84
Balloon-Based Distal Protection Device Improves the Recovery of Left Ventricular Function after Primary Coronary Angioplasty
Il Rhee, MD, Sung-Uk Kwon, MD, Hyeon-Cheol Gwon, MD, Jinho Choi, MD, Sang Hoon Lee, MD, Kyung Pyo Hong, MD and Jung Euy Park, MD
Department of Medicine, Sungkyunkwan University School of Medicine, Cardiac and Vascular Center, Samsung Medical Center, Seoul, Korea
ABSTRACT
Background and Objectives:Despite the high success rate of primary angioplasty in cases of acute myocardial infarction (AMI), myocardial reperfusion can frequently be compromised, mainly due to distal embolization, which can be effectively prevented with the use of distal protection devices. The goal of this study was to see whether PercuSurge®, a balloon-based distal protection device, could improve myocardial reperfusion and late clinical out- comes after primary coronary angioplasty. Subjects and Methods:Between April 2002 and July 2003, 29 patients with AMI, within 12 hours of the onset of symptoms, were scheduled to undergo primary angioplasty using PercuSurge® (PS group). Thirty patients were selected as a control group by matching the 5 clinical and angio- graphic variables; the clinical status and coronary angiograms were also prospectively reviewed and analyzed. Results:
There were no significant differences in the baseline clinical and angiographic characteristics, including the left ventricular ejection fraction (LVEF) between two groups. The procedures were successful, without complications, in all patients from both groups. However, the PS group was associated with a significantly higher incidence of myocardial blush score of 3 (PS 58%, control 30%, p=0.001) and early ST-segment elevation resolution (PS 76%, control 47%, p=0.02) compared to the control group. The PS group also showed a greater LVEF at 60 days after the procedure (PS 51±5%, control 46±8%, p=0.007). There was no significant difference in the incidences of death or myocardial infarction between the two groups during the follow-up period. Conclusion:The use of the PercuSurge® was found to be safe and feasible during primary angioplasty, and this system also improved the recovery of the left ventricular function as well as myocardial reperfusion following primary coronary angioplasty.
(Korean Circulation J 2006;36:84-90)
KEY WORDS:Angioplasty;Transluminal;Percutaneous coronary;Myocardial infarction;Thromboembo- lism;Balloon occlusion.
Introduction
A successful result with Thrombolysis in Myocardial Infarction(TIMI) grade 3 flow can be achieved in about 90% of cases of primary percutaneous coronary inter- vention(PCI) in acute myocardial infarction(AMI).
However, when assessed using the angiographic myocar- dial blush scores and early resolution of ST-segment elevation(STe), the myocardial tissue or microvascular
reperfusion has been shown to be impaired in two thirds of patients with TIMI 3 flow.1-6) Impaired myocardial tissue reperfusion has been shown to be associated with unfavorable left ventricular(LV) functional recovery and a poor clinical prognosis.7)
Distal embolization of a thrombus or plaque material during primary PCI is thought to be the major mecha- nism for impaired microvascular reperfusion.8-10) The- refore, the mechanical prevention of distal embolization would be expected to improve myocardial reperfusion and recovery of the LV function. There are many kinds of distal protection device, including various types of balloon-based devices and distal filter-based devices.
The PercuSurge® Guard-Wire system is a balloon- based distal protection systems, which has been proved to be beneficial during angioplasty of saphenous vein graft lesions.11) Herein, we tested the hypothesis that
Received:November 8, 2005 Accepted:December 26, 2005
Correspondence:Hyeon-Cheol Gwon, MD, PhD,Department of Medicine, Sungkyunkwan University School of Medicine, Cardiac and Vascular Cen- ter, Samsung Medical Center, 50 Ilwon-dong, Gangnam-gu, Seoul 135- 230, Korea
Tel: 82-2-3410-3995, Fax: 82-2-3410-0483 E-mail: [email protected]
the PercuSurge® Guard-Wire system may help the LV functional recovery by improving the myocardial tissue reperfusion during primary angioplasty in AMI pati- ents.
