780
Transradial Coronary Intervention: Comparison of the Left and Right Radial Artery Approach
Jang-Young Kim, MD, Junghan Yoon, MD, Il-Hyung Jung, MD, Hee-Sung Wang, MD,
Hyun-Sook Jung, MD, Byung-Su Yoo, MD, Seung-Hwan Lee, MD and Kyung-Hoon Choe, MD Department of Cardiology, Wonju College of Medicine, Yonsei University, Wonju, Korea
ABSTRACT
Background and Objectives:We evaluated the efficacy and safety of the left transradial approach as compared to the right radial approach when performing transradial coronary intervention. Subjects and Methods:We performed the transradial coronary intervention in 711 cases via the left approach (Lt. group) and in 614 cases via the right approach (Rt. group) for patients with a normal Allen’s test of both arms. We evaluated the pro- cedural success rate, the crossover rate, the puncture time, the total procedural duration, the fluoroscopy time, the amount of contrast agent used and the local vascular complications of both groups. Results:The baseline clinical and angiographic profiles were comparable between both groups. The puncture time, the amount of contrast agent used, choice of the guide catheter and local vascular complications were similar for the two groups. There was no difference in the procedural success rate (Rt. group; 96.4% vs. Lt. group; 96.2%, p=NS). However, there was ten- dency for a higher success rate via radial access for the Lt. group than for the Rt. group (Rt. group; 91.9% vs. Lt.
group; 93.5%, p=0.056). The crossover rate was lower for the Lt. group than for the Rt. group (2.7 % vs. 4.6%, respectively; p=0.04). The total procedural time (32.3±15.4. vs. 30.7±17.6 min, respectively; p=0.03) and fluo- roscopy time (16.9±12.6 vs. 13.9±7.9 min, respectively; p<0.01) were shorter in the Lt. group. The number of guide catheters used was higher in the Rt. group compared to the Lt. group (1.21±0.48 vs. 1.08±0.33, respectively;
p=0.04). Conclusion:The left radial approach may provide increased procedural efficacy for transradial PCI compared to the right radial approach along with similar complications. (Korean Circulation J 2006;36:780-785) KEY WORDS:Angioplasty;Coronary arteries;Radial artery.
Introduction
The radial approach for coronary interventions ap- pears to be a safe alternative to femoral access.1)2) Indeed, the radial approach nearly abolishes complications at the vascular entry sites and it permits a wide range of diagnostic and therapeutic interventions.1-6) Most pro- cedures are usually approached from the right side of the patients. In that sense, the right radial approach ap- pears to be more comfortable to operators. However, the right and left approaching artery systems are not exact mirror counterparts. The course of the guiding catheter can be affected by the braciocephalic artery in the right radial approach, in addition to the subclavian artery.7)
Further, vascular tortuosity is increased with increasing age.7)
Recent evidence suggested that there are some ana- tomical and technical differences(radial artery puncture, selection of the guiding catheter and the procedural re- sults etc) between the right and left radial approaches during transradial procedures.7-10)
At present, the choice of the right or left radial artery as an entry site depends largely on the operator’s prefe- rence. However, there is no comparative data between the right and left radial approach when performing percutaneous coronary intervention(PCI). Therefore, we evaluated the difference between the right and left radial approach for transradial coronary intervention.
Subjects and Methods Study population
Between January 1 2003 and December 31 2004, 1,450 cases of PCI were performed at our institution by three senior operators(greater than 200 PCI cases/year/ope-
Received:November 28, 2006 Accepted:December 27, 2006
Correspondence:Junghan Yoon, MD,Department of Cardiology, Wonju College of Medicine, Yonsei University, 162 Ilsan-dong, Wonju 220-701, Korea
Tel: 82-33-741-1212, Fax: 82-33-741-1219 E-mail: [email protected]
rator). The large majority of these procedures(1,325 cases, 91.4%) were transradial PCI with using the radial artery as a primary vascular route at our institute.
The right radial approach(Rt. group) was used for 614 cases and the left radial approach(Lt. group) was used for 711 cases. The exclusion criteria were the cli- nical indications for using the femoral approach due to cardogenic shock, a negative Allen test, chronic renal failure and no palpable radial artery. The choice between the left or right radial approach was left to the discre- tion of the operators.
