The Reliability of Ultrasound-guided Core Needle Biopsy in the Evaluation of Non-palpable Solid Breast Lesions
Using 18-gauge Needles
1Sung-chul Lim, M.D., Young-sook Kim, M.D.2, Nour Sneige, M.D.3
Purpose: Ultrasound-guided core needle biopsy (US CNB) is increasingly used in the histologic evaluation of non-palpable solid breast lesions. We retrospectively investi- gated the diagnostic accuracy of this technique, using an 18-gauge needle in 422 non- palpable breast lesions.
Materials and Methods: 583 female patients with an average age of 56 (range, 22-90) years underwent 590 US CNBs. Between January 1994 and December 1999, using 18- gauge needles, an average of four cores per lesion was obtained. Three hundred and eighty-five lesions were subsequently surgically excised; for 14 of these, the pathologic diagnosis was breast carcinoma metastasis, while 23 with benign diagnoses were clini- cally followed up for ≥2.5 years and were considered for analysis.
Results: Of the 422 lesions, 340 (80.6%) were malignant [308 invasive, 24 ductal carci- noma in situ (DCIS), 7 DCIS with undetermined invasion and 1 DCIS vs. lobular carci- noma in situ], 67 (15.9%) were benign [30 fibroadenoma (FA) and 37 other diagnoses], and five (1.2%) were fibroepithelial lesions. The remaining ten samples (2.4%) includ- ed six cases of atypical ductal hyperplasia (ADH), two of atypical hyperplasia (AH), and two of lobular neoplasia. The sensitivity, specificity, positive predictive value, and negative predictive value of CNBs were 99%, 100%, 100%, and 96%, respectively.
Two cases of invasive carcinoma were missed at CNB; there was no false-positive diag- nosis. Five of six ADHs and one of two AHs were found to be carcinomas (3 DCIS and 3 infiltrating duct carcinomas). Sixteen of 24 (66.7%) cases of DCIS were found at exci- sion to be invasive carcinomas. Of 31 FAs, two (6.5%) were found to be low-grade phyllodes tumor (PT). The five fibroepithelial lesions were shown at excision to be ei- ther PT (n=4) or FA (n=1).
Conclusion: US CNB using an 18-gauge needle is a safe and reliable means of diagnos- ing breast carcinoma. Because of the high prevalence of ductal carcinoma in these le- sions; findings of ADH/AH at US CNB indicate that surgical excision is needed. In or- der to rule out low-grade PT, a diagnosis of FA at CNB requires close follow-up.
Index words : Ultrasound (US) Core needle biopsy Surgery
1Department of Pathology, Chosun University College of Medicine, Kwangju, Korea
2Department of Radiology, Chosun University College of Medicine, Kwangju, Korea
3Department of Anatomic Pathology, The University of Texas M. D. Anderson Cancer Center, Houston, Texas, U.S.A.
Supported in part by research funds from Chosun University, 2003 Received August 16, 2002 ; Accepted February 24, 2003
Address reprint requests to : Sung-chul Lim, M.D., Ph.D., Department of Pathology, Chosun University Hospital, 588 Seosuk-dong, Dong-gu, Kwangju City 501-140, Korea.
Tel. 82-62-230-6343 Fax. 82-62-234-4584 E-mail: [email protected]
The increased detection of non-palpable breast lesions at screening mammography has resulted in the growing use of image-guided core needle biopsies (CNB).
Imaging modalities used in CNB of breast lesions in- clude stereotactic mammography, ultrasound (US) and MRI (1, 2). With advancements in ultrasound technolo- gy, more than 90% of mammographically detected, non- palpable breast masses are identified in this way (3, 4).
The target of US CNB is solid breast masses, which ac- count for two-thirds of non-palpable breast lesions de- tected by screening mammography (5). US CNB is be- coming the first-line guidance technique for CNB in the evaluation of non-palpable solid breast lesions. It can be applied to virtually any mass visualized at sonography, including lesions with inconclusive findings at fine nee- dle aspiration (FNA), and for obtaining histologic confir- mation of carcinoma in order to implement subsequent therapy including preoperative chemotherapy and/or a definitive, one-stage surgical procedure. The advantages of US over stereotactically guided CNB for mass lesions include its relative ease of use (even at the initial visit) and lack of roentgenographic exposure (2, 6). The role of US CNB becomes critical in the diagnosis of lesions not seen on mammograms, such as those in a radiodense breast or at the periphery of the breast close to the chest wall.
