (19.2%), 30 1 (3.8%)
. 3 6 (23.1%), 4
10 6 (23.1%), 11
14 (Table 3).
26 6 (23.1%) 3
3 (11.5%) 4 .
6 (23.1%) 3 2
(7.7%) 3 . 7
(19.2%) 3 (11.5%) 3 , 4 (15.4%)
3 . 4 (15.4%)
3 2 (7.7%)
1 3
Table 1. Baseline Characterstics of Patients
Characteristics Number
Number of patients Male:Female Gestational age
<37weeks 37weeks
≥
Birth weight
<2,500 g 2,500 g
≥
26 15:11
3(11.5%) 23(88.5%)
6(23.1%) 20(76.9%)
Table 2. Physical Finding at Time of Seizures Abnormal physical findings
Decreased Moro reflex Cephalohematoma Normal
6(23.1%) 4 2 20(76.9%)
Table 3. Characteristics of Seizures
Characteristics Number
Onset 24 hrs
≤
24 hrs< ≤ 72 hrs 72 hrs< ≤ 7 days 7 days< ≤ 28 days Duration
3 min
≤
3 min< ≤ 30 min
>30 min Frequency
3
≤ 4< ≤ 10
>10
7(26.9%) 6(23.1%) 6(23.1%) 7(26.9%)
20(76.9%) 5(19.2%) 1( 3.8%)
6(23.1%)
6(23.1%)
14(53.8%)
. 2 (7.7%) 3
, 1 (3.8%) 3
(Table 4).
발작 형태 3.
9 (34.6%) ,
7 (26.9%),
5 (19.2%), 3 (11.5%),
2 (7.7%) , -
(Table 5).
뇌파 소견 4.
26 24 (92.3%) 19 (73.1%)
abundance of sharp transients 1 (3.8%), se- verely depressed electrical activity 3 (11.5%), (focal spike with normal background) 6 (23.1%),
(focal spike with abnormal background) 3 (11.5%), - (burst-suppression) 4
(15.4%), focal monorhythmic periodic pattern 1 (3.8%), (multifocal icteric pat-
terns) 1 (3.8%), (diffuse
continuous slow background activities) 1 (3.8
%) , 4 (15.4%) .
20 (76.9%) 17 (65.4%)
5 (19.2%),
5 (19.2%), - 1
(3.8%), 1 (3.8%) , 5 (19.2
%) (Table 6).
뇌영상 소견 5.
26 25 (96.2%) , 19 (73.1%)
. 8 (30.8%), 4 (15.4
%), 3 (12%) ,
(mild ventriculomegaly) 1 (3.8
%), (cyst on germinal matrix) 1 (3.8%), (cyst at caudothala-
mic groove) 1 (3.8%), (cyst
on pituitary gland) 1 (3.8%) (Table 7).
치료 및 반응 6.
, , ,
1 (3.8%) pheno-
barbital . 9 (34.6%) phenobarbi-
Table 4. Etiolgy of Neonatal Seizures
Onset age of seizure ≤ 3 days >3 days Total
Hypoxic-ischemic encephalopathy Intracranial hemorrhage
Meningitis
Electrolyte imbalance hypocalcemia hypoglycemia
hyponatremia and hypocalcemia hypernatremia
Unknown
6(23.1%) 6(23.1%) 3(11.5%)
2( 7.7%) 2( 7.7%) 2( 7.7%) 0( 0%) 1( 3.8%)
3(11.5%) 2(7.7%) 4(15.4%)
1( 3.8%) 0( 0%) 0( 0%) 1( 3.8%) 1( 3.8%)
9(34.6%) 8(30.8%) 7(26.9%)
3(11.5%) 2( 7.7%) 2( 7.7%) 1( 3.8%) 2( 7.7%) Table 5. Seizure Types
Subtle
Multifocal clonic Generalized clonic Focal clonic Generalized tonic
9(34.6%)
7(26.9%)
5(19.2%)
3(11.5%)
2( 7.7%)
tal , 4 (15.4%) phenobarbi-
tal phenytoin , 1 (3.8%)
phenobarbital, phenytoin, lorazepam
, 1
(3.8%) midazolam .
8.2±2.7 ,
16 2 (7.7%)
1 8 10 (38.4%), 8
4 (15.4%) (Table 8).
예 후 7.
26 16 (61.5%)
, 3 (11.5%) ,
(Table 9). 16 (61.5%)
2 (7.7%) 8 (30.8%)
, 3
(11.5%) .
10 (38.5%)
3 6 (23.1%) 3
. 3 (11.5%)
4 (15.4%)
5 (19.2%) 4 (15.4%) .