Procedural preparation
A written informed consent was obtained before the PCI from the patient or the family member(s). In the case of elective PCI, baby aspirin(200 mg) and clopi- dogrel(75 mg) were given to all the cases for at least 3 days before the procedure. In case of primary or urgent PCI, all the patients received baby aspirin(300 mg) and a loading dose of clopidogrel(300 mg) just before the PCI. The inguinal area was also prepared for the cases that required crossover, IABP or temporary pacemaker support.
The patients were prepared with the left or right arm abducted and wrist hyperextended on the table next to the thigh. The arms were supported by a preformed fol- ded sheet and by sideward extension of the cathete- rization table(Fig. 1).
Transradial PCI
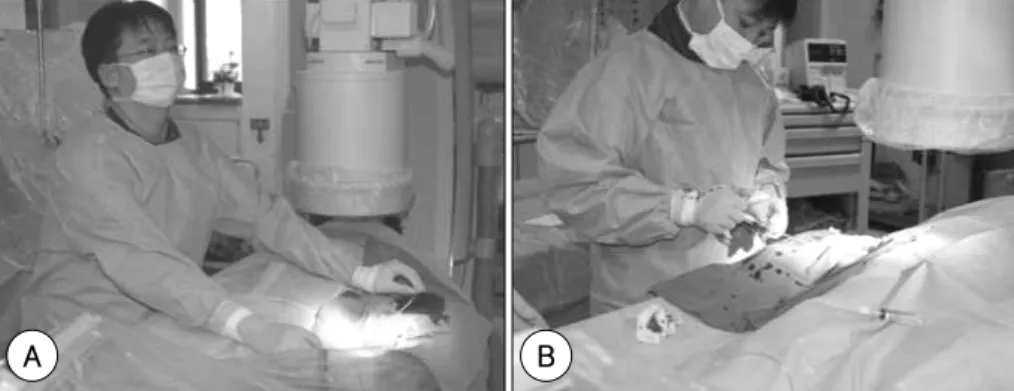
Transradial PCI was performed via the left or right radial artery with using the same methods described in a previous publication.4)5) The whole procedure, inclu- ding left radial arterial cannulation, was performed on the right side of the patients(Fig. 2). After local subcu- taneous infiltration with 2% lidocaine, the radial artery puncture was performed with a 20-gauge angiocatheter needle(Sindongbang Co., Seoul, Korea).
PCI was performed on an ad hoc basis after the dia- gnostic angiography in most cases(97%). A 6 Fr RADI- FOCUS sheath(Termo Co., Tokyo, Japan) or a 7 Fr MAXIMUM sheath(DAIG Corp, Minneapolis, MN) was placed depending on the target lesion, the device needed for the procedure and the size of the radial ar- tery, and an additional 5,000 U of heparin was given through the arterial sheath.
After the procedure, the arterial sheath was immedi- ately removed regardless of the ACT level. Compression was done using a TR bandTM(Terumo Co., Tokyo, Japan) or gauze compression was done with a Clo-Sur P.A.DTM (Scion Cardio-Vascular, Miami, FL) at the puncture site for about 3 hours or more.
Assessment of the procedural results and complica- tions
The procedural success rate, the major adverse cardiac events(MACE) and the vascular access site complications were assessed. Procedural success was defined as a resi- dual diameter stenosis of <30% with TIMI grade 3 flow.
The success rate via the radial access was defined as a successful procedure without crossover to the other ac- cess site. Bleeding at the access site was defined as major if it was associated with a hemoglobin loss of at least 2 mmol/L, administration of blood transfusions, vascular repair or prolonged hospitalization.11)
We estimated the procedure-related variables as fol- lows; the vascular access time(the time from lidocaine infiltration to insertion of the arterial sheath), the flu- oroscopy time and the total procedure time(the time from the first attempt at puncturing the artery to the end of angioplasty), the amount of contrast agent, the crossover rate(changing the vascular access to the opposite
Fig. 1. The pre-procedural position of the arm.
Fig. 2. Procedural position of the right and left radial approaches. A: left radial approach, B: right radial approach.
A B
radial artery or femoral artery), the mean number of guide catheters used and any access site vascular events (all the recordable events at the access site). All the an- giographic and clinical variables were recorded from the start of the procedure to the time of hospital discharge.