Subjects and Methods Patients population
This study was designed as a single center prospective non-randomized comparative study. The patients who presented with acute anterior chest pain of more than 30 minutes duration and ST-segment elevation >0.1 mV in at least 2 contiguous leads on the 12-lead electrocar- diograms(ECGs), and who had undergone primary PCI within 12 hours of the onset of symptoms were inclu- ded. The infarct-related lesion had to be in the mid or proximal segment of the major artery and the reference diameter more than 2.5 mm to accommodate the Guard- Wire balloon. The exclusion criteria were: unprotected left main coronary disease >50%, or after thromboly- tic therapy, cardiogenic shock, a known allergy to aspirin, clopidogrel, or heparin, current neutropenia, thrombo- cytopenia or a history of serum creatinine >2.5 mg/dl.
Primary PCI was performed with distal protection using the PercuSurge® Guard-Wire system in PercuSurge® group(PS group). The matched control group was se- lected from patients who had undergone primary PCI without a distal protection device. The following para- meters were matched; 1) the location of infarct-related artery(IRA), 2) pre-PCI TIMI flow grade, 3) gender, 4) age and 5) pain-to-balloon time.
Data collection
We reviewed the medical records of the patients to identify their clinical characteristics. The 12-lead ECGs were analyzed both before and at the end of the proce- dure by a blinded observer. The total STe was measured manually from the leads exploring the infarct area, as previously described.12) The early resolution of the STe after PCI was defined as >50% reduction in the initial value on the ECG 90 minutes after the procedure. Echo- cardiography was performed both before and 60 days after PCI, with the echocardiograms analyzed by 2 obser- vers blinded to the clinical and angiographic data. Left ventricular wall motion score index(WMSI) and left ventricular ejection fraction(LVEF) were calculated using Simpson’s methods. The creatine kinase MB fraction (CK-MB) was measured every 8 hours during the first day, and then daily thereafter until discharge.
Primary PCI with PercuSurge
®The PercuSurge® Guard-Wire system is a balloon-based distal protection system, composed of three separate ele- ments: the Guard-Wire®, the Micro-seal® inflation adap- tor and the Export® aspiration catheter(EAC). The
Guard-Wire® is a temporary occlusive device, consisting of a hollow 0.014 inch nitinol hypo-tube, with a distal, low profile, elastomeric occlusion balloon. The EAC is a 135cm long 4.6 Fr catheter, with a dual lumen, which allows the aspiration and removal of particulate debris.
All patients received 100 IU/kg of unfractionated he- parin, 300 mg of chewable aspirin and 300 mg of clo- pidogrel. Intra-aortic counter-pulsation was performed in the case of hemodynamic instability. The activated clotting time was maintained at more than 300 seconds during the procedure. After the diagnostic coronary an- giography, an 8 Fr guiding catheter was to engage into the infarct-related artery. An initial attempt to cross the culprit lesion was performed with the Guard-Wire, but when this was not possible, the operator used a con- ventional wire to help the Guard-Wire to cross the lesion.
When required, predilatation with a small-diameter bal- loon was performed before placement of the Guard- Wire. Once in place, the Guard-Wire was about 1-2 cm distal of the target lesion, with the position checked using fluoroscopy. The balloon was then inflated and proper placement of the Guard-Wire confirmed by the lack of distal antegrade flow. The inflation of the distal occluding balloon was maintained while the EAC was connected to a 20 ml suction syringe for manual aspi- ration, followed by initial balloon predilatation and the subsequent aspiration of debris. Following aspiration, the aspirate was rinsed over a 40 mm nylon cell strainer, with the protective distal balloon then inflated again;
stenting was performed only in the IRA in all patients, followed by further aspiration at the conclusion of the stenting procedure. Finally, the balloon was deflated in order to visualize the angiographic results. If additional intervention was required, this was always performed under distal protection.
Glycoprotein IIb/IIIa inhibitors were given at the operator’s discretion. Aspirin, 100 mg per day, was gi- ven after the PCI, as was clopidogrel, 75 mg, once a day.