Stereotactic CNB is now primarily applied in the biop- sy of lesions with suspicious calcification and masses not identified at sonography. Whereas image-guided CNBs have been extensively studied, most reports have focused on stereotactic CNB, and US CNB alone has rarely been focused on (6, 7). Due to differences be- tween the features of US and stereotactic imaging, the diagnostic accuracy of these two modalities in the imag- ing of breast lesions should be studied separately (8).
With the aim of reducing possible complications, includ- ing local hemorrhage, discomfort and tumor seeding along the needle track, an 18-gauge needle is used for US CNB. It has been reported that the risk of complica- tions correlates with the size of needle used (9-11), and though a smaller (18-gauge) needle is in this respect ad- vantageous, reports have claimed that for CNB diagno- sis, a large needle (14-, or 16-gauge) is more accurate (12, 13).
Using an 18-gauge needle, we retrospectively studied the diagnostic accuracy of US CNB of 422 non-palpable breast lesions.
Materials and Methods
Between January 1994 and December 1999, 583 pa- tients with 590 breast masses visualized at sonography underwent US CNB using an 18-gauge needle. To con- firm that biopsy was indicated, the mammograms were systematically reviewed by an experienced radiologist using standard criteria (14). From 1998, a Mammotome device was used, and for most solid breast lesions with microcalcifications, US CNB was not indicated. CNB was performed by radiologists under direct visualization using a handheld, high frequency (7.5 mHz) linear-array transducer. A spring-loaded biopsy gun with an 18- gauge needle was applied and CNB was repeated in dif- ferent areas of a tumor until a sufficient number of satis- factory cores (average, four per lesion) were obtained.
These were placed in 10% formaline solution and sent for routine processing. Six tissue sections per core, with the first and the last stained with H&E, were obtained and examined by breast pathologists.
The histologic diagnoses of CNB specimens were cate- gorized according to the lesion type: 1) malignant neo- plasms [invasive carcinoma, ductal carcinoma in situ (DCIS) with undetermined invasion, and DCIS]; 2) atyp- ical ductal hyperplasia (ADH)/atypical hyperplasia (AH;
ADH could not be excluded) (ADH/AH); 3) lobular neo- plasia [atypical lobular hyperplasia (ALH) or lobular car- cinoma in situ (LCIS)]; 4) fibroepithelial lesions [phyl- lodes tumor (PT) vs. fibroadenoma (FA)]; and 5) benign lesions (specific types or not otherwise specified).
CNB findings were confirmed on the basis of subse- quent tissue excision (n=385); the presence of metas- tases, confirmed by pathologic examination (n=14) and clinical follow-up by mammography for at least 2.5 years (n=23). The diagnostic outcomes of US CNB were correlated with the follow-up findings. Sensitivity, speci- ficity, and positive and negative predictive value were calculated. Six cases diagnosed at CNB as ADH and two as AH were excluded from the calculation.
Results
The diagnostic results of 590 US CNBs are summa- rized in Table 1. Using an 18-gauge needle, sufficient specimens for adequate diagnosis were obtained.
Rebiopsy due to sampling inadequacy was required in only 3 cases (0.5%).
Confirmation was available for 422/590 CNBs (71.5%)
(Table 1). The pathological findings of US CNB were di- vided into five groups, as follows:
Malignant neoplasia
Table 2 summarizes the subsequent confirmative find- ings of cases in which malignant neoplasms were diag- nosed at US CNB. Among 340 cases, there were 308 in- vasive carcinomas, seven DCIS with undetermined in- vasion, 24 DCIS, and one DCIS vs. LCIS. Among inva- sive carcinoma patients, 294 underwent subsequent breast surgery, at which time the condition was con- firmed in 279 cases. DCIS only was found in six cases, and in the other eight, no residual tumor was identified.
The 14 patients with DCIS, or in whom subsequently obtained surgical specimens revealed no residual tumor, underwent preoperative chemotherapy for inflammato- ry carcinoma (n=1) or their masses were visualized at mammography/sonography (n=13). After chemothera- py, there was either no evidence of a tumor, or preoper- ative mammography/sonography revealed that a small residual tumor was present. In one case, the lesions seen at initial diagnosis were small and clinically non-palpa- ble, and ultrasound showed that two measured 1.3 cm and 0.6 cm, respectively. The diagnosis at US CNB was invasive lobular carcinoma (ILC), and the subsequent surgical specimen indicated DCIS without a residual in- vasive component.
