교신저자: 이동국, 대구시 남구 대명 4동 3056-6, 705-718, 대구가톨릭대학교 의과대학 신경과학교실 Tel: 053-650-4267, Fax: 053-654-9786, E-mail: [email protected]
Transient loss of consciousness in the elderly often presents one of the most difficult diagnostic chal- lenges, particularly because of the high incidence of chronic medical conditions and associated medi- cation usage. The major differential diagnoses include neurologic and cardiovascular causes, with seiz- ures and syncope leading the list. Syncope, a transient loss of consciousness and postural tone due to reduced cerebral blood flow, is associated with spontaneous recovery. Syncope may result from cardiac, multiple noncardiac, or undetermined causes. It may occur suddenly, without warning, or may be preceded by symptoms of faintness. The differentiation of syncope from seizure is an important, sometimes difficult, diagnostic problem. Because most spells of episodic loss of consciousness occur outside medical observation, the history is the most critical part of evaluation.
Key Words: Syncope, Seizure, History
실신환자의 임상적 접근
이 동 국
대구가톨릭대학교 의과대학 신경과학교실
Clinical Approach to the Patient in Syncope
Dong Kuck Lee, M.D.
Department of Neurology, School of Medicine, Catholic University of Daegu, Daegu, Korea
서 론
노인에서 흔히 생기는 일시적인 의식소실은 진단하기가 힘든 경우가 자주 있다. 왜냐하면 노인은 동반된 질환이 많고 또한 다양한 약물을 복용하고 있기 때문이다. 일시적인 의식소실은 다양한 신경질환 또는 심혈 관질환에 의해 생기는데 대표적인 것이 발작(seizure)과 실신(syncope)이다. 노인 경련은 뇌혈관질환이나 퇴행 성 질환이 있을 때 잘 생긴다. 또한 노인이 되면서 심혈관질환이 증가하고 따라서 다양한 약물복용이 늘어 감에 따라 실신 빈도도 증가한다.
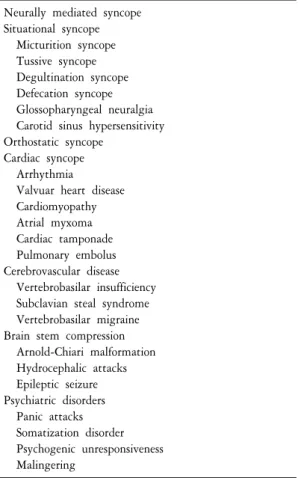
Table 1. Common causes of transient loss of consciousness Neurally mediated syncope
Situational syncope Micturition syncope Tussive syncope Degultination syncope Defecation syncope Glossopharyngeal neuralgia Carotid sinus hypersensitivity Orthostatic syncope
Cardiac syncope Arrhythmia
Valvuar heart disease Cardiomyopathy Atrial myxoma Cardiac tamponade Pulmonary embolus Cerebrovascular disease Vertebrobasilar insufficiency Subclavian steal syndrome Vertebrobasilar migraine Brain stem compression Arnold-Chiari malformation Hydrocephalic attacks Epileptic seizure Psychiatric disorders Panic attacks Somatization disorder Psychogenic unresponsiveness Malingering
본 론
1-12)1. 일시적 의식소실의 흔한 원인
실신같은 뇌관류장애, 뇌허혈, 편두통, 경련, 대사 장애, 및 급성 뇌압상승 등이 있으면 일시적 의식소 실이 생긴다. 그러나 불안, 공황장애, 꾀병, 및 정신 병 경련(psychogenic seizure) 등에서도 비슷한 증상을 보인다. 응급실로 내원하는 흔한 원인중의 하나가 실신이다. 젊은 나이에서는 심장성실신(cardiac syn- cope)이 흔하지만 노인에서는 기립저혈압이나 심혈 관성 원인이 더 흔하다. 과거에는 일시적 의식소실 의 원인을 잘 모르는 경우가 많았지만 최근에는 장 시간 심장감시(cardiac mornitoring), 심장에 대한 전기 생리검사, 기립 스트레스를 유발시키는 두위경사검 사(tilt test), 및 비디오 뇌파검사 등의 발달과 정신과 면담기법의 발전 등으로 인해 많은 원인들이 밝혀 지고 있다. 실신은 심장 부정맥이나 급사할 수도 있 는 위험을 내포하고 있으므로 가볍게 다루어서는 안된다. 일시적 의식소실의 흔한 원인은 Table 1과 같고 특히 노인에서 흔한 원인은 Table 2와 같다.
2. 실신의 정의와 빈도
실신(syncope)은 급작스런 뇌혈류 감소로 인하여 일시적으로 의식을 잃고 자세를 유지하지 못하고 쓰러지는 것으로서, 실신까지는 아니지만 갑자기 힘이 빠지면서 곧 졸도할 것 같은 느낌만 나타나는 것을 전실신 (presyncope)이라고 한다. 이 증상은 수축기 혈압이 60 mmHg 이하로 떨어지거나 뇌혈류가 6∼10초 이상 중단될 때 나타난다. 비교적 갑자기 시작하고 지속기간은 짧으며 저절로 완전히 회복되므로 별다른 소생술은 필요없 다. 환자들이 실신을 표현하는 방법은 매우 다양하여, 일시적 혼란 혹은 약함, 핑돌림, 아찔함, 취한 듯함, 어지럼증, 기억상실, 의식소실, 쓰러짐, 혼수, 및 졸도 등으로 표현한다. 인구의 20∼40%는 일생에 한번은 실신 을 경험한다고 하며, 노인에게서 빈도가 높다. 실신 환자의 60%는 여자이지만 젊은 연령에서는 여자가, 노인 에게서는 남자가 높게 나타난다. 실신 환자의 17~35%에게서 외상이 동반되는데, 작은 외상은 10∼29%, 골절 은 5∼7%, 교통사고는 1∼5%에서 일어나고, 노인 낙상의 약 10%는 실신에 의한 것으로 알려져 있다.