The When the post-procedural diameter stenosis of the infarct artery was <20%, with adequate restoration of coronary patency(TIMI flow grade 3), the PCI was con- sidered successful.
Angiographic analysis
The angiograms were analyzed separately by 2 expe- rienced observers blinded to both the patient groups and clinical data. The basal TIMI flow was evaluated on the first angiogram, with the post-procedure TIMI flow and myocardial blush score graded on those taken immedi- ately after PCI. In each patient, the best projection was chosen to assess the myocardial region of the infarct- related coronary artery. Quantitative coronary angiogra- phy parameters, TIMI flow grade, corrected TIMI frame count(cTFC) and myocardial blush were measured, as previously described.4)13-15) With regard to the cTFC, the
number of frames was multiplied by 30, and then divi- ded by 12.5, to report a cine frame count in accordance with the standard methods. Myocardial blush was graded according to the dye density score proposed by van’t Hof et al; grade 0 to 1 was minimal to no myocardial blush or contrast density, grade 2 was moderate blush, and grade 3 was normal blush in comparison to the dye den- sity in the uninvolved area.4) In the case of any disagree- ment, a third observer evaluated the angiographic images, with consensus obtained by discussion. Intra-observer agreement was measured by having an observer repeat the assessment on 20 angiographic images(presented in random order) after one week. The inter-observer agree- ment was measured by comparing the assessment of the 20 angiographic images by two observers. The kappa values for intra-observer agreement of the TIMI flow grade, cTFC and myocardial blush score were 1.00, 0.90 and 0.78, respectively. In addition, the kappa values for inter-observer agreement of those items were 1.00, 0.89, and 0.74, respectively.
Study End-points
The primary end point was the change in the LVEF at 60 days compared to that prior to discharge. The se- condary end-points were the feasibility and safety of the adjunctive use of the PercuSurge® during primary PCI, 90 minutes resolution of the STe, the myocardial blush score and cTFC.
Statistical analysis
Data are expressed as the mean±standard deviation for continuous variables, and as the absolute and rela- tive frequencies for categorical variables. An unpaired Student’s t test was used to compare the continuous variables between groups, with a paired Student’s t test used to assess changes between the baseline and the follow-up data obtained at 60 days. Categorical variables were compared using the Chi-squared test. Predictors of the occurrence of STe resolution and of a myocardial blush score of 3 were identified by a univariate analysis.
Probability values <0.05 were considered statistically significant.
Results
Matched comparison of baseline characteristics and procedural results
The PS and control groups included 29 and 30 pati- ents, respectively. The baseline clinical and angiographic characteristics of the 2 groups are shown in Table 1.
There were no significant differences between the two groups with regard to age, gender, peak CK-MB, culprit location, incidence of coronary risk factors, TIMI flow grade before reperfusion and pain to balloon time, as well as the mean baseline LVEF and WMSI values on admis-
sion. Intravenous Abciximab was used more frequently in the control group, although this did not reach sta- tistical significance(p=NS). The procedural characte- ristics are presented in Table 2. There were no significant differences between the two groups in terms of the dia- meter of stenosis, reference vessel diameter, minimal luminal diameter and TIMI flow 3 after PCI. There were 3 cases of incomplete procedure in the control group, resulting in residual stenosis and low-grade TIMI flow, but these were resolved by successful PCI after a few days.