Concurrent or subsequent FNA or extramammary surgical biopsy/excision revealed metastases in 14 of 308 cases, with a US CNB diagnosis of invasive carcinoma.
All these patients underwent preoperative chemothera- py.
Among seven cases diagnosed as DCIS with undeter- mined invasion, invasive carcinoma was found at surgi- cal excision in six (85.7%). Among 24 cases diagnosed as DCIS, invasive carcinoma was found in 16 (66.7%). Six of these had an invasive component measuring ≤5 mm;
in four, the size of this was (1 mm. Analysis of the subse- quent surgical specimen of DCIS vs. LCIS showed that ILC was present.
ADH/AH
At US CNB, six cases of ADH and two of AH were di- agnosed. Subsequent surgery revealed that five (83%) of the six supposed ADH cases and one of the two thought to be AH were in fact carcinomas (3 DCIS, and 3 IDC with extensive DCIS component). Malignant neoplasms thus accounted for 75% of CNBs diagnosed as ADH/
AH.
Lobular neoplasia
One of the two cases diagnosed at US CNB as lobular neoplasia (ALH or LCIS) was found at excision to be in- vasive lobular carcinoma. Examination of the surgical specimen revealed that the tumor was the classic type and that the invasive area measured 0.4 cm in its great- est dimension (0.9 cm at ultrasound).
Fibroepithelial lesions
Five fibroepithelial lesions were diagnosed at CNB.
Four were found at surgical excision to be PT and the other was FA. Two of the PTs were of undetermined malignant potential and one was benign.
Benign lesions
Table 3 summarizes the follow-up results of US CNB at which diagnoses were benign. Eighteen of 31 fi- broadenomas were surgically excised and 13 were fol- lowed-up mammagraphically for 2.5 years or longer.
Excisional biopsy showed that two (underestimation rate, 6.5%) were phyllodes tumor (one of undetermined malignant potential and one benign). Surgical excision of the former revealed the presence of a hyalinized benign component in more than 60% of the lesion, though US
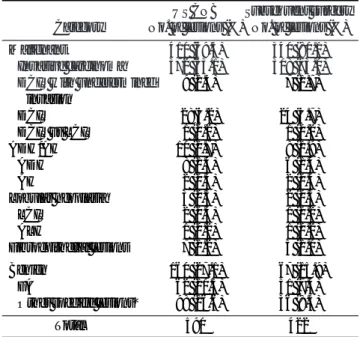
Table 1. Pathologic Diagnosis on 590 Ultrasound Core Needle Biopsies (US CNB) with 422 Subsequent Surgical Confirmation
US CNB Subsequent surgery Category No. of lesions (%) No. of lesions (%)
Malignant 410 (69.5) 340 (80.1)
Invasive carcinoma 372 (63.1) 308 (73.0) DCIS with undetermined 09 (1.5) 07 (1.7)
invasion
DCIS 028(4.2) 24 (5.7)
DCIS vs LCIS 01 (0.2) 01 (0.2)
ADH/AH 10 (1.7) 08 (1.9)
ADH 08 (1.4) 06 (1.4)
AH 02 (0.3) 02 (0.5)
Lobular neoplasia 03 (0.5) 02 (0.5)
LCIS 02 (0.3) 01 (0.2)
ALH 01 (0.2) 01 (0.2)
Fibroepithelial lesions 07 (1.2) 05 (1.0)
Benign 160 (27.1) 067 (15.9)
FA 062 (10.5) 31 (7.4)
Other specific lesions* 098 (16.6) 36 (8.5)
Total 590 422
DCIS: ductal carcinoma in situ, LCIS: lobular carcinoma in situ, ADH: atypical ductal hyperplasia, AH: atypical hyperplasia (can- not exclude ADH), ALH: atypical lobular hyperplasia, FA: fi- broadenoma
*Cyst, ductal hyperplasia without atypia, fat necrosis, lipoma, necrotic adenoma, papilloma, and sclerosing adenosis, fibrocystic changes, inflammation, and/or fibrotic breast parenchyma, etc.