3. 실신의 원인과 분류
실신의 원인은 가만 두면 저절로 회복되는 것부터 만성적이고 반복적이며 잠재적으로 치명적인 것에 이르기까지 다양하다. 그러나 실신은 심장정지를 포함한는 심각한 심장 이상의 조짐일 수도 있으므로 미리 예방하기 위해 검사와 치료가 필요하다. 특히 노인들은 이를 무시하고 일상적인 일로 치부하는 경향이 있으
Table 2. Spells in the elderly: differential diagnosis Neurologic
Seizure
Complex partial
Secondarily generalized tonic-clonic Absence
Nonconvulsive status epilepticus Transient ischemic attack Basilar artery ischemia Transient global amnesia Migraine
Sleep disorder
Nonepileptic psychogenic seizure Cardiac
Obstruction to outflow (aortic stenosis, idiopathic hy- pertrophic subaortic stenosis, pulmonary embolus) Loss of effective pump function (myocardial infarction,
tamponade)
Arrhythmias (bradyarrhythmias, tachyarrhythmias) Reflexogenic
Vasovagal syncope
Situational syncope (cough, micturition, swalllowing) Carotid sinus hypersensitivity
Orthostatic hypotension Medication effect Hypovolemic Neurogenic Metabolic Hypoglycemia Hyperventilation
Table 3. Classification and etiology of syncope Cardiac
Arrhythmias Brdyarrhythmias Tachyarrhythmias Reflex arrhythmias Decreased cardiac output Outflow obstruction Inflow obstruction Cardiomyopathy Hypovolemic Hypotensive Vasovagal attack Drugs
Dysautonomia Cerebrovascular Carotid disease Vertebrobasilar disease Vasospasm
Takayasu’s disease Metabolic
Hypoglycemia Anemia Anoxia Hyperventilation Multifactorial
Vasovagal (vasodepressor) attack Cardiac syncope
Situational: cough, micturition, defecation, swallowing, diving, Valsalva maneuver
므로 각별한 주의가 필요하다. 보통 혈관긴장도 또는 혈액량의 저하, 폐쇄와 심장부정맥을 포함한 심혈관질 환, 또는 뇌혈관질환 등이 발생하면 일시적 뇌혈류 감소가 생겨 실신이 생긴다. 그러나 그 외에도 저혈압, 대사성 질환, 과호흡, 기타 다양한 원인에 의해 실신이 생긴다(Table 3).
4. 실신의 기전
의식이란 자신과 주변을 인식하는 것에 반해 무의식이란 자신과 주변을 인식하지 못해 외부 자극에 대해 적절한 반응을 하지 못하는 상태를 말한다. 의식을 유지하기 위해선 뇌피질과 뇌간 그물활동계가 긴밀하게 잘 작동해야 한다. 만약 이런 조직에 기능이상이 생기면 의식이 저하된다. 따라서 약 5∼8초간 심장 무수축 (asystole) 또는 수축기 혈압이 60 mmHg 이하로 떨어져 뇌혈류감소가 생기거나 산소나 포도당같이 뇌에 필수 적인 영양소가 공급되지 않거나 신경독소(neurotoxin)에 의해 뇌기능장애가 생기거나 또는 경련같이 뇌 전기 활동에 문제가 생기면 의식이 저하된다. 결국 실신이란 급성으로 뇌순환이 일시적으로 감소하여 의식소실 이 생기면서 근긴장도가 떨어진 상태이다.