After PCI; however, the frequency of a myocardial blush score of 3, as well as the STe resolution were significan-
Table 1. Clinical and angiographic characteristics on admission of the patients in the PercuSurge® (PS) and control groups
PS (n=29) Control (n=30) p
Age (years) 58±11 59±14. NS
Sex, male/female (n) 23/6 22/8 NS
Hypertension (%) 17 (59). 18 (60) NS
Hypercholesterolemia (%) 5 (17) 04 (13) NS
Diabetes, n (%) 7 (24) 08 (27) NS
Smoking history, n (%) 6 (21) 08 (27) NS
LVEF (%) 46±9.0 43±90 NS
LV WSMI 1.5±0.3 1.6±0.4 NS
IRA, n (%)
LAD 13 (45) 11 (37) NS
RCA 15 (60) 18 (52) NS
LCX 01 (04) 01 (03) NS
TIMI flow grade, 0-1/2/3 19/4/6 20/4/6 NS Pain-to-balloon time (min) 267±57.0 263±360. NS Use of abciximab, n (%) .3 (10) 10 (33) NS LVEF: left ventricular ejection fraction, WMSI: wall motion score in- dex, IRA: infarct-related artery, LAD: left anterior descending artery, RCA: right coronary artery, LCX: left circumflex artery, TIMI: throm- bolysis in myocardial infarction, NS: not significant
Table 2. Procedural results in the 2 study groups PS (n=29)
Control (n=30) p Procedural success, n (%) 29 (100) 27 (90) NS Reference diameter (mm) 03.4±0.5 3.3±0.5 NS Minimal luminal diameter (mm) 1.85±0.4 1.42±0.63 NS
Diameter stenosis (%) .0.9±10 8±9 NS
Stent length (mm) 19±9. .17±70 NS
TIMI flow grade <3, n (%) 03 (010) 04 (13) NS cTFC, frames 23.5±2.4 25.1±2.90. 0.054 Myocardial blush score, n (%)
0-1 02 (007) 09 (30)
2 10 (035) 12 (40)
3 17 (058) 09 (30)
0.001
STe resolution >50% at 90 min, n (%)
22 (076) 14 (47) 0.020
Peak CK-MB (U/L) 202±45 242±540- 0.010 PCI: percutaneous coronary intervention, cTFC: corrected TIMI frame count, MB: myocardial blush grade, PS: PercuSurge®, TIMI: throm- bolysis in myocardial infarction
tly greater in the PS group(myocardial blush score of 3:
PS 58%, control 30%, p=0.001, STe resolution >50%:
PS 76%, control 47%, p=0.02). There was a tendency for a higher cTFC in the control compared to the PS group(PS 23.5±2.4, control 25.1±2.9, p=0.054). The peak CK-MB value was also significantly higher in the control compared to the PS group(PS 202±45 U/L, control 242±54 U/L, p=0.01). A univariate analysis indicated that use of the PercuSurge® was the only pre- dictor of STe resolution(p=0.02) and a myocardial blush score of 3 after PCI(p=0.002)(Table 3).
Feasibility and safety of the use PercuSurge
®during primary PCI
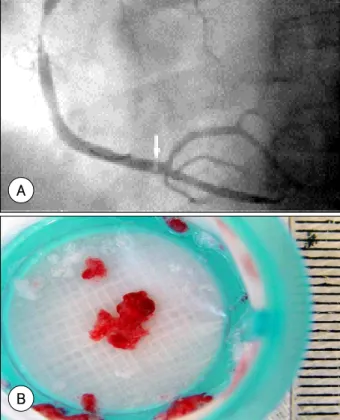
The PercuSurge® Guard-Wire system was successfully used in all the patients of the PS group, with no case of major in-hospital complications attributable to the PercuSurge® system. In 26 of the 29 PS cases(92%), aspiration with the EAC® yielded grossly visible particles and thrombotic material, which were reddish or white in color, and sometimes admixed with partially organized clots(Fig. 1).