Data analysis
Statistical analysis was performed using the SPSS 12.0 statistical program(SPSS Inc., Chicago. IL, USA). Con- tinuous variables are expressed as means±SDs. Con- tinuous variables were compared using Student’s t-test, and the differences between the categorical variables were examined using the chi-square test. A probability level of <0.05 was considered statistically significant.
Results
Clinical and angiographic characteristics
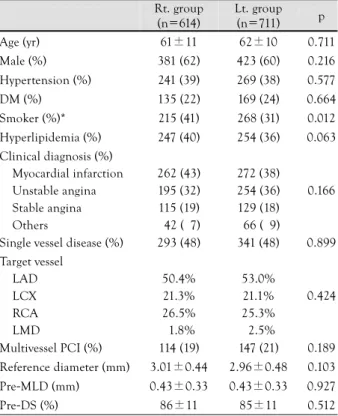
The baseline clinical and angiographic characteristics of the patients are shown in Table 1. The clinical para- meters such as mean age, gender, the clinical diagnosis and risk factors were similar in both groups. However, smokers were more prevalent for the right approach.
There were no differences in the reference vessel diame- ter, the minimal luminal diameter(MLD), the extent of coronary artery disease, the diameter of stenosis and the
PCI target vessel for both groups on the baseline angio- graphic findings.
Vascular access and cross-over rate
The cannulation failure rate was similar for both groups. There were 5 cases(0.9%) of puncture failure in the Rt. group and 6 cases(0.9%) in the Lt. group.
The PCIs were successfully completed after switching to the femoral artery in these cases. The vascular access time was not significantly different between both groups (Rt. group: 2.3±2.9 vs. Lt. group: 2.4±3.5 min, p=NS) (Table 2).
The cross-over rate to the femoral or contralateral ra- dial artery was lower for the Lt. group than for the Rt.
group(2.7% vs. 4.6%, respectively, p=0.04). The reasons for crossover in the Rt. group were severe subclavian artery tortuosity in 3 cases(0.5%), the alpha loop of the radial artery in 7 cases(1.1%), puncture failure in 5 cases(0.9%) and poor guiding support in 12 cases (2.0%). Crossovers were needed In the Lt. group due to severe subclavian artery tortuosity in 1 case(0.1%), the alpha loop of the radial artery in 3 cases(0.5%), puncture failure in 6 cases(0.9%), a small vessel with spasm in 4 cases(0.6%), and poor guiding support in 5 cases(0.9%)(Table 2).
Selection of the guide catheter
There was no difference in selecting the guiding ca- theter size for both groups. The most frequently used
Table 1. Clinical and angiographic characteristics of the right and left radial approaches
Rt. group (n=614)
Lt. group (n=711) p
Age (yr) 61±11 62±10 0.711
Male (%) 381 (62) 423 (60) 0.216
Hypertension (%) 241 (39) 269 (38) 0.577
DM (%) 135 (22) 169 (24) 0.664
Smoker (%)* 215 (41) 268 (31) 0.012
Hyperlipidemia (%) 247 (40) 254 (36) 0.063 Clinical diagnosis (%)
Myocardial infarction Unstable angina Stable angina Others
262 (43) 195 (32) 115 (19) 042 (07)
272 (38) 254 (36) 129 (18) 066 (09)
0.166
Single vessel disease (%) 293 (48) 341 (48) 0.899 Target vessel
LAD LCX RCA LMD
50.4%
21.3%
26.5%
01.8%
53.0%
21.1%
25.3%
02.5%
0.424
Multivessel PCI (%) 114 (19) 147 (21) 0.189 Reference diameter (mm) 3.01±0.44 2.96±0.48 0.103
Pre-MLD (mm) 0.43±0.33 0.43±0.33 0.927
Pre-DS (%) 86±11 85±11 0.512
*: p<0.05. DM: diabetes mellitus, LAD: left anterior descending, LCX: left circumflex, RCA: right coronary artery, LMD: left main disease, PCI: percutaneous coronary intervention, MLD: minimal luminal diameter, DS: diameter stenosis
Table 2. Procedural characteristics and results of the right and left radial approaches
Rt. group (n=614)
Lt. group (n=711) p Vascular access time (min) 2.3±2.9 2.4±3.5 0.873 Crossover (%)*
Puncture failure Small vessel with spasm*
Vessel tortuosity or loop Poor guide support*
28 (4.6) 05 00 10 12
19 (2.7) 6 4 4 5
