Repeat Hepatectomy of Recurrent Tuberculous Hepatic Abscess
4
0
0
전체 글
(2) 백낙원 외 : 수술 절제 후 재발된 결핵성 간농양의 재절제 치료 경험. 519. ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ. A. A. B. B. A. mg/dl, BUN 9.3 mg/dl, creatinine 0.7 mg/dl이었고, 전해질 검 사상 Na 144 mEq/l, K 4.2 mEq/l이었으며 객담검사상 항상 균 검사는 음성이었다. 방사선학적 소견상 내원 당시 흉부방사선 검사에서는 정. B. Fig. 1. (A) Fistulogram revealed fistula cavity and its connection with hepatic vein. (B) Cross section view of specimen shows yellowish abscess cavity.. Fig. 2. (A) Previous CT scan shows a 4×6 cm sized abscess lesion in right lobe of liver. (B) Preoperative CT scan shows enlarging multifocal cystic lesion, about 6×8 cm sized, than previous one.. Fig. 3. (A) A scene of operation. (B) 8×6.5 cm sized yellowish cystic mass lesion at cross section view of specimen.. 상 소견이였고, 복부 전산화 단층촬영상 간우엽 8분절에서 8×6 cm 크기의 다발성 농양 소견을 보였다. 이 농양은 6개 월 전보다 증대된 것으로 나타났다(Fig. 2). 이에 수술적 치 료를 시행하기로 결정되어 간 우엽 절제술을 시행하였다..
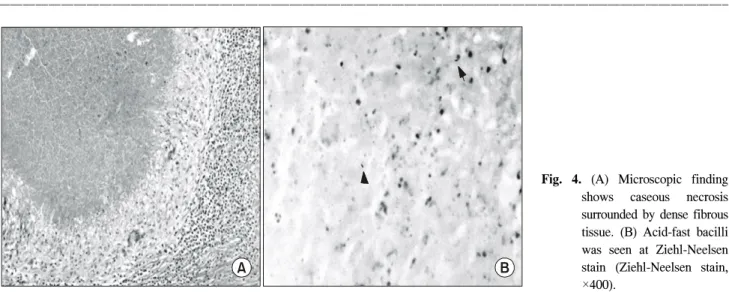
(3) 520. 대한외과학회지 : 제 68 권 제 6 호 2005. ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ. A. 병리 소견상 육안으로 8×6.5 cm 크기의 종괴가 관찰되었 고(Fig. 3), 단면에서는 황색의 농양 양상의 내용물과 건락 괴사 변형(caseous necrotic change) 내용물을 포함한 다발성 농양으로 확인되었으며, 간 실질 세포는 정상소견이었다. 농양은 Ziehl-Neelsen염색상 항산균 양성으로 나타났다(Fig. 4). 환자는 술 후 7일째부터 3차 항결핵 약물 투여를 시작하 여 현재 prothionamide 500 mg, cycloserine 750 mg 투여 중이 다.. 고. 찰. 폐외 결핵(extrapulmonary tuberculosis)은 위장관, 장간막, 복막, 간, 비장, 임파선, 신장과 요로, 췌장 등에 흔한 것으로 알려져 있고,(2,3) 폐결핵 환자인 경우 약 15∼20%에서 폐 외 결핵이 병발하는 것으로 보고되고 있다.(3,4) 간에서 발생하는 결핵은 드문 질환으로 미만성 폐결핵을 앓고 있는 환자나 후천성 면역 결핍증 환자에서 주로 관찰 되고, 신체의 다른 부위에 동반된 폐외 결핵에 의해 2차적 으로 발생하는 것이 대부분이며,(2,4) 주로 위장관 결핵이 원발병소이다.