Pediatric patients with cerebral palsy are likely to suffer severe pain postoperatively. Muscle spasticity can be increased by pain stimuli, and may further increase pain to create a vi- cious cycle. Moreover, difficulties in pain assessment associat- ed with poor verbal communication skills and the concerns of parents and medical personnel about the side effects of anal- gesics may result in insufficient pain control6,17).
Although several methods of reducing pain and spasticity have been proposed in non-operatively treated patients with cerebral palsy1,4,14,18), adequate and specialized methods of po- stoperative pain management in this group of patients have yet to be established. In this study, we evaluated the efficacy and safety of intravenous patient-controlled analgesia (PCA) with fentanyl and ketorolac versus the pethidine-based con-
ventional analgesic method after orthopaedic surgical pro- cedures.
MATERIALS AND METHODS
Of the 88 patients with cerebral palsy who underwent or- thopaedic surgery of the lower extremity between June 2001 and December 2001, 68 were included in this prospective study. The inclusion criteria included; five years of age or ol- der, capable of verbal communication, and absence of a sen- sory deficit or mental retardation. Of these 68 patients, eight were excluded during the study, because of non-cooperation (n=5) or early hospital discharge (n=3), which left 60 patients (23 females and 37 males) for analysis. Mean patient age was 8.5 years (range 5.0-14.8). Fifty-six patients had the spastic type and four mixed type cerebral palsy. Thirty-five had diple- gia, 13 hemiplegia, 9 quadriplegia, 2 triplegia and 1 paraple- gia, and all were of grade 1 according to the American Soci- ety of Anesthesiologists physical status grading system.
Patients were divided into either a minor operation group which involves soft tissue procedures only, or a major opera-
544 544
Intravenous Patient-controlled Analgesia for Postoperative Pain Management in Patients with Cerebral Palsy
Won Joon Yoo, M.D., Chin Youb Chung, M.D., In Ho Choi, M.D., Tae-Joon Cho, M.D., Joon O Lee, Hee-Soo Kim, M.D.*, and Chong Sung Kim, M.D.*
Departments of Orthopaedic Surgery and Anesthesiology*, Seoul National University Hospital, Seoul, Korea
544 544 Address reprint requests to
Chin Youb Chung, M.D.
Department of Orthopaedic Surgery, Seoul National University Bundang Hospital, 300 Gumi-dong, Bundang-gu, Seongnam 463-707, Korea
Tel: +82.31-787-2200, Fax: +82.31-787-2204 E-mail: [email protected]
*No financial support was received for this study.
Purpose: The purpose of this study was to evaluate the safety and efficacy of intravenous patient-controlled analgesia (PCA) with fentanyl and ketorolac for postoperative pain management in patients with cerebral palsy.
Materials and Methods: Sixty patients were categorized based on operation complexity into either a minor operation group or a major operation group, and then subdivided based on the analgesic methods used, i.e., intravenous PCA with fentanyl and ketorolac or intravenous pethidine injection. Pain intensity was assessed using the Wong-Baker,
s faces pain scale.
Results: In the major operation group, patients that received PCA had significantly lower pain scores than those who received intravenous pethidine injection, while no significant differences in pain scores were ob- served in the minor operation group. Moreover, the side effects of these two analgesic methods did not differ significantly.
Conclusion: Intravenous PCA with fentanyl and ketorolac is effective and safe for moderate to severe post- operative pain control in pediatric patients with cerebral palsy.
Key Words: Intravenous patient-controlled analgesia, Fentanyl, Ketorolac, Pethidine, Postoperative pain, Cerebral palsy
tion group which includes osteotomies and soft tissue proce- dures. The patients were then further subdivided based on the analgesic method used into intravenous PCA with fen- tanyl and ketorolac, or intravenous pethidine injection. Pa- tients were matched in these groups for age and sex. Summa- rizing, the 60 patients were allocated to four groups: group I (minor operation/PCA, n=16), group II (minor operation/
pethidine, n=18), group III (major operation/PCA, n=14), and group IV (major operation/pethidine, n=12) (Table 1).