0.041 0.913 0.025 0.062 0.047 No of guide catheter (%)
One catheter More than 2 catheters
523 (93) 091 (07)
632 (95) 079 (05)
0.772
No of guide catheter* 1.21±0.48 1.08±0.33 0.042 The size of guide catheter (%)
5/6/7/8 french 5/81/13/1 7/77/14/1 0.388
Fluoroscopy time (min)† 16.9±12.6 13.9±7.91 0.002 Total procedure time (min)* 32.3±15.4 30.7±17.6. 0.034 Contrast volume (mL) .208±76.0 .203±73.1 0.300 Stent implantation (%) 559 (91) 654 (92) 0.786 Post-MLD 2.84±0.43 2.78±0.47 0.094
Post-DS (%) 7±4 8±4 0.574
Procedural success (%) 592 (96.4) 684 (96.2) 0.892 Success via radial A. (%) 564 (91.9) 665 (93.5) 0.056
*: p<0.05, †: p<0.01. MLD: minimal luminal diameter, DS: dia- meter stenosis, A: artery
size of the guiding catheter was the 6 Fr guide catheter;
81% in the Rt. Group and 77% in the Lt. group(p=NS), respectively(Table 2).
For selecting the shape of the guiding catheter depen- ding on the right or left radial approach, there was no difference in the shapes of the guiding catheters for both approach methods(Fig. 3). Conventional Judkins catheters were frequently used in both groups. However, the mean number of guide catheters used was signifi- cantly lower for the Lt. group(1.08±0.33) as compared to the Rt. group(1.21±0.48)(p=0.03).
Procedural results
The post procedural MLD and diameter stenosis were similar in both groups. The total procedural time(Rt.
group; 32.3±15.4 min vs. Lt. group; 30.7±17.6 min, p=0.03) and fluoroscopy time(Rt. group; 16.9±12.6 min vs. Lt. group; 13.9±7.9 min, p<0.01) were shorter in the Lt. group. The amount of contrast material used was similar between the two groups(Rt. group; 208±
76 mL vs. Lt. group; 202±72 mL, p=0.30)(Table 2).
There was no statistical difference for the procedural success rate(Rt. group; 96.4% vs. Lt. group; 96.2%, p=
NS). However, there was a tendency for a higher success rate via the radial access for the Lt. group than for the Rt. group(Rt. group; 91.9% vs. Lt. group; 93.5%, p=
0.056)(Table 2).
There was no significant difference in the frequency of stent implantation between both groups (Rt. group:
91% vs. Lt. group: 92%, p=NS).
Procedure-related complications:
There was no difference for the hospital MACEs(Rt.
group; 2.1% vs. Lt. group; 2.5%, p=NS)(Table 3). 13 cases of the Rt. group experienced MACEs: cardiac death in 2 cases, atherothrombus embolism in 2 cases, coronary artery perforation in 1 case with CTO lesion, stent mig- ration in 1 case, cardiogenic shock in 1 case and 6 cases of slow flow and periprocdural myocardial infarction with increasing CK-MB. 18 cases in the Lt. group expe- rienced MACEs: cardiac death in 2 cases, atherothrom- bus embolism in 1 case, air embolism in 1 case, coro- nary artery perforation in 1 case, stent migration in 1 case, cardiogenic shock in 2 cases, aortocoronary dissec- tion in 1 case and 8 cases of slow flow and periproc- dural myocardial infarction with increasing CK-MB.
There was no difference for major vascular compli- cations between both groups(Rt. group; 0.3% vs. Lt.
group; 0%, p=NS). Vascular complication occurred in 2 cases in the Rt. group due to radial artery perforation that required transfusion. There was no case of hand ischemia or infarction(Table 3).
Discussion
We examined the efficacy of the left radial approach for transradial PCI as compared to the right approach.
The major finding in this study is that the left radial approach shows a higher trend of the procedural success rate than did the right approach, along with a lower rate of vascular access failure and a lower crossover rate to the other vascular access.