5. 실신의 임상 증상(Table 4)
실신의 임상양상은 원인에 따라 차이가 난다. 가장 흔한 유형은 혈관억제(vasodepressor) 또는 혈관미주신경
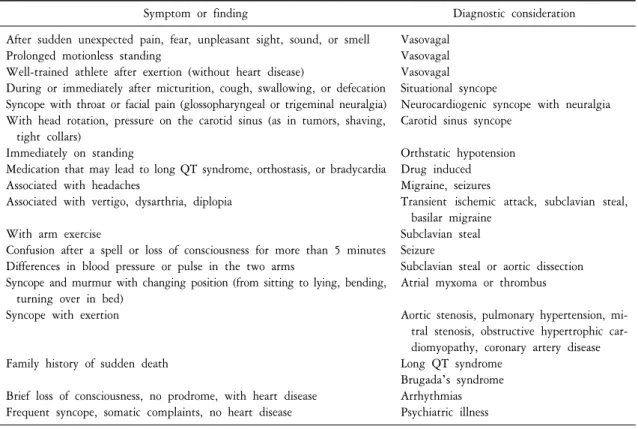
Table 4. Clinical features suggesting specific causes
Symptom or finding Diagnostic consideration
After sudden unexpected pain, fear, unpleasant sight, sound, or smell Prolonged motionless standing
Well-trained athlete after exertion (without heart disease)
During or immediately after micturition, cough, swallowing, or defecation Syncope with throat or facial pain (glossopharyngeal or trigeminal neuralgia) With head rotation, pressure on the carotid sinus (as in tumors, shaving,
tight collars)
Immediately on standing
Medication that may lead to long QT syndrome, orthostasis, or bradycardia Associated with headaches
Associated with vertigo, dysarthria, diplopia With arm exercise
Confusion after a spell or loss of consciousness for more than 5 minutes Differences in blood pressure or pulse in the two arms
Syncope and murmur with changing position (from sitting to lying, bending, turning over in bed)
Syncope with exertion
Family history of sudden death
Brief loss of consciousness, no prodrome, with heart disease Frequent syncope, somatic complaints, no heart disease
Vasovagal Vasovagal Vasovagal Situational syncope
Neurocardiogenic syncope with neuralgia Carotid sinus syncope
Orthstatic hypotension Drug induced Migraine, seizures
Transient ischemic attack, subclavian steal, basilar migraine
Subclavian steal Seizure
Subclavian steal or aortic dissection Atrial myxoma or thrombus
Aortic stenosis, pulmonary hypertension, mi- tral stenosis, obstructive hypertrophic car- diomyopathy, coronary artery disease Long QT syndrome
Brugada’s syndrome Arrhythmias Psychiatric illness
실신(vasovagal syncope)으로 대개 환자가 앉아 있거나 서있는 자세에서 시작하며 조짐이 먼저 나타난다. 메스 껍고 어지러우면서 휘청거리고 쓰러질 것 같은 두려움과 함께 얼굴이 창백해 지고 전신에 식은땀을 흘린다.
침이 고이고 상복부 불편감을 느끼며 욕지기나 일부에서 구토가 동반되기도 하는데 환자는 이러한 증상을 완화시키기 위하여 하품을 하거나 한숨을 쉬거나 숨을 크게 쉬기도 한다. 이러한 조짐은 수초에서 수분간 지속되는데, 만약 이 기간에 환자가 재빨리 누워버리면 회복될 수 있다. 실신 때 생기는 의식소실의 정도와 기간은 다양하다. 환자에 따라서는 의식을 완전히 잃지 않고 말소리를 듣거나 주위사람의 형체를 희미하나 마 알아보기도 하지만, 의식을 잃고 전혀 반응이 없어지는 경우가 더 흔하다. 환자는 전혀 움직이지 않고 누워있는데 골격근은 모두 이완된 상태지만 조임근(sphincteric muscle)의 조절은 대부분 유지된다. 동공은 확대되고 맥박은 느리고 약하거나 감지하기 힘든데 수축기 혈압이 60 mmHg 이하로 떨어지고 호흡도 감지 하기 어렵다. 그러나 일단 수평으로 누우면 혈액순환이 회복되면서 맥박이 다시 강해지고 안색이 정상으로 회복된다.
1) 신경탓 실신(Neurally mediated syncope)
신경탓 실신은 혈관미주신경 또는 반사 실신이라고도 불리며 심장병이 없는 사람에게 가장 흔히 생기는 실신이다. 동맥이나 내장 기계수용체가 자극되면 반사가 일어나 실신이 생긴다. 방광, 위장관, 또는 경동맥 동(carotid sinus)에 있는 기계수용체가 압박이나 팽만(distension)으로 인해 자극되면 뇌간으로 구심 신호를 전달하고 그 후 원심 신호는 미주신경을 통해 심장결절로 전달되면 서맥(bradycardia)이 생긴다. 한편 반사로 인해 혈관확장이 생겨 혈압을 떨어뜨리는 것도 실신의 한 원인이 된다. 반사는 급성 통증이나 감정변화에 의해 악화되지만 다른 원인없이 서 있거나 걸을 때 하지 정맥으로 혈액이 몰려 반사가 생기기도 한다. 서맥
Table 5. Neurally mediated syncope Discriminating features
1. Evidence of an overactive autonomic nervous system
2. Positive tilt table test with reflex bradycardia and/or peripheral vasodilatation with reproduction of the syncopal episode 3. Sometimes triggered by specific circumstances (situational syncope)
Consistent features
1. Usually occurs in younger patients
2. Usually occurs while standing in a hot, crowded room
3. Physical examination, screening laboratory tests, and ECG are normal 4. Consciousness regained almost immediately after falling
Variable features
1. Presyncopal symptoms of blurred vision, nausea, diaphoresis, generalized weakness, and sense of impending loss of consciousness
2. Brief myoclonic jerks accompanying loss of consciousness
과 저혈압이 생기면 뇌순환이 떨어져 의식소실이 온다. 신경탓 실신은 앉아 있거나 심지어는 누워 있을 때도 생기지만 대부분 덥거나 복잡한 환경에 있거나 탈수상태에서 잘 생긴다. 실신 전에 오심, 눈이 침침함, 땀, 전신 무력, 또는 거의 의식을 잃을 것 같은 증상이 선행된다. 그 후 환자는 의식을 잃고 쓰러진다. 가끔 요실금이나 근간대경련(myoclonus)을 잠깐 보여 경련으로 오인되기도 한다. 이때 생기는 근간대경련은 뇌혈 류감소와 저산소증 때문에 생긴다. 보통 실신후 바로 의식이 회복되지만 잠깐 동안 혼동(confusion)을 보이다 가 원래 상태로 돌아간다. 신경탓 실신은 특징적 병력과 진찰을 통해 다른 원인을 제외시키면 진단된다 (Table 5).