The PCA unit was composed of a basal infusor and a pa- tient control module (AutoMed 3,300�, Ace Medical Inc., Seoul, Korea). The PCA regimen used was fentanyl citrate (15 mcg/kg) and ketorolac tromethamine (2.5 mg/kg) mixed in D5W to a total volume of 50 mL. Drugs were infused con- tinuously at the rate of 0.4 mL/hr and a bolus amount of 0.6 mL/injection was administered by button pressing. The ‘lock out’ time interval between allowed bolus deliveries was set at 15 min. PCA drug administration commenced immedi- ately after a patient left the recovery room. Pethidine HCl was administered intravenously at 1 mg/kg (maximum 40 mg) whenever patient or parent required, but with a mini-
mum injection interval of four hours. All patients were given the antispasmodic, diazepam, at a daily dose of 0.2 mg/kg.
Pain intensity was assessed at two hours postoperatively, and then every six hours for 50 hr using the Wong-Baker faces pain scale17)(Fig. 1). The total amount of drugs deliv- ered by the PCA system was determined by adding the bolus volume to the basal infusion volume over 50 hr postoperative- ly, and the total amount of pethidine injected was calculated from the number of the injections recorded on medical charts.
Any side effects such as respiratory depression, nausea, vomit- ing, somnolence, itching, and headache were notified to the doctor on duty and recorded.
Pain scores by the analgesic methods were compared for each operation group. Repeated ANOVA (SPSS version 10.0, SPSS Institute, Chicago, USA) was used for the statistical analysis, and p values of <0.05 were considered statistically significant.
RESULTS
In the major operation group, PCA with fentanyl and ke- torolac produced significantly lower pain scores than pethi-
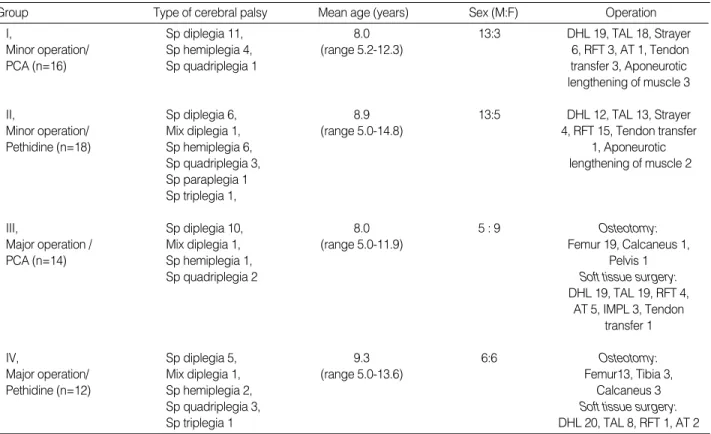
Sp, spastic; Mix, mixed; DHL, distal hamstring lengthening; TAL, Achilles tendon lengthening; RFT, rectus femoris transfer; AT, adductor tenotomy; IMPL, intramuscular psoas lengthening; PCA, patient-controlled analgesia.
Group Type of cerebral palsy Mean age (years) Sex (M:F) Operation
I, Sp diplegia 11, 8.0 13:3 DHL 19, TAL 18, Strayer
Minor operation/ Sp hemiplegia 4, (range 5.2-12.3) 6, RFT 3, AT 1, Tendon
PCA (n=16) Sp quadriplegia 1 transfer 3, Aponeurotic
lengthening of muscle 3
II, Sp diplegia 6, 8.9 13:5 DHL 12, TAL 13, Strayer
Minor operation/ Mix diplegia 1, (range 5.0-14.8) 4, RFT 15, Tendon transfer
Pethidine (n=18) Sp hemiplegia 6, 1, Aponeurotic
Sp quadriplegia 3, lengthening of muscle 2
Sp paraplegia 1 Sp triplegia 1,
III, Sp diplegia 10, 8.0 5 : 9 Osteotomy:
Major operation / Mix diplegia 1, (range 5.0-11.9) Femur 19, Calcaneus 1,
PCA (n=14) Sp hemiplegia 1, Pelvis 1
Sp quadriplegia 2 Soft tissue surgery:
DHL 19, TAL 19, RFT 4, AT 5, IMPL 3, Tendon
transfer 1
IV, Sp diplegia 5, 9.3 6:6 Osteotomy:
Major operation/ Mix diplegia 1, (range 5.0-13.6) Femur13, Tibia 3,
Pethidine (n=12) Sp hemiplegia 2, Calcaneus 3
Sp quadriplegia 3, Soft tissue surgery:
Sp triplegia 1 DHL 20, TAL 8, RFT 1, AT 2
Table 1.Demographic data of the 60 patients
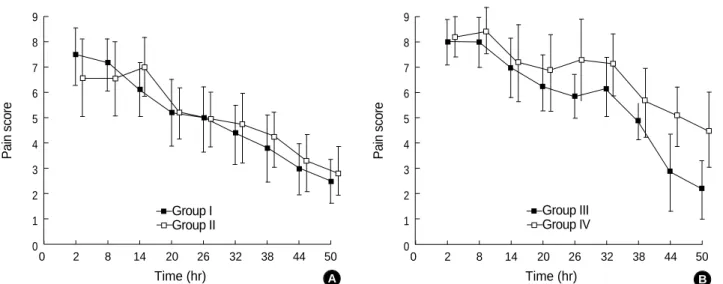