CNB had not indicated this (sampling problem). In nei- ther of the two PTs did CNB revealed the characteristic leaf-like pattern.
In this last group, there was a false negative case. At mammography, the lesion appeared as microcalcifica- tions only, without a mass; ultrasound examination con- firmed the absence of a mass, though a vague elongated hypoechoic area was present. Five US CNBs were ob- tained from this patient, and duct dilatation with mild epithelial hyperplasia and calcification was observed.
Subsequent needle localization excision revealed an in- vasive, moderately differentiated ductal carcinoma, 5
mm in diameter.
The overall sensitivity, specificity, positive predictive value, and negative predictive value of US CNBs in this study were 99%, 100%, 100%, and 96%, respectively.
Two cases of invasive carcinoma were missed at CNB.
There was no false-positive diagnosis.
Discussion
Due to its reliability, lower cost, and lower rates of morbidity and subsequent scarring, core needle biopsy has achieved an established role in reducing the number
Table 2. Subsequent Findings of 340 Cases Diagnosed as Malignant Neoplasms on Ultrasound Core Needle Biopsies (US CNB)
US CNB Diagnosis Subsequent Surgical Specimens Metastases*
Invasive: 308
IDC: 239 IDC: 200 Metastatic site: 12
Mixed IDC & ILC: 6 ILC: 1
Mucinous carcinoma: 1 Tubular carcinoma: 3 DCIS: 6
LCIS: 1 MTPC: 1
No residual tumor: 8
ILC: 37 ILC: 28 Metastatic site: 1
Mixed IDC & ILC: 5 IDC: 2
DCIS: 1
IDC vs. ILC: 9 IDC: 6 Metastatic site: 1
Mixed IDC & ILC: 1 Tubular Ca: 1 Mixed IDC & ILC: 10 Mixed IDC & ILC: 5
IDC: 4 ILC: 1
Tubular Carcinoma: 4 Tubular carcinoma: 3
IDC: 1
Mucinous carcinoma: 6 Mucinous carcinoma: 4
IDC: 1
IDC with mucinous feature: 1
MPC: 1 MPC with invasion: 1
Sarcomatoid carcinoma: 1 Sarcomatoid carcinoma:1
SSC: 1 SSC: 1
DCIS with undetermined invasion: 7 IDC: 6 ICPC: 1
DCIS: 24 IDC: 16
DCIS: 8
DCIS vs LCIS: 1 ILC: 1
IDC: invasive ductal carcinoma, ILC: invasive lobular carcinoma, MPC: micropapillary carcinoma, SSC: sarcomatoid squamous carcino- ma, DCIS: ductal carcinoma in situ, LCIS: lobular carcinoma in situ, MTPC: matrix producing carcinoma, ICPC: intracystic papillary car- cinoma
*Metastases of breast carcinoma confirmed by subsequent pathologic examination.
Nine of these patients underwent preoperative chemotherapy.
of excisional biopsies (15, 16). CNB provides more spe- cific histologic diagnosis than fine needle aspiration, es- pecially for lesions which are difficult to aspirate or where problems arise in determining tumor invasive- ness.
A number of studies have revealed high concordance between CNB using 14-gauge needles and surgical diag- noses of breast palpable and non-palpable solid breast lesions, especially in carcinoma cases (6, 7, 17, 18). No false-positive diagnosis of malignancy has been report- ed, though a low false-negative rate (≤1.7%) did occur (19, 20). Diagnostic sensitivity varied according to nee- dle size. Nath et al. showed that for the diagnosis of ma- lignant lesions, sensitivity was 100%, 92%, and 65% for 14-, 16-, and 18-gauge needles, respectively, and that al- though sensitivity for benign diseases was 100% for all three needle sizes, the number of specific benign diag- noses increased with size (13). For 18-gauge needles, their result was poorer than in the present study, a find- ing which might be explained by the fact that they used short-throw needles, known to harvest significantly less
tissue than long-throw needles and for that reason rec- ommended only occasionally. Using stereotactic CNB and US CNB with 14-gauge needles, Nguyen et al.
achieved a sensitivity of 99% in the diagnosis of breast lesions which were confirmed on the basis of surgery or clinical follow-up (19). Specificity for the diagnosis of breast lesions on the basis of image-guided CNB findings has consistently been 100% in all studies (13, 19, 20).