2) 환경탓 실신(Situational syncope)
특별한 환경에서 신경탓 실신이 생긴 경우를 환경탓 실신이라고 한다. 정맥천자(venipuncture) 중 생기는 실신이 가장 흔한 환경탓 실신이다. 또한 갑자기 심한 통증이나 감정 충격이 있으면 서맥, 혈관확장, 및 일시적 의식소실이 생긴다. 환경탓 실신이 자주 생기면 일단 이런 환경을 피하거나 변화시켜야 한다.
(1) 배뇨(Micturition)실신: 배뇨실신이란 배뇨중이거나 배뇨 직후에 실신이 생기는 것이다. 보통 자다가 한밤중에 소변을 보는 중 수축된 방광벽에 있는 기계수용체가 자극되어 반사 서맥과 혈관확장이 생겨 실신 하게 된다. 더구나 남자라면 서서 소변을 보는 중 기립저혈압이 생겨 더욱 실신을 유발하게 된다. 치료는 배뇨실신에 대해 이해하고 좌변기에 앉아서 소변을 보도록 권하는 것이다.
(2) 기침실신: 만성 폐쇄성 호흡기질환에서처럼 심한 기침을 하면 흉압이 올라가 정맥순환을 억제하고 심장 박출량을 감소시키며 반사 서맥과 혈관확장을 일으켜 실신이 생긴다. 따라서 기침을 일으키는 원인을 치료하는 것이 가장 우선이다.
(3) 삼킴(Swallow)실신: 삼킬 때 식도의 기계수용체가 자극되어 실신이 생기며 특히 크고 딱딱한 음식을 삼킬 때 더 잘 생긴다. 대부분 식도협착(stricture)이나 식도연축(spasm)이 있는 환자에서 잘 생기므로 삼킴실 신에서는 식도질환을 확인하고 치료하는 것이 우선이다.
(4) 배변(Defecation)실신: 배변시 심한 통증이 있을 때 배에 힘을 주면 복압이 올라가면 횡경막 위치에 서 아래대정맥(inferior vena cava)을 막아 실신이 생긴다.
(5) 혀인두 신경통(Glossopharyngeal neuralgia): 인두, 목, 외이도로 극심한 신경통증이 생기면 반사 서맥, 혈관확장, 저혈압이 와서 실신한다.
(6) 경동맥동 과민(Carotid sinus hypersensitivity): 특히 노인이나 동맥경화성 혈관병이 있는 사람에서 경동맥동을 자극하면 미주신경을 통해 반사 서맥과 혈관확장이 생겨 실신한다. 목이 꽉 조이는 옷을 입고
Table 7. Vertebrobasilar insufficiency Discriminating features
1. Other brainstem signs and symptoms accompany syncope 2. Cerebral angiogram is abnormal
Consistent features
1. Usually takes place in elderly patients 2. Occurs in any position
Variable features
Recurrent episodes may lead to a fixed neurologic deficit
Table 6. Orthostatic hypotension Discriminating features
1. Significant drop in orthostatic blood pressure 2. Often associated with a decrease in muscle tone Consistent features
1. Most common cause of syncope in elderly patients
2. Occurs while standing or when making postural changes to a more upright position 3. Consciousness regained almost immediately after falling
4. Usually aborted if the patient can immediately assume a sitting or prone position Variable features
Presyncopal symptoms of blurred vision, nausea, and disequilibrium 있거나 면도를 하다가 또는 고개를 돌리다가 실신하기도 한다.
3) 기립저혈압
이런 병은 노인에서 흔하며 심혈관계가 자세변화에 빨리 적응하지 못하여 혈압저하, 뇌관류 부족, 및 의식소실이 생긴다. 노인에서 기립저혈압의 가장 흔한 원인은 이뇨제 과용, 항고혈압약, 진정제 또는 여러 약을 함께 복용하는 경우 등이다. 그 외에도 심한 빈혈, 탈수, 장기간 요양, 척수질환, 자율신경병, 신경퇴행 병, 식후 저혈압, 부신 기능부전, 신생물딸림증후군(paraneoplastic syndrome), 또는 유전성 질환 등에서도 기립 저혈압이 생길 수 있다. 진단은 기립저혈압이 있는지 확인해 보면 된다. 만약 갑자기 서면 평소보다 수축기 혈압이 20 mmHg이상 떨어지거나 전체 수축기 혈압이 90 mmHg보다 떨어지고 실신하려고 하면 알 수 있다.
치료는 원인인자를 제거하고 필요하면 광물코르티코이드같은 약을 쓰며 평소 자세를 변화시킬 때 천천히 적응하면서 움직이도록 권한다. 자세 빈맥증후군(postural tachycardia syndrome)이란 갑자기 서면 심박동이 빨라지고 두근거리며 눈이 침침해지면서 실신이 오는 증상을 말한다(Table 6).