dine injection (p=0.032). Initially, the pain scores of the two analgesic methods were similar, but the pain relieving effect of the PCA method became significantly superior to that of pethidine injection at 20 hr postoperatively and this was sus- tained (p=0.031). In the minor operation group, the pain control achieved by the two analgesic methods was similar (Fig. 2). The total doses of drugs administered are shown in Table 2. Side effects such as nausea, vomiting, somnolence, itching, headache, and respiratory depression occurred infre- quently, and they did not differ significantly by analgesic me- thod (Table 3). In no case were the side effects severe enough for the drug administration to be changed or stopped.
DISCUSSION
Ketololac coadministration with intravenous fentanyl PCA resulted in reduced pain ratings after total hip replacement surgery9)or radical retropubic prostatectomy5). Prolongation of bleeding time caused by the inhibition of prostaglandin synthesis, which occurs with ketorolac and other NSAIDs
may be associated with gastrointestinal ulceration and an increased risk of acute renal failure in some clinical condi- tions7). In major orthopedic surgery, however, there is no evi- dence of an interaction with NSAIDs that could increase po- stoperative blood loss21). Several reports have shown that ke- torolac has an opioid-sparing effect in pain management after orthopaedic surgery3,20,22). Fentanyl has a high protein bind- ing capacity, about 84% is protein bound in vivo13), and ke- torolac is approximately 99.2% bound to plasma albumin15). Thus, ketorolac may compete with fentanyl for protein bind- ing and possibly potentiate the action of fentanyl by increas- ing the unbound fraction of fentanyl, as other non-steroid
Fig. 1.Wong-Baker’s faces pain scale. This scale employs six faces with expressions ranging from smiling to a sad face with tears. Below the faces were even numbers from zero (smiling) to 10 (sad face with tears) which represented numerical ratings of pain.
0 2 4 6 8 10
9 8 7 6 5 4 3 2 1
00 2 8 14 20 26 32 38 44 50
Time (hr)
Painscore
9 8 7 6 5 4 3 2 1
00 2 8 14 20 26 32 38 44 50
Time (hr)
Painscore
Group I Group II
Group III Group IV
Fig. 2.Postoperative changes in pain scores by analgesic method. (A) Minor operation group. (B) Major operation group. Error bar shows 95% confidence interval of means.
PCA, patient-controlled analgesia; N, none.
Group
Group I 8.71 1.45 N
Group II N N 3.33
Group III 10.89 1.82 N
Group IV N N 5.30
Table 2.Total dose of drugs administered
Fentanyl (mcg/kg) Ketorolac (mg/kg)
Pethidine (mg/kg) PCA
A B
PCA, patient-controlled analgesia.
Respiratory depression 0 0
Nausea 6 4
Vomiting 1 2
Somnolence 0 1
Itching 0 0
Headache 3 1
Table 3.Side effects
PCA with fentanyl and ketorolac
Intravenous pethidine
anti-inflammatory drugs11).
We assessed pain using a self reporting method, the Wong- Baker faces pain scale. Several studies have confirmed the validity and reliability of this scale for children8,16,19). It is gen- erally accepted that self reporting is the most effective method of pain measurement, and that children older than five years can reliably self report pain intensity12). Other pain assessing parameters like behavioral scoring or the length of hospital stay could not be used in this study, because many patients were placed in a cast or an immobilizer postoperatively, and hospital stay might have been determined by factors like po- stoperative fever, wound problems, or secondary procedures.