(5) 간결핵이 폐결핵에 의한 2차적으로 발생 한 경우는 약 13%로 보고되고 있다.(6) 간결핵은 임상적으로 원발성 간결핵과 2차성 간결핵으 로 분류하고 원발성 간결핵은 망상내피계에 결핵균이 침범 하여 발생되며 간과 국소임파절에 국한되어 있는 경우이 며, 2차성 간결핵은 원래의 오래된 결핵 병소가 재활성화되 는 경우를 말한다. 이 경우는 주로 간동맥 또는 문맥을 통한 혈행성 파급으로 이환되며 드물게는 림프관을 통해서도 병 소를 유발하기도 한다.(7) 임상 증상은 비특이적인 우상복부 동통과 발열, 기면, 오 심, 식욕감퇴, 체중감소 및 복통 등이 있고, 신체적 검사상 상복부 압통 및 간종대 소견이 관찰될 수 있다.(8) 간기능 검사 소견으로 저알부민증, AST와 ALT, ALP, 감마글로브. B. Fig. 4. (A) Microscopic finding shows caseous necrosis surrounded by dense fibrous tissue. (B) Acid-fast bacilli was seen at Ziehl-Neelsen stain (Ziehl-Neelsen stain, ×400).. 린 등이 상승되며, 혈액학적 소견으로 적혈구 침강속도 증 가, 범혈구 감소증, 비기능 항진 등의 소견이 나타날 수 있 다. 방사선학적으로는 전산화 단층촬영 소견상 저음영의 다발성 종괴로 보이는데 초기에는 격막이 있으며 경계가 불분명하기 때문에 농양과 같은 양상을 보이지만, 진행되 면 중심부가 균일해지면서 석회화 소견이 나타날 수 있 다.(9) 간결핵의 진단에 있어서 임상증상이나 검사실 소견, 방 사선학적 소견상 특이한 것이 없으므로 간생검이 가장 진 단적 가치가 높고 약 75∼83%의 양성율을 보이는 것으로 알려져 있고,(10,11) 간조직에서 결핵균이 발견되지 않는 경 우에는 PCR (polymerase chain reaction)로 확진할 수 있 다.(12,13) Essop 등(14)은 간결핵의 확진 기준을 간조직에서 항산균의 검출, 간조직 배양시 결핵균의 양성반응, 건락성 괴사(caseation necrosis)와 Mantoux 반응의 양성, 간의 육아 종성 염증과 다른 장기에서 결핵균의 검출, 복강내의 특이 한 소견, 부검에 의한 확인, 항결핵제 투여후 증세호전 등의 7가지로 보고하였다. Terry와 Gunnor(15)는 원인을 알 수 없 는 지속적인 발열, 간비대, 비장종대, 복부 팽만감, 복수, 설 명할 수 없는 혈청 감마글로블린 증가 등이 있는 경우에는 간결핵을 강력히 의심해야 한다고 하였다. 간에서 육아성 병변을 일으키는 가장 흔한 형태는 결핵균 감염이라고 보 고가 있으며(10) 우리나라의 경우 유육종증, 브루셀라증, 진 균질환 등이 드물기 때문에 간생검에서 발견된 만성 육아 종은 대부분 간 결핵의 가능성을 고려하여야 한다.(16) 간결핵은 항결핵제 약물요법으로 약 85%에서 완치될 수 있으므로 대개의 경우 약물요법이 원칙이긴 하지만, 크기 가 크고 국소성 결핵종인 경우이거나 항결핵제 약물요법에 반응이 없거나 합병증이 병발될 때, 크기가 증가할 때에는 경피적 배농술이나 외과적 절제가 필요하다.(17) 우리나라 에서도 원발성 간결핵 낭종을 외과적 절제를 시행한 증례 가 보고된 바 있다.(18,19).