Left ventricular function and clinical course
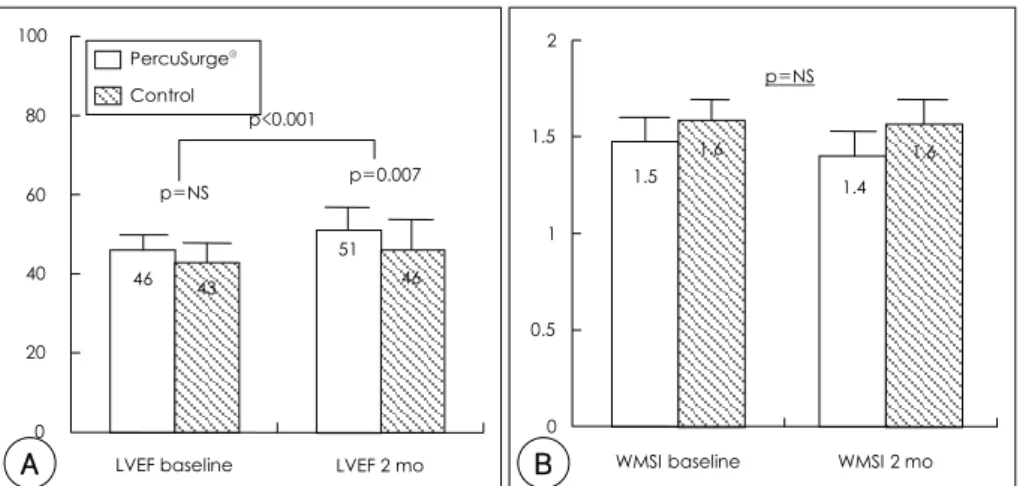
The LVEF at day 60 was significantly higher in the PS than in the control group(Fig. 2A, PS group 51±5%, C group 46±8%, p=0.007), whereas the baseline LVEF was not statistically different between the 2 groups(PSgroup 46±9%, C group 43±9%, p=NS). The LVEF had improved significantly at 60 days in both groups (PS group p<0.001, C group p<0.001), but there was a tendency for a larger improvement in the PS group (PS group 5.2±5.1%, C group 3.3±3.2%, p=0.089).
The WMSI was not significantly improved in either group(Fig. 2B, PS group: 1.5±0.3 to 1.4±0.3, p=NS, C group: 1.6±0.4 to 1.6±0.4, p=NS).
One patient in the control group died in hospital due to the development of refractory cardiogenic shock and mitral regurgitation. There were no significant differen- ces in the incidence of death, myocardial infarction or revascularization at 30-day between the 2 groups(PS group 5%, C group 11%, p=0.49).
Discussion
This study demonstrates that a balloon-based distal protection device, the PurcuSurge® Guard-Wire system, can be effectively used during primary PCI, with a high rate of success and without significant complications, which was followed by improved myocardial reperfusion and LV functional recovery.
Distal embolization to the coronary circulation, as well as impaired microvascular reperfusion, are serious com- plications during primary PCI in AMI patients.8)10)16-18) Angiographic evidence of distal embolization during pri-
Table 3. Variables associated with STe resolution and a myocardial blush score of 3 in a univariate analysis
No Yes p
STe resolution 90 min after
reperfusion n=17 n=28
Age (years) 062±13.. 057±12. NS
DM, n (%) 02 (12) 08 (29) NS
LAD, n (%) 10 (59) 18 (64) NS
Multivessel involvement 07 (41) 13 (46) NS Use of abciximab, n (%) 04 (24) 05 (18) NS Pain-to-balloon time (min) 254±42. 271±50 NS
LVEF (%) 42±9. 45±8. NS
WMSI 01.6±0.5 01.5±0.3 NS
Use of PS, n (%) 5 (29) 18 (64) 0.02
Grade 3 blush n=20 n=25
Age 061±13. 060±12. NS
DM, n (%) 03 (15) 07 (28) NS
LAD, n (%) 11 (55) 17 (68) NS
Multivessel involvement 08 (40) 12 (48) NS Pain-to-balloon time (min) 252±40. 275±51 NS
LVEF (%) 43±9. 45±8 NS
WMSI .1.6±0.5 01.5±0.3 NS
Use of PS, n (%) 05 (25) 18 (72) 0.002 STe: ST segment elevation, DM: diabetes mellitus, LAD: left anterior descending artery, LVEF: left ventricular ejection fraction, WMSI: wall motion score index, PS: PercuSurge®
Fig. 1. A: angiographic view of the PS deployed during PCI of an acu- tely occluded RCA artery. A filling defect (arrow) is visible. B: same case, magnified view of obtained reddish thrombi. RCA: right coronary artery, PCI: percutaneous coronary intervention, PS: PercuSurge®.