Surgical procedures performed in groups I and II were sim- ilar in terms of number, procedure complexity, and expected pain. However, a larger number of operations on soft tissues were performed in group III (mean 3.6 operations/patient) than in group IV (mean 2.6 operations/patient) while osteoto- my complexities were similar in group III (19 femoral, 1 cal- caneal, and 1 pelvic osteotomies) and group IV (13 femoral, 3 tibial, and 3 calcaneal osteotomies). Therefore, the statis- tical results strongly suggest that the analgesic effect of PCA with fentanyl and ketorolac is superior to that of pethidine by injection for major operations. In contrast, the relative infusion amount of pethidine to fentanyl in the minor oper- ation group (3.33/8.71, 38.2%) was lower than that in the major operation groups (5.30/10.89, 48.7%), while the anal- gesic effects of the two methods were similar in the minor operation groups. In addition, three of the 18 patients in group II did not need any pain control. These findings sug- gest that conventional on demand pethidine injections may still be an appropriate analgesic method for patients under- going minor operations involving soft tissue procedures only.
However, caution should be exercised concerning the pro- longed use of pethidine, because it has been associated with seizure occurred at high doses, and with other central ner- vous system toxicities, such as, nervousness, hyperreflexia, tremors and myoclonus2,10).
In view of finding that the analgesic benefit of the PCA method was not apparent until 20 hr after major operation and that an unnecessary amount of drug was administered due to the continuous basal infusion setting of the PCA sys- tem in minor operations, some modification of the current PCA method, including changes in drug concentration, drug regimen, and basal flow rate may be justified.
CONCLUSION
In conclusion, intravenous PCA with fentanyl and ketorolac was found to be an effective and safe modality for moderate to severe pain control after orthopaedic surgery in pediatric patients with cerebral palsy. However, in minor operations where mild pain is expected, it appears not to have a definite advantage over conventional ‘on demand’ pethidine injection.
REFERENCES
1. Albright AL, Barron WB, Fasick MP, Polinko P and Janosky J:Continuous intrathecal baclofen infusion for spasticity of cerebral origin. JAMA, 270: 2475-2477, 1993.
2. Beaule PE, Smith MI and Nguyen VN: Meperidine-induced seizure after revision hip arthroplasty. J Arthroplasty, 19: 516-519, 2004.
3. Eberson CP, Pacicca DM and Ehrlich MG: The role of ketoro- lac in decreasing length of stay and narcotic complications in the postoperative pediatric orthopaedic patient. J Pediatr Orthop, 19:
688-692, 1999.
4. Gilmartin R, Bruce D, Storrs BB, et al: Intrathecal baclofen for management of spastic cerebral palsy: Multicenter trial. J Child Neu- rol, 15: 71-77, 2000.
5. Grass JA, Sakima NT, Valley M, et al: Assessment of ketorolac as an adjuvant to fentanyl patient-controlled epidural analgesia after radical retropubic prostatectomy. Anesthesiology, 78: 642-648, 1993.
6. Gureno MA and Reisinger CL: Patient controlled analgesia for the young pediatric patient. Pediatr Nurs, 17: 251-254, 1991.
7. Insel PA: Analgesic-antipyretics and anti-inflammatory agents;
drugs employed in the treatment of rheumatoid arthritis and gout.
In: Goodman LS, Gilman A, Rall TW, Nies AS, Taylor P, eds. Good- man and Gilman’s the pharmacologic basis of therapeutics. Elms- ford, NY: Pergammon Press, 642, 1990.
8. Keck JF, Gerkensmeyer JE, Joyce BA and Schade JG: Reliabil- ity and validity of the Faces and Word Descriptor Scales to measure procedural pain. J Pediatr Nurs, 11: 368-374, 1996.
9. Kostamovaara PA, Hendolin H, Kokki H and Nuutinen LS:
Ketorolac, diclofenac and ketoprofen are equally efficacious for pain relief after total hip replacement surgery. Br J Anaesth, 81: 369-372, 1998.
10. Latta KS, Ginsberg B and Barkin RL: Meperidine: a critical re- view. Am J Ther, 9: 53-68, 2002.
11. Lotsch J, Skarke C, Tegeder I and Geisslinger G: Drug inter- actions with patient-controlled analgesia. Clin Pharmacokinet, 41:
31-57, 2002.