26 7 (26.9
%) 4 (15.4%), 3 (11.5%),
Table 8. Treatment and Duration of Therapy Treatment
Phenobarbital
Phenobarbital, phenytoin
Phenobarbital, phenytoin, lorazepam Calcium gluconate, phenobarbital Calcium gluconate
Glucose, sodium Midazolam drip Treatment duration
During admission 1 ≤ <8 weeks
8 weeks
≥
9(34.6%) 4(15.4%) 1( 3.8%) 1( 3.8%) 4(15.4%) 4(15.4%) 1( 3.8%)
2( 7.7%) 10(38.4%)
4(15.4%)
Table 9. Overall Prognosis Normal
Epilepsy
Developmental delay Cerebral palsy
Epilepsy, cerebral palsy developmental delay Unknown
16(61.5%) 3(11.5%) 2( 7.7%) 1( 3.8%) 1( 3.8%)
3(11.5%) Table 6. Electroencephalographic Finding
Initial F/U Abnormal
Abundance of sharp transients
Severely depressed electrical activity Focal spike with normal
background Focal spike with
abnormal background Burst-suppression pattern Focal monorhythmic
periodic pattern
Multifocal icteric patterns Diffuse continuous slow
background activity Normal
Not done
1( 3.8%)
3(11.5%)
6(23.1%)
3(11.5%)
4(15.4%) 1( 3.8%)
1( 3.8%) 1( 3.8%)
4(15.4%) 2( 7.7%)
5(19.2%)
5(19.2%)
1( 3.8%)
1( 3.8%)
5(19.2%) 9(34.6%)
Table 7. Neuroimaging Findings of Patients Abnormal
Intracranial hemorrhage Infarction
PVL
Mild ventriculomegaly Cyst on germinal matrix Cyst at caudothalamic groove Cyst on pituitary gland Normal
Not done
19(73.1%)
8
4
3
1
1
1
1
6(26.9%)
1( 3.8%)
Abbreviations : PVL, periventricular leukomalacia
2 (7.7%) 1 (3.8%)
, .
3 (11.5%)
, 2 (7.7%) . 2 (7.7
%) , 1 (3.8%)
.
3 (11.5%), 2 (7.7%),
2 (7.7%)
. 1 4 (15.4
%), 1 -3 3 (11.5%) , 2
(7.7%) 10 , 5 (19.2
%) 10 3 10
. 7 (26.9%)
6 (23.1%) , 4
(15.4%) . 7
(26.9%) 6 (23.1%) 6 (23.1
%) ,
1
(Table 10, 11).
고 찰
,
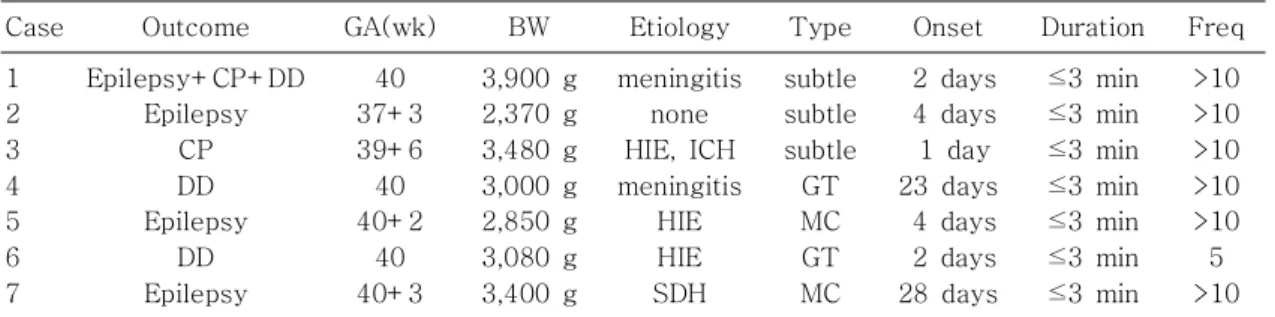
. Table 10. Clinical Features of Patients with Poor Prognosis(N=7)
Case Outcome GA(wk) BW Etiology Type Onset Duration Freq
1 2 3 4 5 6 7
Epilepsy+CP+DD Epilepsy
CP DD Epilepsy
DD Epilepsy
40 37+3 39+6 40 40+2
40 40+3
3,900 g 2,370 g 3,480 g 3,000 g 2,850 g 3,080 g 3,400 g
meningitis none HIE, ICH meningitis
HIE HIE SDH
subtle subtle subtle GT MC GT MC
2 days 4 days 1 day 23 days
4 days 2 days 28 days
3 min
≤ 3 min
≤ 3 min
≤ 3 min
≤ 3 min
≤ 3 min
≤ 3 min
≤
>10
>10
>10
>10
>10 5
>10 Abbreviations : GA(wk), gestational age(weeks); BW, body weight; Freq, frequency; CP, cerebral palsy;
DD, developmental delay; HIE, hypoxic-ischemic encephalopathy; ICH, intracranial hemorrhage; SDH, subdural hemorrhage; GT, generalized tonic; MC, multifocal clonic
Table 11. EEG & Neurologic Image of Patients with Poor Prognosis(N=7)
Case Outcome EEG(initial) EEG(F/U) Neuroimage
1
2
3
4 5 6
7
Epilepsy+CP+DD
Epilepsy
CP
DD Epilepsy
DD
Epilepsy
Focal monorhythmic periodic pattern
Focal spike with normal background
Burst-suppression
Not done
Burst-suppression Focal spike with normal
background
Focal spike with normal background
Focal spikes with normal backbround
Focal spike with abnormal background
Focal spike with normal background
Not done
Multifocal icteric patterns Normal
Focal spike with normal background
PVL
Normal
ICH
Not done Infarction Normal
ICH
Abbreviations : CP, cerebral palsy; DD, developmental delay; PVL, periventricular leucomalacia; ICH, in-
tracranial hemorrhage
National Colla- borative Perinatal Project(NCPP)
0.5%
5)Kim
6)0.29%, Kong
7)0.65%
.