A
B
mary PCI has been reported to range between 9 and 15%,10)19) with signs of microvascular hypoperfusion after successful PCI also observed due to microemboli, which are considered an important contributor to the no-re- flow phenomenon according to the markers used to assess effective reperfusion, such as angiographic MB and resolution of STe.1-6)20)
Distal embolization and/or the no-reflow phenome- non during primary PCI have an adverse effect on the prognosis. The 5-year mortality rate can be as high as 44% in patients with distal embolization, whereas this is only 9% in those without.10) Thus, the mechanical prevention of distal embolization during primary PCI might prevent myocardial reperfusion and improve cli- nical outcomes.21-23)
Glycoprotein IIb/IIIa inhibitors have been reported to be effective in preventing distal microembolization and improving myocardial perfusion during PCI.24-26) However, the clinical outcomes in large randomized trials were not shown to be improved. The CADILLAC trial showed that Abciximab was not effective at reducing the 30-day major adverse cardiac events in the primary sten- ting of AMI.
The PercuSurge® has recently been shown in the SAFER study to improve the clinical outcomes in pati- ents undergoing saphenous vein graft intervention. The beneficial effect of distal protection was noted to be independent of the use of GP IIb/IIIa inhibitors.11)17) However, not much data exists on the efficacy of distal protection in native coronary arteries during primary PCI in AMI.
The use of PercuSurge® has been discouraged due to the technical limitations of the available device; 1) The design of the Guard-Wire®, which is less trackable and maneuverable than routine 0.014” guide-wires, 2) Its incomplete protection of proximal side branches from atheroembolization and its limited utility for preexisting distal embolization, 3) Cessation of distal flow, with ischemia, during intervention, 4) A mismatch of the bal-
loon and vessel diameters due to difficulty in estimating the actual distal vessel size, and 5) excessive time required for its use. Our series; however, showed that use of the PercuSurge® was feasible and safe, with a high rate of success, even during emergent angioplasty in AMI.
Some small studies have reported favorable immediate angiographic results using the PercuSurge® as an adjunct to primary PCI, and without procedural complications;
conversely, the EF in the acute phase did not change, although the EF in the chronic phase was significantly higher in the PS compared with the control group.
However, this prospective study has demonstrated that, after the use of the PercuSurge® in native coronary arte- ries during primary PCI, the integrated analysis of the cTFC, MB and STe changes in a single patient allows for better characterization of the microvascular reperfusion of the infarct area, and also predicts a 2-month LV func- tional recovery in patients with AMI. In this study, the LVEF was significantly improved at 60 days with respect to the baseline values, with this increase being greater in the PS group.
We evaluated simple tools that significantly correlate with the tissue-level perfusion shortly after recanalization of the IRA, early recovery of the LV function and sur- vival. The MB score and STe resolution have been vali- dated as markers of effective myocardial reperfusion and as predictors of the clinical outcome.3)4)12) A cTFC cutoff value of 23 has also been demonstrated as being highly predictive of a greater LV functional recovery and favo- rable clinical outcomes, including a lower incidence of in-hospital complications compared to those patients with a higher cTFC27); in the present study, a cTFC >23 was observed in 62 and 73% of the patients treated with PS and in the control groups(p=NS), respectively.
However, a recent large scale randomized study sho- wed no benefit from the use of the Guard-Wire system either in terms of myocardial perfusion and STe resolu- tion or 30-day cardiac event, and even using the infarcted size suggested by Tc-sestamibi, the myocardial SPECT
p=NS
0 0.5 1 1.5 2
WMSI baseline WMSI 2 mo 1.5
1.6
1.4 1.6 p=0.007
p=NS
46
51
43 46
0 20 40 60 80 100
LVEF baseline LVEF 2 mo p<0.001
Fig. 2. Changes in the LVEF and LVWMSI during follow-up. LVEF: left ventricular ejection fraction, WMSI: wall motion score index, NS: not sig- nificant.