12. McGrath PJ, de Veber LL and Hearn MT: Multidimensional pain assessment in children. In: Fields HL (ed) Advances in pain research and therapy, Raven Press, New York, 387-393, 1986.
13. Meuldermans WE, Hurkmans RM and Heykants JJ: Plasma protein binding and distribution of fentanyl, sufentanil, alfentanil and lofentanil in blood. Arch Int Pharmacodyn Ther, 257: 4-19, 1982.
14. Meythaler JM, DeVivo MJ and Hadley M: Prospective study on the use of bolus intrathecal baclofen for spastic hypertonia due to acquired brain injury. Arch Phys Med Rehabil, 77: 461-466, 1996.
15. Mroszczak EJ, Lee FW, Combs D, et al: Ketorolac tromethamine absorption, distribution, metabolism, excretion, and pharmacokinet- ics in animals and humans. Drug Metab Dispos, 15: 618-626, 1987.
16. Robertson J: Pediatric pain assessment: validation of a multidi- mensional tool. Pediatr Nurs, 19: 209-213, 1993.
17. Rodgers BM, Webb CJ, Stergios D and Newman BM: Pa- tient-controlled analgesia in pediatric surgery. J Pediatr Surg, 23:
259-262, 1988.
18. Scheinberg A, O’Flaherty S, Chaseling R and Dexter M: Con- tinuous intrathecal baclofen infusion for children with cerebral palsy:
a pilot study. J Paediatr Child Health, 37: 283-288, 2001.
19. Stein PR: Indices of pain intensity: construct validity among pres- choolers. Pediatr Nurs, 21: 119-123, 1995.
20. Sutters KA, Shaw BA, Gerardi JA and Hebert D: Compari- son of morphine patient-controlled analgesia with and without ke- torolac for postoperative analgesia in pediatric orthopaedic surgery.
Am J Orthop, 28: 351-358, 1999.
21. Toon S, Holt BL, Mullins FG, Bullingham R, Aarons L and Rowland M:Investigations into the potential effects of multiple dose ketorolac on the pharmacokinetics and pharmacodynamics of racemic warfarin. Br J Clin Pharmacol, 30: 743-750, 1990.
22. Vetter TR and Heiner EJ: Intravenous ketorolac as an adjuvant to pediatric patient-controlled analgesia with morphine. J Clin Ane- sth, 6: 110-113, 1994.
목 적: 뇌성마비 환자에서 fentanyl과 ketorolac을 이용한 경정맥 자가 통증 치료법(intravenous patient-controlled analgesia) 의 수술 후 통증 조절에 대한 안전성과 효용성을 평가하고자 하였다.
대상 및 방법: 60명의 환자를 대상으로 수술의 복잡성에 따라 대 수술과 소 수술로 나누어 두 군으로 분류하였고 각 군을 수 술 후 통증 조절 방법에 따라 fentanyl과 ketorolac을 이용한 경정맥 자가 통증 치료법을 사용한 군과 pethidine정맥 주사를 사용한 군으로 세분하였다. 통증의 강도는 Wong-Baker,
s faces pain scale에 따라 평가하였다.
결 과: 대 수술군에서는 경정맥 자가 통증 치료법을 사용한 환자군에서 pethidine을 사용한 환자군보다 유의한 통증의 감소 가 있었고 소 수술군에서는 경정맥 자가 통증 치료법을 사용한 환자군과 pethidine을 사용한 환자군 사이에 유의한 통증 감 소 효과의 차이는 없었다. Fentanyl과 ketorolac을 이용한 경정맥 자가 통증 치료법과 pethidine정맥 주사 요법에 따른 부 작용은 큰 차이를 보이지 않았다.
결 론: Fentanyl과 ketorolac을 이용한 경정맥 자가 통증 치료법은 뇌성마비 소아 환자에서 수술 후 중등도 이상의 통증 조절 에 있어 안전하고 효과적이다.
색인 단어: 경정맥 자가 통증 치료법, Fentanyl, Ketorolac, Pethidine, 수술 후 통증, 뇌성마비
뇌성마비 환자에서 수술 후 통증 조절을 위한 경정맥 자가 통증 치료법
유원준ㆍ정진엽ㆍ최인호ㆍ조태준ㆍ이준오ㆍ김희수*ㆍ김종성*
서울대학교 의과대학 정형외과학교실, 마취통증의학교실*