(4) 백낙원 외 : 수술 절제 후 재발된 결핵성 간농양의 재절제 치료 경험. 521. ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ. 본 증례의 경우 간농양 진단하 경피적 배농술과 개복 배 농술을 시행한 후 12개월간 항결핵 요법을 시행한 환자로 이후에도 피하 배농이 지속되어 방사선학적 검사상 결핵성 간농양, 간내담도-경피 누공, 간내담도-간정맥 누공으로 진 단되어 간 7분절 절제술을 시행하고 6개월간 2차 항결핵 요 법을 재시행하였으나, 다시 지속적인 우상복부 동통을 호 소하여 재발성 결핵성 간농양으로 진단되었다. 이전보다 농양의 크기가 더 커졌고, 약물 반응이 없는 것으로 판단되 어 수술적 치료를 위하여 간우엽 절제술을 시행한 환자를 경험하였기에 보고하는 바이다.. 참 고 문 헌 1) Kim DS, Yun SS, Chang JC, Kim HJ, Kwun KB. Biliarycutaneous fistula combined with biliary-hepatic venous connection, a case report. Korean HBP Surg 1999;3:113-6. 2) Hong SM, Kim DH, Lee WH, Kong HH, Woo JH. A clinical review of intraabdominal tuberculosis. Korean J Gastroenterol 1994;26:1021-8. 3) Sharma SK, Mohan A. Extrapulmonary tuberculosis. Indian J Med Res 2004;120:316-53. 4) Hassan I, Brilakis ES, Thompson RL, Que FG. Surgical management of abdominal tuberculosis. J Gastrointest Surg 2002; 6:862-7. 5) Chan HS, Pang J. Isolated giant tuberculomata of the liver detected by computed tomography. Gastrointest Radiol 1989;14: 305-7. 6) Seife M, Kessler BJ, Hoffman J, Lisa JR. A clinical, functional, and needle biopsy study of the liver in pulmonary tuberculosis. Am Rev Tuberc 1951;63:202-9. 7) Essop AR, Moosa MR, Segal I, Posen J. Primary tuberculosis of the liver, a case report. Tubercle 1983;64:291-3.. 8) Leader SA. Tuberculosis of the liver and gall-bladder with abscess formation. Ann Int Med 1952;37:594-606. 9) Denath FM. Abdominal tuberculosis in children. CT findings. Gastrointest Radiol 1990;15:303-6. 10) Babara BF. Edward CR. Hepatic granulomata. Arch Int Med 1965;115:223-34. 11) Park JH, Baek SH, Ko JK, Lee YK, Lee JY, An DS. A case of miliary tuberculosis of the liver. Korean J Gastroenterol 1980;12:93-7. 12) Alcantara-Payawal DE, Matsumura M, Shiratori Y, Okudaira T, Gonzalez R, Lopez RA, et al. Direct detection of mycobacterium tuberculosis using polymerase chain reaction assay among patients with hepatic granuloma. J Hepatology 1997;27: 620-7. 13) Diaz ML, Herrera T, Lopez-Vidal Y, Calva JJ, Hernandez R, Palacios GR, et al. Polymerase chain reaction for the detection of mycobacterium tuberculosis DNA in tissue and assessment of its utility in the diagnosis of hepatic granulomas. J Lab Clin Med 1996;127:359-63. 14) Essop AR, Posen JA, Hodkinson JH, Segal I. Tuberculosis hepatitis, a clinical review of 96 cases. Q J Med 1984;53:46577. 15) Terry RB, Gunnar RM. Primary miliary tuberculosis of the liver. JAMA 1957;164:150-7. 16) Choi JY, Kim KW, Shin DJ, Mok CS, Chang SI, Choi DS. A case of hepatic tuberculosis secondary to intestinal tuberculosis. Tuberculosis and respiratory disease 1998;35:262-9. 17) Henry LB. Tuberculosis of the liver. In: Gastroenterology. 3rd ed. Philadelphia: W.B. Saunders; 1976. p.511. 18) Ham HJ, Park EB. Tuberculous cyst of the liver, a case report. Korean J Gastroenterol 1984;16:329-33. 19) Kim YJ, Yu SY, Kim SY, Kim SW. Solitary tuberculoma of the liver, a case report. J Korean Surg Soc 1978;20:61-8..
(5)
수치

관련 문서
In the present case, neck abscess caused by Salmonella serotype D in a patient with liver cirrhosis and diabetic was successfully treated with antibiotics and surgical drainage.. A
In addition, the number of patients who have been admitted at Daejeon Jaseng Hospital of Korean Medicine for recurrent neck pain after receiving surgical and
We present a case where the accessory right hepatic artery of the liver was ligated leading to postoperative liver abscess formation in the liver graft.. A for-
Although this series did not confirm any beneficial effect of surgical procedures to recurrent masses in the liver, lung, pleura, or multiple sites on survival, sur- gical
In this study, we examined the outcomes of surgical resection for HCC patients meeting the Milan criteria with preserved liver function and rationale of hepatic resection as the