PercuSurge® Control
A B
might not be sensitive or accurate enough to demonst- rate the extent of subendocardial infarction. However, the inclusion criteria for subjects to that study resulted in the enrollment of patients with a shorter pain-to-bal- loon time, a greater number of low-risk patients, a much higher incidence of abciximab use, lower cTFC and a greater number with a MB score of 3 in the control group.28) Moreover, PCIs were fully protected, with occlu- sion balloon inflation in only 79%.
This study suggests that mechanical prevention of dis- tal embolization might prevent no-reflow and unfavora- ble clinical results during primary PCI, with a substantial benefit expected.
Study limitations
The results of this study should be considered in the light of the following limitations: Firstly, the non-ran- domized small sample size should be noted with caution when interpreting our data. However, the case-matched design of the present study allowed a balanced between- group distribution of the main baseline parameters that are known to affect the prognosis after primary PCI (Table 1). Secondly, the principal end points of the present study were not evaluated by an independent, validated core laboratory, although the angiography, echocardiography and ECG data were analyzed by re- viewers other than the operators; these were also blinded to the treatment.
Conclusions and clinical implications
The adjunctive use of the PercuSurge® Guard-Wire system is feasible and safe during primary PCI in AMI, and seems to reduce microcirculatory damage and im- prove the recovery of the LV function. A larger randomi- zed study will be needed to see whether distal protection devices can reduce the major cardiac events, as well as myocardial damage, after primary PCI.
■ Acknoewledgments
The authors thank Suk-Ja Moon, RN, and Dong-Hoon Hahm, CVRT, for the data collection and angiographic analysis.
REFERENCES
1) Akasaka T, Yoshida K, Kawamoto T, et al. Relation of phasic co- ronary flow velocity characteristics with TIMI perfusion grade and myocardial recovery after primary percutaneous transluminal coronary angioplasty and rescue stenting. Circulation 2000;101:
2361-7.
2) Ito H, Okamura A, Iwakura K, et al. Myocardial perfusion pat- terns related to thrombolysis in myocardial infarction perfusion grades after coronary angioplasty in patients with acute anterior wall myocardial infarction. Circulation 1996;93:1993-9.
3) Poli A, Fetiveau R, Vandoni P, et al. Integrated analysis of myo- cardial blush and ST-segment elevation recovery after successful primary angioplasty: real-time grading of microvascular reper- fusion and prediction of early and late recovery of left ventricular function. Circulation 2002;106:313-8.
4) van’t Hof AW, Liem A, Suryapranata H, Hoorntje JC, de Boer MJ, Zijstra F. Angiographic assessment of myocardial reperfusion in patients treated with primary angioplasty for acute myocardial infarction: myocardial blush grade. Circulation 1998;97:2302-6.
5) Stone GW, Peterson MA, Lansky AJ, Dangas G, Mehran R, Leon MB. Impact of normalized myocardial perfusion after successful angioplasty in acute myocardial infarction. J Am Coll Cardiol 2002;39:591-7.
6) Lepper W, Hoffmann R, Kamp O, et al. Assessment of myocardial reperfusion by intravenous myocardial contrast echocardiography and coronary flow reserve after primary percutaneous translu- minal coronary angioplasty in patients with acute myocardial infarction. Circulation 2000;101:2368-74.
7) Ito H, Maruyama A, Iwakura K, et al. Clinical implications of the “no-reflow” phenomenon: a predictor of complications and left ventricular remodeling in reperfused anterior wall myocardial infarction. Circulation 1996;93:223-8.
8) Eeckhout E, Kern MJ. The coronary no-reflow phenomenon: a review of mechanisms and therapies. Eur Heart J 2001;22:729-39.
9) Hokimoto S, Saito T, Noda K, et al. Relation between coronary thrombus and angiographic no-flow during primary angioplasty in patients with acute myocardial infarction. Jpn Circ J 1999;63:
849-53.
10) Henriques JP, Zijlstra F, Ottervanger JP, et al. Incidence and clinical significance of distal embolization during primary angio- plasty for acute myocardial infarction. Eur Heart J 2002;23:
1112-7.