The decision to perform breast biopsy with larger nee- dles was based on the assumption that breast tissue ob- tained with smaller needles is frequently friable and tends to fragment more often than tissue harvested with 14-gauge needles. However, the results of our study for diagnosing non-palpable solid breast lesions using US 18-gauge CNB show a diagnostic accuracy comparable to that noted in studies in which 14-gauge needles were used. A suggestion supported by our findings is that le- sions in which mammography reveals the presence of microcalcifications frequently consist of friable and fatty tissue (12, 21, 22), both of which are believed to be re- sponsible for incorrect diagnosis with smaller needles (12, 21). We found that was much higher than in earlier reports, and that sensitivity was as high as when larger needles were used. Since 1998, US CNB using an 18- gauge needle has not been indicated in most cases in- volving lesions with microcalcifications. In such cases, larger needles or a Mammotome device have been used.
Our study also highlights three situations that warrant careful evaluation, as discussed below. First, for lesions visualized at sonography there was no false-positive di- agnosis of invasive carcinoma at US CNB. Two cases of invasive carcinoma were, however, missed at US CNB (0.8% false-negative rate). In both, surgical specimens measured 0.4 cm in their greatest dimension, and were not visualized at sonography. Ultrasound is reported to be less accurate for the detection of lesions smaller than 0.6 cm, though mammography-directed US can visual- ize the overwhelming majority of non-palpable masses detected at mammography (1, 7). It is therefore recom- mended that stereotactic mammography should be the preferred method of localization and/or biopsy for most lesions ≤5 mm.
For 16 (67%) of 24 lesions diagnosed as DCIS on the basis of US CNB findings, proof of invasion was provid- ed by the excisional specimen. This prevalence appears higher than that reported in the literature (range, 16- 23%; mean, 19%) (18, 19, 23-25), though a review of our surgical specimens showed that four lesions had on- ly microinvasion (≤0.1 mm in depth). If ‘invasion’ is Table 3. Follow-up Results of 67 Cases with Benign Diagnosis on
Ultrasound Core Needle Biopsy (US CNB)
US CNB Diagnosis Subsequent Surgical Mammography
Diagnosis Follow-up*
FA: 31 FA: 12 No change: 13
ADH: 2 ALH: 1 PT: 2 FCC: 1
DH: 6 DH: 3 No change: 2
IDC: 1
FN: 3 FN: 3
SA: 2 SA: 1
DH: 1
FCC: 1 FCC: 1
Papilloma: 1 Papilloma: 1 Necrotic adenoma: 1 Infarcted lactating
adenoma: 1
Others: 22 FA: 2 No change: 8
FCC: 3 Cyst: 2 DH: 1 LCIS: 2
Others, benign: 4
*Mammography follow-up for 2.5 years or longer
FA: fibroadenoma, DH: ductal hyperplasia, FN: fat necrosis, SA:
sclerosing adenosis, FCC: fibrocystic change, ADH: atypical duc- tal hyperplasia, ALH: atypical lobular hyperplasia, PT: phyllodes tumor, IDC: infiltrating duct carcinoma, LCIS: lobular carcinoma in situ
considered to be >2 mm, the rate of the invasive carci- noma would be reduced to 50% of DCIS, as determined at US CNB. Another possible cause of the higher preva- lence of invasive carcinoma recovery may be the small- er number (average, five) of cores obtained per solid mass lesion visualized at US, as compared to the average number of cores in stereotactic CNB (five per mass le- sion and ten per microcalcification). When DCIS with- out invasive carcinoma is diagnosed at CNB, further his- tologic evaluation by excisional biopsy is, therefore, re- quired.
Second, with regard to atypical hyperplasia, previous reports have addressed the significance of finding ADH at 14-gauge CNB of the breast. In our series, 75% of ADH or AH diagnosed at US 18-gauge CNB were found to be carcinomas, a prevalence consistent with those previously reported (range, 31-88%; mean, 49%) (17, 19, 20, 23, 26-29).
There are two potential explanations for the high inci- dence of discordance between CNB and surgical find- ings for ADH lesions diagnosed at CNB. First, ADH is a histopathologic entity that meets some but not all of the morphologic criteria for DCIS (a diameter of less than 2 mm or involvement of less than two ducts, for example);
because of the small size of CNB, the specimens ob- tained might not, however, satisfy these quantitative cri- teria. Second, because of the heterogeneity of breast le- sions, ADH may be within or near an associated DCIS.