For selecting the vascular access site, most interven- tional cardiologists are familiar with doing the procedure at the right side of the patient because this approach is more convenient for manipulating the devices, inclu- ding the guide catheter. Therefore, most interventional cardiologists select the right radial artery as a first access route when performing transradial PCI. However, even
Table 3. Clinical outcome of the right and left radial approaches Rt. group
(n=614)
Lt. group (n=711)
p
In-hospital MACE (%) Cardiac death MI due to slow flow Atherothrombus embolism Cardiogenic shock Coronary artery perforation Stent migration
Air embolism
Aortocoronary dissection
13 (2.1) 2 6 2 1 1 1 0 0
18 (2.5) 2 8 1 2 1 1 1 1
0.834
Major vascular Cx (%) 02 (0.3) 00 (0) 0.911 MACE: major adverse cardiac event, MI: myocardial infarction, Cx:
complication
Judkins AL KIMNY XB Others
100%
080%
060%
040%
020%
000%
80%77%
5% 6% 3% 4% 9% 8% 3%5%
Right Left
A
Judkins AR KIMNY AL Others
100%
080%
060%
040%
020%
000%
74%72%
3% 5% 3% 7%
17%12%
3%4%
Right Left
B
Fig. 3. The shape of the guide catheter between the right and left ra- dial approach. A: guide shape of LCA, p=0.551 between both group.
B: guide shape of RCA, p=0.370 between both group. AL: Amplatz left, AR: Amplatz right, LCA: left coronary artery, RCA: right coronary artery, Others: RAD, hybrid, multipurpose and hockystick catheter.
for the left radial approach, the procedure can be per- formed at the right side of the patient with the left arm closely abutted to the patient’s trunk, just like the procedure in the right or femoral approach. The only difference in performing the left radial access is that because the operator’s standing position is apart from the left arm, the operator must bend over the patient, which might be inconvenient to the operator. However, the access time and success rate of vascular access were nearly same between the left and right approaches.
There are several advantages in selecting the left radial approach in terms of patient comfort and the effecti- veness of the procedures. The right approach might be more convenient for the operator; however, in our study, the left approach did not cause any inconvenience to the operator and it has several advantages. First, the left radial approach potentially increases patient comfort because most patients and especially Asains are right han- ded. The patients are free to use his/her right hand immediately after the procedure. Second, a left internal mammary angiogram can easily be performed in the case of a CABG candidate.
The access failure rate was similar in both groups. In the early period of transradial PCI, most of the failures were due to puncture failure. In fact, accessing the ra- dial artery requires a learning period to be competent.12-14) Achieving access to the radial artery is technically more challenging and time-consuming than is the femoral access, but when the right skills are grasped, then the technique is much easier and reliable. In our study, there was less than 1% puncture failure and no difference for the vascular access time between both groups. Therefore, radial arterial access might not be a limiting step to achieve procedural success.
In selecting the guide catheter, the size and shape of the guiding catheter that was used were similar for both groups in this study. However, the mean number of guide catheters was lower for the left group. In our previously reported data,9) the major reasons of failure for trans- radial PCIs were inadequate guide support or guiding failure due to radial artery tortuosity and subclavian or inominate artery tortuosity. A tortuous conduit vessel may cause discomfort that’s associated with prolonged manipulation of catheters, access failure, arterial dissec- tion and arterial perforation. So, severe tortuosity of the conduit vessel was a limiting factor for transradial PCI. In the study of Wu et al. and Kawashima et al., mar- ked subclavian tortuosity was prevalent in the patients who underwent the right radial approach.8)15)16) For our data, the crossover rate was lowered for the left group than for the right group(2.7% vs. 4.6%, respectively, p=0.04), and crossover to the femoral or contralateral radial artery was due to conduit vessel tortuosity and poor guide support. There was a trend for a higher success rate via the radial approach in the left approach com-
pared to the right approach(p=0.056)(Table 2). There- fore, our data demonstrates that access failure during transradial PCI is lower for the left approach than the right approach due to the higher incidence of conduit vessel tortuosity in the right approach.
