156
책임저자: 이동호, 대전광역시 중구 대흥동 520-2 301-723, 가톨릭대학교 대전성모병원 외과 Tel: 042-220-9520, Fax: 042-220-9565
E-mail: [email protected]
접수일:2008년 4월 15일, 게재승인일:2008년 5월 19일
유두상 갑상선암에서 종양의 크기에 따른 중앙 경부림프절 전이 및 이와 관련된 인자에 대한 비교분석
가톨릭대학교 의과대학 외과학교실
이관주ㆍ김형래ㆍ김세준ㆍ이상철ㆍ김정구ㆍ성기영ㆍ박우찬ㆍ오세정ㆍ안창준ㆍ이동호
Analysis of the Relationship between Central Cervical Lymph Node Metastasis from Papillary Thyroid Carcinoma and the Associated Factors according to the Tumor Size
Kwan Ju Lee, M.D., Hyung Rae Kim, M.D., Say June Kim, M.D., Sang Chul Lee, M.D., Jeong Goo Kim, M.D., Gi Young Sung, M.D., Woo Chan Park, M.D.,
Se Jeong Oh, M.D., Chang Joon Ahn, M.D., Dong Ho Lee, M.D.
Department of Surgery, College of Medicine, The Catholic University of Korea, Seoul, Korea
Purpose: The aim of this study was to analyze the relationship between central lymph node metastasis and the associated factors in patients with papillary thyroid carcinoma (PTC) according to the tumor size, and we wanted to determine an appropriate treatment for PTC.
Methods: From June 2005 to May 2007, 218 patients with PTC underwent total thyroidectomy or lobectomy, and they also received central lymph node dissection at our institution. The patients were divided into three groups: group 1 (tumor ≤5 mm), group 2 (5 mm<tumor≤10 mm), and group 3 (tumor>10 mm). We retrospectively reviewed these patients to analyze the relationship between tumor size and the clinicopathological characteristics, including age, gender, lymph node metastasis, extrathyroidal extension, capsular invasion and lymphovascular invasion.
Results: There were 47 (21.6%) patients in group 1, 101 (46.3%) patients in group 2 and 70 (32.1%) patients in group 3. The tumor size was closely correlated with the presence of extrathyroidal extension, capsular invasion and lymph node metastasis (P<0.001). Lymph node metastasis was not only closely correlated with tumor size, but it was also significantly associated with extrathyroidal extension, capsular invasion and lymphovascular invasion (P<0.05).
Conclusion: Our study confirmed that some factors, including central lymph node metastasis, capsular invasion and extrathyroidal extension, were frequently observed in patients with papillary thyroid microcarcinoma (PTMC), and central lymph node metastasis was related to tumor size, extrathyroidal extension, capsular invasion and lymphovascular invasion. Therefore, routine central lymph node dissection is recommended during the initial surgery for patients with PTMC. (J Korean Surg Soc 2008;75:156-161)
Key Words: Papillary thyroid carcinoma, Papillary thyroid microcarcinoma, Central cervical lymph node, Tumor size 중심 단어: 유두상 갑상선암, 유두상 갑상선 미세암, 중앙 경부림프절, 종양크기
서 론
유두상 갑상선암은 내분비암 중 가장 흔한 악성 종양이 고 전체 갑상선암의 80∼90%를 차지하며, 수술을 받는다면
Table 1. Type of surgery according to tumor size
Operation group 1 (%) group 2 (%) group 3 (%) Total (%)
Lobectomy with CND(I)* 1 (2.1) 4 (4.0) 1 (1.4) 6 (2.8)
TT†with CND(B)§ 46 (97.9) 96 (95.0) 68 (97.1) 210 (96.3)
TT with MRND(I)‡ 0 1 (1.0) 1 (1.4) 2 (0.9)
*CND(I) = central node dissection, ipsilateral; †TT = total thyroidectomy; §CND(B) = central node dissection, bilateral; ‡MRND(I) = modified radical neck dissection, ipsilateral.