Reported differences in the prevalence of carcinoma in surgical specimens of lesions identified as ADH at CNB may relate to the size of needle used and the num- ber of cores obtained. It has been noted that increasing the number of cores per lesion reduced both the num- ber of ADHs diagnosed at CNB and subsequent histo- logic discordance with the findings of excisional biopsy (4). For a given number of cores, histopathologic diagno- sis is more likely for masses than for lesions with micro- calcification (30); most radiologists now accept that for nodules or densities, a minimum of five cores should be obtained, and for microcalcifications a minimum of ten.
Studies have suggested that better results were ob- tained with 14-gauge needles than with 18-gauge, partic- ularly for biopsy of microcalcifications (13, 30).
Fourteen-gauge needles were used in those studies, while we used 18-gauge only. These aim at reducing possible complications, including local hemorrhage, dis- comfort and tumor seeding along the needle track, the risk of which, according to reports (31-33), correlates with the gauge of needle used. There is, however, some
degree of controversy and doubt as to whether larger needles are as harmless as smaller ones, and whether they cause prohibitive amounts of bleeding (9-11). For this reason, and because of the possible limitations of large-core breast biopsy, some investigators advocate the use of smaller needles. Accordingly, it seems that a comparison between 18-gauge and other needles in terms of their precise reliability would be meaningful.
The target of ultrasound is solid masses that require smaller needles and fewer cores for histologic diagnosis of the same accuracy. Our data indicate that for the di- agnosis of ADH at US CNB, an 18-gauge needle and five cores are suitable; as indicated by earlier studies of stereotactic CNB with findings of ADH, excisional biop- sy is necessary.
Third, with regard to fibroepithelial lesions, two of 31 fibroadenomas in our series, diagnosed at US CNB were found at examination of surgical specimens to be phyl- lodes tumors. One was low grade, with an extensive be- nign hyalinized component, and the other was benign.
In core-needle specimens, the fibrotic stroma was pre- dominant and the focal leaf-like pattern was overlooked.
In most situations, such as the present study and a pre- vious report (34), CNB can be used to distinguish a phyl- lodes tumor from a fibroadenoma, but heterogeneity within a lesion means that more reliable diagnosis is likely to require a larger tissue sample (13).
Examination of surgical specimens showed that five fi- broepithelial lesions diagnosed at US CNB were four phyllodes tumors and one fibroadenoma. Two of PTs were low grade, and two were benign.
In cases of epithelial lesions where diagnosis differs between CNB and the clinical or radiological findings, either excisional biopsy or close follow-up, clinically and radiologically, is, therefore, required.
In summary, US CNB using an 18-gauge needle is a safe and reliable means of diagnosing breast carcinoma in which the findings of ultrasonography are positive.
Diagnostic accuracy is comparable to that of excisional biopsy. Because of the high prevalence of ductal/lobular carcinoma in such lesions, US CNB findings of ADH/
AH and lobular neoplasia indicate that surgical excision is required.
The use of US CNB can avoid many unnecessary open biopsies for benign lesions, while discordance between CNB diagnosis and the clinical and/or radiological find- ings requires close follow-up or excisional biopsy. Our data indicate that for non-palpable solid breast lesions, the overall diagnostic accuracy of US 18-gauge CNB is
comparable to that of standard stereotactic CNB using 14-gauge needles.
References
1. Cross MJ, Evans WP, Peters GN, Cheek JH, Jones RC, Krakos P.
Stereotactic breast biopsy as an alternative to open excisional biop- sy. Ann Surg Onc 1995;2:195-200
2. Liberman L, LaTrenta LR, Dershaw DD, et al. Impact of core biop- sy on the surgical management of impalpable breast cancer. AJR Am J Roentgenol 1997;168:495-499