4) 심장탓 실신
갑자기 심장박출량이 줄어들면 뇌관류가 줄고 의식소실이 생긴다. 흉통, 두근거림, 힘든 작업후 또는 서 있는 자세가 아닌데 실신이 생긴 경우에는 심장탓 실신을 의심한다. 특히 판막성 심장병이나 부정맥이 있으 면 실신 위험상이 높아진다. 만약 심전도검사에서는 이상이 없는데도 심장탓 실신이 의심되면 장시간 심장 감시검사를 해 보는 것이 좋다.
5) 뇌혈관질환에 의한 실신
뇌혈관질환에 의해 뇌간허혈이 생기면 상행 그물 각성계에 기능이상이 와서 실신이 일어난다. 편두통이 나 쇄골하 훔침 증후군(subclavian steal syndrome)에서도 실신이 생긴다. 추골기저동맥 뇌졸중에 의한 실신에
Figure 1. Diagnostic appro- ach to a patient with syncope.
서는 현훈, 복시, 구음장애, 실조, 협동운동 장애, 또는 운동이나 감각장애 등 뇌간허혈 증상을 보일 수 있다 (Table 7).
6) 뇌간 압박에 의한 실신
일시적 뇌압상승은 뇌간을 압박한 결과 그물 각성계, 뇌간 혈압상승 중추, 및 추골기저 혈액순환 등에 기능이상을 일으켜 실신이 생긴다.
7) 기타 원인불명 실신
여러 가지 검사를 해도 1/3∼1/2에서는 원인을 알 수 없다. 이런 경우에는 정기적으로 경과를 관찰하며 추적검사를 하는 것이 좋다.
6. 실신의 진단검사
만약 실신의 원인이 명확하다면 병력과 진찰만으로도 충분히 진단이 가능하다. 많은 실신들이 특이 상황 에서 유발되므로 실신했을 때의 상황을 재현시켜 보면 진단에 도움이 된다. 진단검사는 이미 의심되는 원인 을 확인하는 단계이다. 그중 심전도는 경비가 적고 간단하지만 중요한 정보를 주는 검사이므로 대부분의 실신환자에서 시행한다. 특히 실신이 단순한 정도인지 아니면 심각한 문제가 있는 것인지 빨리 평가하는데 심전도가 중요하다. 만약 이미 심장병이 있거나 심전도에 이상이 있으며 부정맥 증상이 있고 실신이 자꾸 재발되면 24시간 Holter검사같이 장시간 심장기능을 평가하는 검사를 한다. 경동맥 마사지는 경동맥 과민을
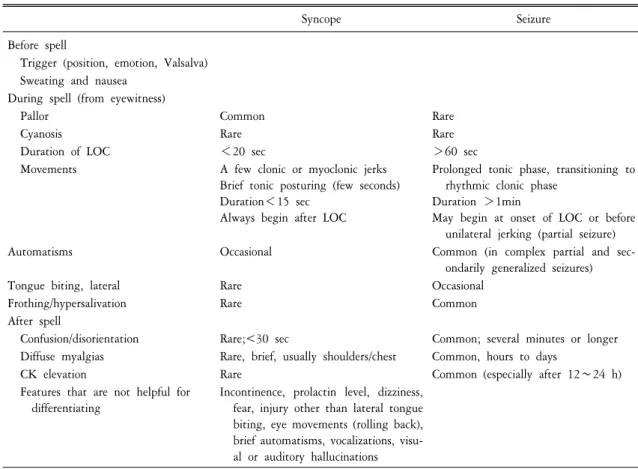
Table 8. Syncope versus seizure: useful distinguishing feature
Syncope Seizure
Before spell
Trigger (position, emotion, Valsalva) Sweating and nausea
During spell (from eyewitness)
Pallor Common Rare
Cyanosis Rare Rare
Duration of LOC <20 sec >60 sec
Movements A few clonic or myoclonic jerks Brief tonic posturing (few seconds) Duration<15 sec
Always begin after LOC
Prolonged tonic phase, transitioning to rhythmic clonic phase
Duration >1min
May begin at onset of LOC or before unilateral jerking (partial seizure)
Automatisms Occasional Common (in complex partial and sec-
ondarily generalized seizures)
Tongue biting, lateral Rare Occasional
Frothing/hypersalivation Rare Common
After spell
Confusion/disorientation Rare;<30 sec Common; several minutes or longer Diffuse myalgias Rare, brief, usually shoulders/chest Common, hours to days
CK elevation Rare Common (especially after 12∼24 h)
Features that are not helpful for differentiating
Incontinence, prolactin level, dizziness, fear, injury other than lateral tongue biting, eye movements (rolling back), brief automatisms, vocalizations, visu- al or auditory hallucinations CK: creatine kinase, GTC: generalized tonic-clonic, LOC: loss of consciousness.
아는데 도움을 주지만 심실 세동(ventricular fibrillation), 심장 무수축, 뇌졸중, 및 급사 위험이 있으므로 주의해 야 한다. 기립경사검사는 신경탓 실신을 진단하는데 도움이 된다. 일반적인 대사 검사나 혈액상(hemogram) 은 빈혈을 아는 정도 외에는 실신 진단에 큰 도움이 되지 않는다. 병력을 보고 약물과용이나 복용유무를 확인하는 것은 필요하다. 특히 코카인은 심장 부정맥이나 경련을 유발시킬 수 있으므로 주의한다. CT, MRI, 또는 MRA같은 신경영상검사는 뇌혈관질환같은 중추신경계 질환을 진단하는데 도움이 되며 뇌파검사는 경련성 질환을 아는데 유용하다. 만약 광범위한 검사를 해도 원인불명의 실신이 반복되면 정신과 면담도 필요하다. 특히 불안, 우울증, 신체화(somatization), 약물이나 알코올 중독 병력이 있는 경우에 더욱 그러하다.