10년 후의 사망률은 10% 미만으로 보고될 정도로 좋은 예 후를 보여준다.(1) 유두상 갑상선암은 림프절로 전이를 잘 하는 것으로 알려져 있고 경부림프절로의 전이는 20∼50%
정도의 환자에서 발견되는 것으로 보고된다.(2) 이런 유두 상 갑상선암 중에서 특히 크기가 1 cm 이하인 경우를 WHO (the World Health Organization)에서 유두상 갑상선 미세암 (papillary thyroid microcarcinoma)으로 정의했고(3) 세침흡인 세포검사, 고해상 초음파 등의 진단기술의 발달로 유두상 갑상선 미세암의 조기진단이 늘어나고 있다.(4,5) 이러한 유 두상 갑상선 미세암 중에서 5 mm 이하의 크기를 갖는 종양 이 꽤 높은 빈도를 차지하고 있기에, 저자들은 대전성모병 원에서 유두상 갑상선암으로 한쪽 엽절제술 혹은 갑상선 전절제술을 중앙 경부림프절 절제술과 함께 시행 받은 환 자들을 종양의 크기에 따라 분류하여 각 군에서 임상병리 적 특성이 어떤지, 중앙 경부림프절 전이 유무와 임상병리 적 특성의 관계가 어떤지를 비교분석하고 이들에 대한 치 료방향을 생각해보고자 하였다.
방 법
2005년 6월부터 2007년 5월까지 대전성모병원에서 유두 상 갑상선암으로 갑상선 전절제 또는 한쪽 엽절제술을 중 앙 경부림프절 절제술과 함께 시행 받은 환자 218명을 대상 으로 했고 림프절을 얻지 못한 경우와 재발로 수술한 경우, 그리고 원격 전이의 소견을 갖는 환자는 제외시켰다. 이 환 자들에 대해 우선 종양의 크기가 10 mm 이하인 경우와 10 mm를 초과하는 군(group 3)으로 나누고 10 mm 이하는 다시 5 mm 이하(group 1)와 5 mm보다는 크며 10 mm를 넘지 않 는 경우(group 2)로 분류하여 중앙 경부림프절 전이의 유무 와 연령, 조직병리검사, 다발성 여부 등을 후향적으로 비교 분석 하였다. 통계처리는 Fisher's exact test 및 Chi-square test를 이용하였고 P-value가 0.05 미만인 경우를 통계학적으
로 의미가 있다고 하였다.
결 과
1) 성별 및 연령
성별은 남성이 7명(3.2%)이며 여성이 211명(96.8%)으로 여성이 많았고, 평균연령은 47.01세(18∼73)였으며 45세 이 상이 129명(59.2%), 45세 미만이 89명(40.8%)에 해당되었다.
연령과 성별 모두 종양의 크기나 림프절 전이와는 통계적 으로 유의한 상관관계는 없었다.
2) 수술 방식 및 림프절 절제
수술은 갑상선 전절제술과 중앙 경부림프절 절제술이 210예(96.3%)였고 전절제술 및 변형근치 경부림프절 곽청 술이 2예(0.9%), 그리고 일측엽 및 협부절제술과 동측의 중 앙 경부림프절 절제술이 6예(2.8%)였다(Table 1). 중앙 경부림 프절의 획득은 한 환자당 평균 11.42개(1∼35개)였다(Fig. 1).
3) 종양의 크기에 따른 임상 및 병리조직학적 특성
종양의 평균 크기는 10.41 mm였으며 5 mm 이하가 47예 (21.6%), 5 mm보다 크고 10 mm 이하인 경우가 101예 (46.3%), 10 mm보다 큰 경우가 70예(32.1%)로 유두상 갑상 선 미세암이 67.9%를 차지하고 있었다. 49예(22.5%)에서 갑 상선 외 침범이 있었으며 이는 원발종양의 크기와 통계적 으로 유의한 상관관계를 보였고(P<0.001), 림프절 전이의 경우도 종양의 크기와 통계적 유의성을 보였다(P<0.001).
피막침범은 89예(40.8%)로 종양의 크기와 통계적 유의성을 보였고(P<0.001), 혈관의 침범이 16예(7.3%)로 그 숫자는 많지 않았지만 종양의 크기와 통계적으로 유의한 상관관계 를 보였다(P<0.05). 다발성은 14예(6.4%), 양측성은 67예 (31.6%)로 종양 크기와 통계적 유의성은 관찰되지 않았다 (Table 2).