3. Staren ED, Fine R. Breast ultrasound for surgeons. Am J Surg 1996;
62:108-112
4. Staren ED. Surgical office-based ultrasound of the breast. Am J Surg 1995;61:619-627
5. Miller RS, Adelman RW, Espinosa MH. Dorma SA, Smith DH.
The early detection of nonpalpable breast carcinoma with needle localization. Experience with 500 patients in a community hospi- tal. Am J Surg 1992;58:193-198
6. Parker SH, Jobe WE, Dennis MA, et al. Ultrasound-guided auto- mated large core breast biopsy. Radiology 1993;187:507-511 7. Staren ED. Ultrasound-guided biopsy of nonpalpable breast mass-
es by surgeons. Ann Surg Oncol 1996;3:476-482
8. Kopans DB. Caution on core (comment). Radiology 1994;193:325- 326
9. Dowlatshahi K, Yaremko ML, Kluskens LF, Jokich PM.
Nonpalpable breast lesions: findings of stereotaxic needle-core biopsy and fine-needle aspiration cytology. Radiology 1991;181:
745-750
10. Jackson VP, Reynolds HE. Stereotaxic needle-core biopsy and fine- needle aspiration cytologic evaluation of nonpalpable breast le- sions. Radiology 1991;181:633-634
11. Dowlatshahi K, Yaremko ML, Kluskens LF, Jokich PM. Nonpal- pable breast lesions: findings of stereotaxic needle-core biopsy and fine-needle aspiration cytology. Radiology 1991;181: 745-750 12. Helbich TH, Rudas M, Haitel A, et al. Evaluation of needle size for
breast biopsy: comparison of 14-, 16-, and 18-gauge biopsy nee- dles. AJR Am J Roentgenol 1998;171:59-63
13. Nath ME, Robinson TM, Tobon H, Chough DM, Sumkin JH.
Automated large-core needle biopsy of surgically removed breast lesions: comparison of samples obtained with 14-, 16-, and 18- gauge needles. Radiology 1995;197:739-742
14. Svane G, Potchen EJ, Sierra A, Azavedo E. Screening mammogra- phy: breast cancer diagnosis in asymptomatic women. St. Louis:
Mosby, 1993
15. Fornage BD, Coan JD, David CL. Ultrasound-guided needle biop- sy of the breast and other interventional procedures. Radiol Clin North Am 1992;30:167-185
16. Parker SH, Stavros AT, Dennis MA. Needle biopsy techniques.
Radiol Clin North Am 1995;33:1171-1186
17. Dahlstrom JE, Sutton S, Jain S. Histological precision of stereotac-
tic core biopsy in diagnosis of malignant and premalignant breast lesions. Histopathology 1996;28:537-541
18. Pijnappel RM, van Dalen A, Rinkes IH, van den Tweel JG, Mali WP. The diagnostic accuracy of core biopsy in palpable and non- palpable breast lesions. Eur J Radiol 1997;24:120-123
19. Nguyen M, McCombs MM, Ghandehari S, et al. An update on core needle biopsy for radiologically detected breast lesions.
Cancer 1996;78:2340-2345
20. Seoudi H, Mortier J, Basile R, Curletti E. Stereotactic core needle biopsy of nonpalpable breast lesions: initial experience with a promising technique. Arch Surg 1998;133:366-372
21. Parker SH, Lovin JD, Jobe WE, et al. Stereotactic breast biopsy with a biopsy gun. Radiology 1990;176:741-747
22. Burbank F, Belville J. Core breast biopsy, research, and what not to do. Radiology 1992;185:639-640
23. Jackman RJ, Nowels KW, Shepard MJ, Finkelstein SI, Marzoni FA Jr. Stereotaxic large-core needle biopsy of 450 nonpalpable breast lesions with surgical correlation in lesions with cancer or atypical hyperplasia. Radiology 1994;193:91-95
24. Burbank F. Stereotactic breast biopsy of atypical ductal hyperpla- sia and ductal carcinoma in situ lesions: improved accuracy with directional, vacuum-assisted biopsy. Radiology 1997; 202:843-847 25. Liberman L, Dershaw DD, Rosen PP, et al. Stereotaxic core biopsy
of breast carcinoma: accuracy at predicting invasion. Radiology 1995;194:379-381
26. Liberman L, Cohen MA, Dershaw, DD, Abramson, AF, Hann LE, Rosen PP. Atypical ductal hyperplasia diagnosed at stereotaxic core biopsy of breast lesions: an indication for surgical biopsy. AJR Am J Roentgenol 1995;164:1111-1113
27. Gadzala DE, Cederbom GJ, Bolton JS, et al. Appropri-ate manage- ment of atypical ductal hyperplasia diagnosed by stereotactic core needle breast biopsy. Ann Surg Oncol 1997;4:283-286
28. Moore MM, Hargett CW 3rd, et al. Association of breast cancer with the finding of atypical ductal hyperplasia at core breast biop- sy. Ann Surg 1997;225:726-733
29. Brown TA, Wall JW, Christensen ED, et al. Atypical hyperplasia in the era of stereotactic core needle biopsy. J Surg Oncol 1998;67:
168-173
30. Liberman L, Dershaw DD, Rosen PP, Abramson AF, Deutch BM, Hann LE. Stereotaxic 14-gauge breast biopsy: how many core biopsy specimens are needed? Radiology 1994;192:793-795 31. Youngson BJ, Liberman L, Rosen PP. Displacement of carcinoma-
tous epithelium in surgical breast specimens following stereotaxic core biopsy. Am J Clin Pathol 1995;103:598-602