경련, 비간질성 정신 경련, 또는 가성 경련 등이 의심되면 비데오 뇌파 및 심전도검사가 필요하다. 실신을 진찰하기 위해서는 대부분 외래에서 검사하지만 심각한 문제가 의심되면 입원시켜두고 경과를 보면서 진 단한다(Figure 1).
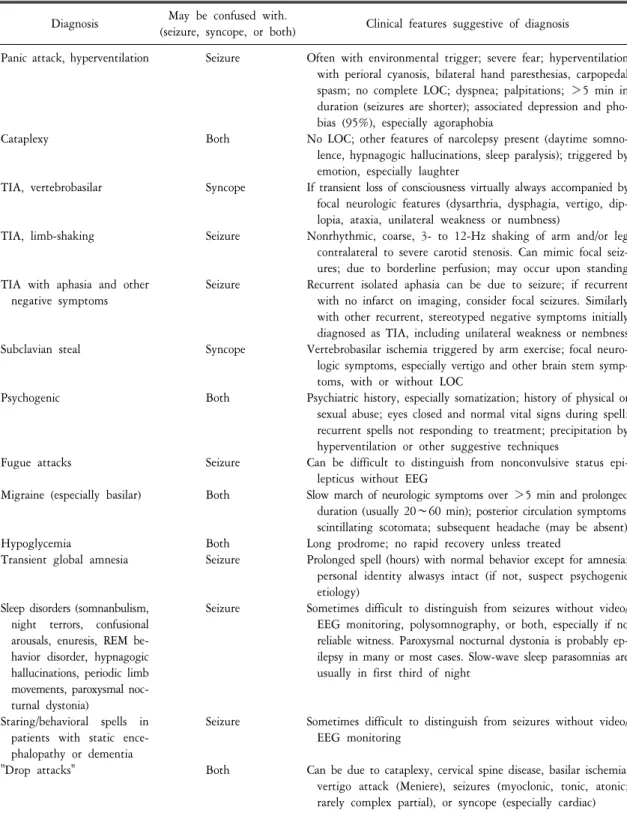
7. 실신의 감별진단
의식을 잃기 전후의 증상이나 상황을 살펴보면 실신과 다른 질환들과 감별진단이 가능하다. 실신은 경련, 국소 뇌허혈, 일과성 전체 기억상실(transient global amnesia), 수면장애, 비간질성 정신 경련(nonepileptic
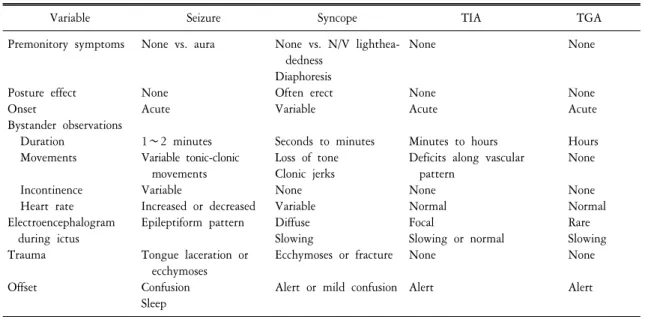
Table 9. Variables that distinguish common spells in the elderly
Variable Seizure Syncope TIA TGA
Premonitory symptoms
Posture effect Onset
Bystander observations Duration
Movements Incontinence Heart rate Electroencephalogram
during ictus Trauma Offset
None vs. aura
None Acute 1∼2 minutes Variable tonic-clonic
movements Variable
Increased or decreased Epileptiform pattern Tongue laceration or
ecchymoses Confusion Sleep
None vs. N/V lighthea- dedness
Diaphoresis Often erect Variable
Seconds to minutes Loss of tone Clonic jerks None Variable Diffuse Slowing
Ecchymoses or fracture Alert or mild confusion
None
None Acute
Minutes to hours Deficits along vascular
pattern None Normal Focal
Slowing or normal None
Alert
None
None Acute Hours None None Normal Rare Slowing None Alert
N/V: nausea and vomiting, TGA: transient global amnesia, TIA: transient ischemic attack.
psychogenic seizure), 심혈관 실신, 반사(reflexogenic) 실신, 및 기립 실신, 불안 및 과호흡 증후군, 저혈당, 히스테 리, 공황장애, 및 편두통 등과 감별해야 한다(Table 2, 4, 8∼10)
8. 실신의 치료
실신이 생기면 우선 뇌혈류를 최대로 올리기 위해, 앉아 있다면 머리를 양 무릎 사이로 내리거나, 누운 채 다리를 올린다. 꼭 조이는 옷은 느슨하게 풀어주고 머리를 돌려 혀가 기도를 막지 않도록 하여야 한다.
동시에 대량 내부출혈, 무통 심근경색이나 부정맥 등과 같이 응급치료가 필요한 실신인지를 먼저 구분하는 것이 중요하다. 특별한 원인이 없는데 노인에게 갑자기 실신이 일어났다면 완전방실차단이나 다른 부정맥 을 의심한다.