8-10)
, 26
24 7
(26.9%), 2-3 6 (23.1%), 4-7
6 (23.1%), 7 (26.9%)
, 73.1%
.
.
11-13)
,
.
23 (88.5%), 3
(11.5%) .
2,500 g 20 (76.9%), 2,500 g 6 (23.1%)
. 26 4
. 1 2
.
14, 15)
, , , ,
, ,
16)
.
9 (34.6%) , 8 (30.8%),
8 (30.8%), 7 (26.9%)
, 8
(30.8%), 2
(7.7%) . ,
,
17)
. ,
25 8 (30.8%)
, 4 (15.4%) .
18)
7 (26.9%) ,
.
2,
19)
, 26 8 (30.8%)
.
.
.
.
Volpe
4), ,
, , ,
.
.
.
, ,
, ,
.
9 (34.6%) ,
7 (26.9%), 5 (19.2%),
3 (11.5%), 2 (7.7%) ,
.
, ,
20)
. ,
,
. ,
.
. phenobarbital, pheny-
toin, benozodiazpine . phe-
nobabrital 1 , pheno-
barbital
. , 2 phe-
nytoin .
benzodiazepine
21-23).
phenobarbital 1
,
phenytoin 1
midazolam ,
.
24)
.
1 1
.
2
4, 21-23)
.
2 (7.7%), 1 8 10 (38.4%), 8
4 (15.4%) 2
.
.
.
,
25-35%
4)
. NCPP
34.8% , 7
70% , 13%
, 19% , 20% , 13
% 2
5).
7 (26.9%) ,
4 (15.4%),
3 (11.5%), 2 (7.7%) ,
1 (3.8%) ,
. 4 (15.4%)
3 6 ,
, ,
.
Volpe
4).
3
18),
, .
.
7 (26.9%) 2 (7.7%)
.
25-27)
. 7 (26.9%)
1 4 (15.4%), 1-3 3
(11.5%) , 2 (7.7%) 10
5 (19.2%) 10
3 10 .
.
,
4, 28, 29)
. 3 (11.5%)
, 3 (11.5%),
2 (7.7%) .
Holden
5)48
% , Legido
25)70% ,
. Lombroso
3)
. 26
24 20 (76.9%)
6 (23.1%), - 4 (15.4%),
3 (11.5%),
3 (11.5%), abundance of sharp transients 1 (3.8%), focal monorhythmic periodic pattern 1
(3.8%), 1 (3.8%),
1 (3.8%) , 4
. 20 (76.9
%) 17 (65.4%) ,
5 (19.2%), 5 (19.2%), -
1 (3.8%), 1 (3.8%) , 5
(19.2%) .
4 (15.4%) ,
5 (19.2%) 4 (15.4%) .
7 (26.9%) 6 (23.1%)
, 6 (23.1%) ,
1 .
,
.
1 2
, ,
.
,
.
.
요 약
목 적 :
.
,
. 방 법 : 1999 1 2008 10
26 ,
,
, , , ,
.
결 과 : 9 (34.6
%) , 7 (26.9%),
5 (19.2%),
3 (11.5%), 2 (7.7
%) . 9 (34.6
%) , 8 (30.8%),
8 (30.8%), 7 (26.9%) ,
8 (30.8%), 2 (7.7%) . 25 19 (73.1%)
8 (31
%), 3 (12%), 4
(15.4%) , 1 (3.8%),
1 (3.8%),
1 (3.8%), 1 (3.8%)
. 26 24
19 (73.1%)
abundance of sharp transients 1 (3.8%), 3 (11.5%),
6 (23.1%),
3 (11.5%), - 4 (15.4%), focal monorhythmic periodic pattern 1 (3.8%),
1 (3.8%), 1
(3.8%) , 4 .
20 (76.9%) 17
(65.4%) ,
5 (19.2%),
5 (19.2%), - 1
(3.8%), 1 (3.8%) , 5 (19.2
%) .
, ,
, phenobarbital 1
phenytoin .
.
결 론 :
1 2
, ,
.
,
.
.
References