The other results of our study are consistent with the previous studies of transradial PCI that have compareed the clinical characteristics, angiographic characteristics, procedural results and MACEs.1-4) The vascular com- plication rate was nearly zero(two cases) in our study group. We routinely used a TR bandTM(Terumo Co., Tokyo, Japan) or gauze compression with a Clo-Sur P.A.DTM(Scion Cardio-Vascular, Miami, FL) as the com- pression method at the puncture site.17)
Although this study enrolled a relative large sample size(about 1,400 cases) of transradial PCI, a limitation of this study is that it is retrospective observation study and it lacked randomization between the right and left radial accesses. The present study demonstrated that the left radial approach may provide high procedural efficacy for performing transradial PCI compared to the right radial approach.
REFERENCES
1) Agostoni P, Biondi-Zoccai GG, de Benedictis ML, et al. Radial versus femoral approach for percutaneous coronary diagnostic and interventional procedures: systematic overview and meta- analysis of randomized trials. J Am Coll Cardiol 2004;44:349-56.
2) Archbold RA, Robinson NM, Schilling RJ. Radial artery access for coronary angiography and percutaneous coronary interven- tion. BMJ 2004;329:443-6.
3) Yoon J, Lee SH, Lee HH, et al. Usefulness of trans-radial coro- nary angiography in Wonju. Korean Circ J 1998;28:1670-6.
4) Kim JY, Lee SH, Choe HM, Yoo BS, Yoon J, Choe KH. The feasibility of percutaneous transradial coronary intervention for chronic total occlusion. Yonsei Med J 2006;47:680-7.
5) Kim JY, Yoon J, Jung HS, et al. Feasibility of the radial artery as a vascular access route in performing primary percutaneous coronary intervention. Yonsei Med J 2005;46:503-10.
6) Lee KJ, Lee SH, Hong KP, Park JE, Seo JD, Gwon HC. Feasibility and safety of the transradial approach for the intracoronary spasm provocation test. Catheter Cardiovascular Interv 2005;65:240-6.
7) Cha KS, Kim MH, Kim HJ. Prevalence and clinical predictors of severe tortuosity of right subclavian artery in patients under- going transradial coronary angiography. Am J Cardiol 2003;
92:1220-2.
8) Kawashima O, Endoh N, Terashima M, et al. Effectiveness of right or left radial approach for coronary angiography. Catheter Cardiovasc Interv 2004;61:333-7.
9) Yoo BS, Lee HH, Yoon J, et al. The study of branching ano- maly and tortuosity of radial artery for trans-radial coronary procedure. Korean Circ J 2000;30:82-9.
10) Yoo BS, Yoon J, Ko JY, et al. Anatomical consideration of the radial artery for transradial coronary procedures: arterial dia- meter, branching anomaly and vessel tortuosity. Int J Cardiol 2005;101:421-7.
11) Choussat R, Black A, Bossi I, Fajadet J, Marco J. Vascular com- plications and clinical outcome after coronary angioplasty with platelet IIb/IIIa receptor blockade: comparison of transradial vs transfemoral arterial access. Eur Heart J 2000;21:662-7.
12) Goldberg SL, Renslo R, Sinow R, French WJ. Learning curve in the use of the radial artery as vascular access in the performance of percutaneous transluminal coronary angioplasty. Cathet Car- diovasc Diagn 1998;44:147-52.
13) Cheng TO. Influence of learning curve on the success of trans- radial coronary angioplasty. Cathet Cardiovasc Diagn 1998;45:
215-6.
14) Salgado Fernandez J, Calvino Santos R, Vazquez Rodriguez JM, et al. Transradial approach to coronary angiography and angio- plasty: initial experience and learning curve. Rev Esp Cardiol 2003;56:152-9.
15) Wu CJ, Lo PH, Chang KC, Fu M, Lau KW, Hung JS. Transradial coronary angiography and angioplasty in Chinese patients.
Cathet Cardiovasc Diagn 1997;40:159-63.
16) Abhaichand RK, Louvard Y, Gobeil JF, Loubeyre C, Lefevre T, Morice MC. The problem of arteria lusoria in right transradial coronary angiography and angioplasty. Catheter Cardiovasc Interv 2001;54:196-201.
17) Choi EY, Ko YG, Kim JB, et al. Hemostatic efficacy of hydro- philic wound dressing after transradial catheterization. J Invasive Cardiol 2005;17:459-62.