Received August 3, 2018; revised October 9, 2018; accepted October 27, 2018.
Corresponding author: Seung-Woon Rha, Cardiovascular Center, Korea University Guro Hospital, 148 Gurodong-ro, Guro-gu, Seoul 08308, Korea. E-mail:
[email protected]
Copyright Ⓒ 2018 The Korean Academy of Clinical Geriatrics
This is an open access article distributed under the term s of the Creative Com m ons Attribution Non-Com m ercial License (http://creativecom m ons.org/licenses/by-nc/4.0) which perm its unrestricted non-com m ercial use, distribution, and reproduction in any m edium , provided the original work is properly cited.
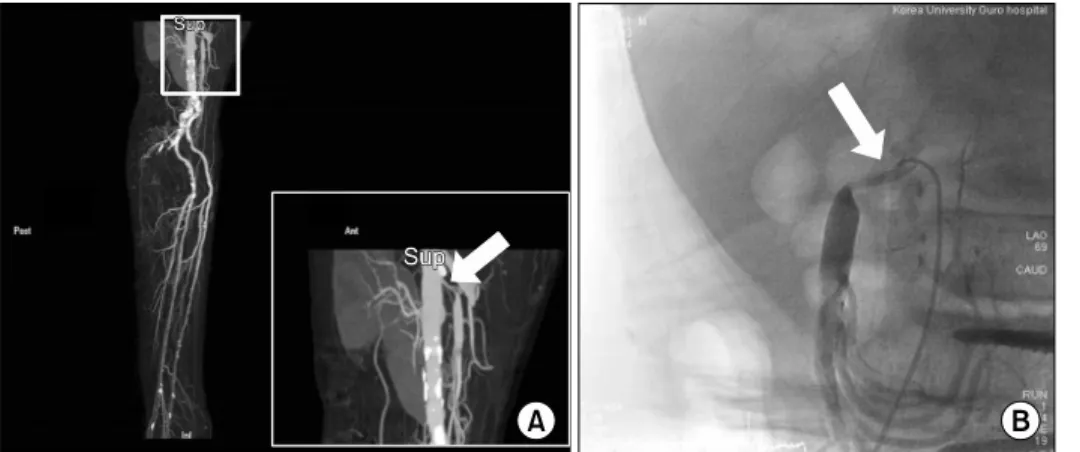
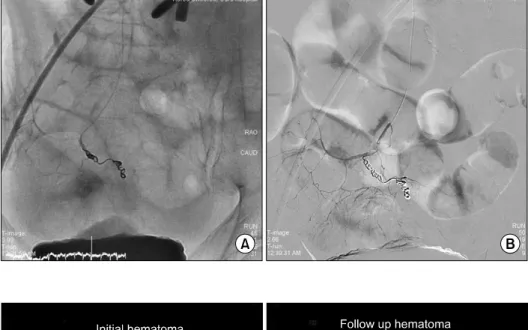
Successful Management of Spontaneous Intraperitoneal Hemorrhage Occurred after Superior Mesenteric Artery Stenting
Ji-Young Park
1, Seung-Woon Rha
21
Division of Cardiology, Department of Internal Medicine, Nowon Eulji Medical Center, Eulji University, Seoul, Korea;
2