실신의 예방은 발병기전에 따라 다르다. 혈관억제 실신환자에서는 더운 환경, 허기, 피곤, 또는 음주같이 혈관확장이 잘 일어날 만한 상황이나 정서적 흥분상태를 피하도록 한다. 기립저혈압 환자에게는 잠자리에 서 급히 일어나지 않도록 조심시킨다. 대신 처음에 수 초간 다리 운동을 하고 침대 모서리에 앉았을 때 어지럼증을 느끼지 않으면 걷기 시작하도록 한다. 베게머리를 높인 채 잠을 자거나 몸에 꼭 맞는 복부 탄력 압박대나 탄력양말을 착용하는 것도 도움된다. 만성 기립저혈압 환자에게는 fludrocortisone acetate를 하루에 0.05∼0.4 mg을 나누어 복용하게 하고 염분섭취를 늘려 혈액용적을 늘리는 것도 도움된다. 신경심장 혹은 혈관억제 실신에서는 acebutolol, atenolol 또는 disopyramide을 쓴다. 목동맥팽대 실신 환자는 목 칼라가 넉넉한 옷을 입어야 하고 한쪽을 쳐다볼 때 목만 돌리지 말고 몸 전체를 돌리도록 한다. 실신 시에 심한 서맥이나 저혈압이 생기면 각각 atropine이나 교감신경계 약물을 사용한다. 혈관미주신경 실신은 propantheline에 잘 반응한다. 그러나 항고혈압제, 항정신병제, 항우울제, 항콜린제, levodopa, dopamine 길항제, 기타 항파킨슨제, 또는 sildenafil 등은 실신을 악화시킬 수 있으므로 주의한다. 한편 자주 실신을 하는 경우에는 생활주변 환경 을 정리해 두고 필요하면 편한 신발이나 보조기를 사용하며 응급시 연락처를 준비해 두는 등 평소 예방책을 준비하는 것이 좋다.
Table 10. Differential diagnosis of seizures and syncope Diagnosis May be confused with.
(seizure, syncope, or both) Clinical features suggestive of diagnosis Panic attack, hyperventilation
Cataplexy
TIA, vertebrobasilar
TIA, limb-shaking
TIA with aphasia and other negative symptoms
Subclavian steal
Psychogenic
Fugue attacks
Migraine (especially basilar)
Hypoglycemia
Transient global amnesia
Sleep disorders (somnanbulism, night terrors, confusional arousals, enuresis, REM be- havior disorder, hypnagogic hallucinations, periodic limb movements, paroxysmal noc- turnal dystonia)
Staring/behavioral spells in patients with static ence- phalopathy or dementia
"Drop attacks"
Seizure
Both
Syncope
Seizure
Seizure
Syncope
Both
Seizure Both
Both Seizure
Seizure
Seizure
Both
Often with environmental trigger; severe fear; hyperventilation with perioral cyanosis, bilateral hand paresthesias, carpopedal spasm; no complete LOC; dyspnea; palpitations; >5 min in duration (seizures are shorter); associated depression and pho- bias (95%), especially agoraphobia
No LOC; other features of narcolepsy present (daytime somno- lence, hypnagogic hallucinations, sleep paralysis); triggered by emotion, especially laughter
If transient loss of consciousness virtually always accompanied by focal neurologic features (dysarthria, dysphagia, vertigo, dip- lopia, ataxia, unilateral weakness or numbness)
Nonrhythmic, coarse, 3- to 12-Hz shaking of arm and/or leg contralateral to severe carotid stenosis. Can mimic focal seiz- ures; due to borderline perfusion; may occur upon standing Recurrent isolated aphasia can be due to seizure; if recurrent
with no infarct on imaging, consider focal seizures. Similarly with other recurrent, stereotyped negative symptoms initially diagnosed as TIA, including unilateral weakness or nembness Vertebrobasilar ischemia triggered by arm exercise; focal neuro- logic symptoms, especially vertigo and other brain stem symp- toms, with or without LOC
Psychiatric history, especially somatization; history of physical or sexual abuse; eyes closed and normal vital signs during spell;
recurrent spells not responding to treatment; precipitation by hyperventilation or other suggestive techniques
Can be difficult to distinguish from nonconvulsive status epi- lepticus without EEG
Slow march of neurologic symptoms over >5 min and prolonged duration (usually 20∼60 min); posterior circulation symptoms;
scintillating scotomata; subsequent headache (may be absent) Long prodrome; no rapid recovery unless treated
Prolonged spell (hours) with normal behavior except for amnesia;
personal identity alwasys intact (if not, suspect psychogenic etiology)
Sometimes difficult to distinguish from seizures without video/
EEG monitoring, polysomnography, or both, especially if no reliable witness. Paroxysmal nocturnal dystonia is probably ep- ilepsy in many or most cases. Slow-wave sleep parasomnias are usually in first third of night
Sometimes difficult to distinguish from seizures without video/
EEG monitoring
Can be due to cataplexy, cervical spine disease, basilar ischemia, vertigo attack (Meniere), seizures (myoclonic, tonic, atonic;
rarely complex partial), or syncope (especially cardiac) LOC: loss of consciousness, TIA: transient ischemic attack.