32. Smith EH. Complications of percutaneous abdominal fine-needle biopsy. Radiology 1991;178:253-258
33. Roussel F, Dalion J. The risk of tumoral seeding in needle biopsies.
Acta Cytol 1989;33:936-939
34. Florentine BD, Cobb CJ, Frankel K, Greaves T, Martin SE. Core needle biopsy. A useful adjunct to fine-needle aspiration in select patients with palpable breast lesions. Cancer (Cancer Cytopathol) 1997;81:33-39
대한방사선의학회지 2003;48:353-360
비촉지성 유방 고형종괴의 18게이지 생검침을 이용한 초음파 유도하 핵생검의 신뢰도1
1조선대학교 의과대학 병리학교실
2조선대학교 의과대학 진단방사선과학교실
3Department of Anatomic Pathology, The University of Texas M.D.
Anderson Cancer Center, Houston, Texas, U.S.A.
임성철・김영숙2・Nour Sneige3
목적:유방의 비촉지성 고형종괴의 진단에 초음파 유도하 핵 생검이 널리 이용되고 있다. 저자들은 핵 생검 후 진단이 확인된 422예를 대상으로 후향적 분석을 통하여 비촉지성 유방병변에 대한 18게이지 생검침의 유용성을 알아보고자 하였다.
대상과 방법:1994년 1월부터 1999년 12월까지 시행된 초음파 유도하 핵 생검중 18게이지 생검침을 이용한 590예
(583환자)를 대상으로 하였다. 병변당 생검 횟수는 평균 4회 시행하였다. 이중385예는 뒤이어 시행한 외과적 절제 생 검으로 확인되었으며, 14예는 다른 부위에 전이된 유방암이 확인된 경우이며, 23예는 2.5년 이상의 임상 추적을 통해 양성 병변으로 진단이 확인된 경우이다.
결과:422예중 340예(80.6%)는 악성(침습성 308예, 관내암종 24예, 침습여부 미결정 관내암종 7 예, 그리고 관내암 종과 소엽내암종의 감별이 필요한 1예), 67예(15.9%)는 양성(섬유선종 30예, 기타 37예), 그리고 5예(1.2%)는 섬유 상피성 병변이었다. 그리고, 나머지 10예(2.4%)는 비정형 관상피증식증 6예, 비정형 증식증 2예, 그리고 소엽종양 2예 이었다. 민감도, 특이도, 양성 예측도, 음성 예측도는 각각 99%, 100%, 100%, 그리고 96%이었다. 2예의 침습성 암이 핵 생검에서 발견되지 않았으나 위양성으로 진단된 예는 없었다. 6예의 비정형 관상피증식증 중 5예, 그리고 2예의 비 정형 증식증 중 1예에서 암(관내암종 3예, 침윤성 관암종 3예)이 발견되었다. 24예의 관내암종 중 16예가 외과적 절제 상 침윤성 암이 있었다. 31예의 섬유선종 중 2예(6.5%)는 저등급 엽상종양으로 밝혀졌으며, 5예의 섬유상피성 병변은 절제생검상 4예는 엽상종양, 1예는 섬유선종으로 밝혀졌다.
결론:비촉지성 유방 고형종괴의 초음파 유도하 18게이지 생검침을 이용한 핵생검은 안전하며 신뢰할 수 있다. 핵 생검 상 비정형 관상피증식증/비정형 증식증은 관암종의 발생빈도가 높기 때문에 외과적 절제의 적용대상이고, 섬유선종의 경우 저등급 엽상종양을 감별하기위한 면밀한 추적이 필요하다.