11) Grube E, Gerckens R, Muller R, Rowold S. Multicenter evalua- tion of a protection catheter system for distal embolization in coronary venous bypass grafts (SVGs). Am J Cardiol 1999;84:
19P. Abstract
12) Claeys MJ, Bosmans J, Veenstra L, Jorens P, de Raedt H, Vrints CJ. Determinants and prognostic implications of persistent ST- segment elevation after primary angioplasty for acute myocardial infarction: importance of microvascular reperfusion injury on clinical outcome. Circulation 1999;99:1972-7.
13) Limbruno U, Petronio AS, Amoroso G, et al. The impact of co- ronary artery disease on the coronary vasomotor response to nonionic contrast media. Circulation 2000;101:491-7.
14) TIMI Study Group. The Thrombolysis in Myocardial Infarction (TIMI) trial: phase I findings. N Engl J Med 1985;312:932-6.
15) Gibson CM, Cannon CP, Daley WL, et al. TIMI frame count: a quantitative method of assessing coronary artery flow. Circulation 1996;93:879-88.
16) Grube E, Gerckens U, Yeung AC, et al. Prevention of distal em- bolization during coronary angioplasty in saphenous vein grafts and native vessels using porous filter protection. Circulation 2001;
104:2436-41.
17) Belli G, Pezzano A, de Biase AM, et al. Adjunctive thrombus aspiration and mechanical protection from distal embolization in primary percutaneous intervention for acute myocardial infarction.
Catheter Cardiovasc Interv 2000;50:362-70.
18) Saber RS, Edwards WD, Bailey KR, et al. Coronary embolization after balloon angioplasty or thrombolytic therapy: an autopsy study of 32 cases. J Am Coll Cardiol 1993;22:1283-8.
19) Giri S, Mitchel JF, Hirst JA, et al. Synergy between intracoronary stenting and abciximab in improving angiographic and clinical outcomes of primary angioplasty in acute myocardial infarction.
Am J Cardiol 2000;86:269-74.
20) Rezkalla SH, Kloner RA. No-reflow phenomenon. Circulation 2002;105:656-62.
21) Yoon MH, Tahk SJ, Choi SY, et al. Effect of distal protection device on the microvascular integrity during primary stenting in acute myocardial infarction: distal protection device in acute myo-
cardial infarction. Korean Circ J 2005;35:106-14.
22) Kim JY, Yoon JH, Lee SH, et al. Efficacy of embolic protection using PercuSurge® GuardWire system during primary percutane- ous coronary intervention with the lesions suggesting large throm- bus burden. Korean Circ J 2003;33:1103-9.
23) Kim HJ, Gwon HC, Yoon JC, et al. Clinical experiences with the PercuSurge® for the coronary lesions with intracoronary throm- bus. Korean Circ J 2002;32:407-12.
24) EPIC Investigators. Use of a monoclonal antibody directed against the glycoprotein IIb/IIIa receptor in high-risk coronary angioplasty.
N Engl J Med 1994;330:956-61.
25) EPILOG Investigator. Platelet glycoprotein IIb/IIIa blockade with abciximab with low dose heparin during percutaneous coronary
revascularization. N Engl J Med 1997;336:1689-96.
26) EPISTENT Investigators. Randomized placebo-controlled and balloon-angioplasty controlled trial to assess safety of coronary stenting with use of glycoprotein IIb/IIIa blockade. Lancet 1998;
352:87-92.
27) Hamada S, Nishiue T, Nakamura S, et al. TIMI frame count im- mediately after primary coronary angioplasty as a predictor of functional recovery in patients with TIMI 3 reperfused acute myo- cardial infarction. J Am Coll Cardiol 2001;38:666-71.
28) Stone GW, Webb J, Cox DA, et al. Distal microcirculatory protec- tion during percutaneous coronary intervention in acute ST-seg- ment elevation myocardial infarction. JAMA 2005;293:1063-72.