9. 실신의 예후
실신의 예후는 원인질환에 따라 다르다. 대부분에서는 양성이지만 적은 수에서는 급사의 경고징후가 되 기도 한다. 허혈성 또는 구조적인 심장병에 의한 실신의 경우에는 다음 1년 동안 약 20%에서 급사할 수 있다. 그러나 대부분 자연스럽게 회복되며 다양한 검사를 해도 실신의 원인을 알아내지 못한 경우에는 급사 할 가능성이 아주 낮다.
결 론
일시적 의식소실은 흔한 증상이다. 특히 실신과 경련이 가장 흔한 원인이지만 그 외에도 다양한 병을 감별해야 한다. 실신을 진단하기 위해서는 우선적으로 심장병이 있는지 알아 보는 것이 중요하다. 특히 원래 심장병이 있거나 심전도에 이상이 있고 노인이며 자세 변화와 상관없이 실신이 생기고 발병 당시 오심이나 땀 같은 자율신경 이상증상이 없었다면 더욱 심장병에 의한 실신을 생각해야 한다. 한편 혈관미주 신경실신을 포함한 신경탓 반사 실신과 기립저혈압도 중요 원인이다. 일단 일시적 의식소실이 있으면 약복 용과 과거력을 포함한 상세한 병력청취 후 적절한 검사를 통한 임상적 분석이 진단에 가장 중요하다. 그러 나 의식소실이 산발적으로 생긴 경우에는 진단이 어려울 때도 많다. 특히 치료에 반응이 없다면 그 원인을 알기는 더욱 힘들다. 그러나 최근에는 뇌와 심장병에 대한 다양한 진단기술이 발달하여 일시적 의식소실의 많은 경우에 그 원인을 알 수 있게 되었다.
참고문헌
1. Nei M, Ho RT. Transient loss of consciousness: Syncope and seizure. In: Sirven JI, Malamut BL. Clinical neurology of the older adult. 1st ed. New York: Lippincott Williams & Wilkins; 2002. p. 76-89.
2. Drislane FW, Transient events. In: Samuels MA, Feske SK. Office practice of neurology. 2nd ed. New York: Churchill Livingstone;
2003. p. 126-37.
3. DeMyer WE. Technique of the neurologic examination. 5th ed. New York: McGraw Hill; 2004. p. 614-25.
4. Lindsay KW, Bone I. Neurology and neurosurgery illustrated. 4th ed. New York: Churchill Livingstone; 2004. p. 88.
5. Bleck TP. Levels of consciousness and attention. In: Goets CG. Textbook of clinical neurology. 3rd ed. New York: Saunders Elsevier; 2007. p. 13.
6. Bruni J. Episodsic impairment of consciousness. In: Bradley WG, Daroff RB, Fenichel GM, Jankovic J. Neurology in clinical practice. 5th ed. New York: Butterworth Heinemann Elsevier; 2008. p. 11-20.
7. Carlson MD. Syncope. In: Fauci AS, Kasper DL, Longo DL, Braunwald E, Hauser SL, Larry Jameson J, Loscalzo J. Harrison's Principles of internal medicine. 17th ed. New York: McGraw Hill Medical; 2008. p. 139-44.
8. Hankey GJ, Wardlaw JM. Disorders of consciousness. Clinical neurology. 1st ed. New York: Manson Publishing; 2008. p. 59-64.
9. Simon RP. Syncope. In: Lee G, Ausiello D. Cecil medicine. 23rd ed. New York: Saunders Elsevier; 2008. p. 2687-91.
10. Massey AD. Syncope and seizures. In: Corey-Bloom J, David RB. Clinical adult neurology. 3rd ed. New York: Demos Medical;
2009. p. 81-91.
11. Ropper AH, Samuels MA. Faintness and syncope. Adams and Victor's Principles of neurology. 9th ed. New York: McGraw Hill Medical; 2009. p. 362-73.
12. Hirsch LJ, Pedley TA. Syncope, Seizures and their mimics. In: Rowland LP, Pedley TA. Merritt's neurology. 12th ed. New York:
Williams & Wilkins; 2010. p. 15-21.
= 국문요약 =
임상적으로 일시적 의식소실은 흔한 증상이다. 특히 실신과 경련이 가장 흔한 원인이지만 그 외에도 다양한 병을 감별해야 한다. 노인에서 흔히 생기는 일시적인 의식소실은 진단하기가 힘든 경우가 자주 있다. 왜냐하면 노인은 노화에 의해 동반된 질환이 많고 또한 다양한 약물을 복용하고 있기 때문이다. 이 종설에서는 일시적 의식소실의 흔한 원인, 실신의 정의, 빈도, 원인, 분류, 기전, 증상, 진단검사, 감별진단, 치료, 및 예후에 대하여 간단히 정리했다. 일단 일시적 의식소실이 있으면 약복용 과 과거력을 포함한 상세한 병력청취 후 적절한 검사를 통한 임상적 분석이 진단에 가장 중요하다.
그러나 의식소실이 산발적으로 생긴 경우에는 진단이 어려울 때도 있다. 특히 치료에 반응이 없다면 그 원인을 알기는 더욱 힘들다. 그러나 최근에는 뇌와 심장병에 대한 다양한 진단기술이 발달하여 일시적 의식소실의 많은 경우에 그 원인을 알 수 있게 되었다.
중심 단어: 실신, 경련, 병력