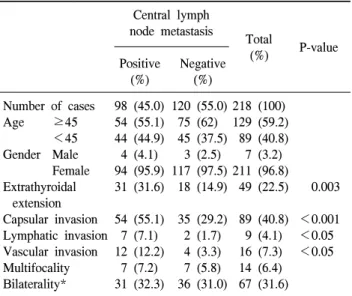
Table 3. Comparison of clinicopathologic characteristics between lymph node positive group and negative group
Central lymph node metastasis
Total
P-value (%)
Positive Negative
(%) (%)
Number of cases 98 (45.0) 120 (55.0) 218 (100) Age ≥45 54 (55.1) 75 (62) 129 (59.2)
<45 44 (44.9) 45 (37.5) 89 (40.8) Gender Male 4 (4.1) 3 (2.5) 7 (3.2)
Female 94 (95.9) 117 (97.5) 211 (96.8)
Extrathyroidal 31 (31.6) 18 (14.9) 49 (22.5) 0.003 extension
Capsular invasion 54 (55.1) 35 (29.2) 89 (40.8) <0.001 Lymphatic invasion 7 (7.1) 2 (1.7) 9 (4.1) <0.05 Vascular invasion 12 (12.2) 4 (3.3) 16 (7.3) <0.05 Multifocality 7 (7.2) 7 (5.8) 14 (6.4)
Bilaterality* 31 (32.3) 36 (31.0) 67 (31.6)
*The patient who received lobectomy was excluded.
Fig. 1. The number of acquired lymph nodes.
Table 2. Clinicopathological information for the 218 cases of papillary carcinoma according to tumor size
group 1 (%) group 2 (%) group 3 (%) Total (%) P-value
Number of cases 47 (21.6) 101 (46.3) 70 (32.1) 218
Age ≥45 27 (57.4) 59 (58.4) 43 (61.4) 129 (59.2)
<45 20 (42.6) 42 (41.6) 27 (38.6) 89 (40.8)
Gender Male 1 (2.1) 3 (3.0) 3 (4.3) 7 (3.2)
Female 46 (97.9) 98 (97.0) 67 (95.7) 211 (96.8)
Extrathyroidal extension 5 (10.6) 17 (16.8) 27 (38.6) 49 (22.5) <0.001
Lymph node metastasis 15 (31.9) 35 (34.7) 48 (68.6) 98 (45.0) <0.001
Capsular invasion 8 (17.0) 38 (37.6) 43 (61.4) 89 (40.8) <0.001
Lymphatic invasion 1 (2.1) 2 (2.0) 6 (8.6) 9 (4.1)
Vascular invasion 2 (4.3) 4 (4.0) 10 (14.3) 16 (7.3) <0.05
Multifocality 4 (8.5) 7 (6.9) 3 (4.3) 14 (6.4)
Bilaterality* 9 (19.6) 33 (34) 25 (36.2) 67 (31.6)
*The patient who received lobectomy was excluded.
4) 중앙 경부림프절 전이에 따른 임상 및 병리조직학적 특성
중앙 경부림프절 전이는 98명으로 전체환자의 45%에서 관찰되었고 이 중에서 갑상선 외 침범은 31예(31.6%), 피막 침범은 54예(55.1%), 림프관 침범이 7예(7.1%), 혈관 침범이 12예(12.2%)로 이들 모두 중앙 경부림프절 전이와 통계적 으로 유의한 상관관계(P<0.05)를 보였다(Table 3). 다발성 및 양측성은 림프절 전이군과 비전이군 간에 통계적 의의 를 보이지 않았다.
고 찰
갑상선암은 모든 악성종양 중에서 1% 정도에 해당되며 (6) 그 중 유두상 갑상선암이 80% 정도를 차지하고 있다.
유두상 갑상선암 중에서 크기가 1 cm 이하인 유두상 갑상 선 미세암은 임상적 증상의 발현 없이 우연히 발견되는 경
우가 많고, 최근 초음파, 세침흡인세포검사 등의 진단법의 발달로 진단율과 수술의 빈도가 증가하고 있다.(7,8) 유두상 갑상선암에서 예후에 영향을 주는 인자들은 아직 까지 확실히 밝혀지진 않았지만, Roti 등(9)은 종양의 크기 를 예후인자라 하였고 Hay 등(10)은 경부림프절 전이 및 수 술의 범위를, Baudin 등(11)은 수술의 범위 및 양측성을 위 험인자로 언급했다. Besic 등(8)은 유두상 갑상선 미세암에 서 종양의 크기가 6 mm를 넘거나 림프절 전이가 있는 경우 나쁜 예후를 보인다고 하였다. 본 연구에서도 림프절 전이 를 중요한 예후인자로 간주하여 분석한 결과, 이와 연관된 인자로 종양의 크기, 피막침범, 갑상선 외 조직침범, 림프- 혈관 침범(lymphovascular invasion)이 있었다. 림프-혈관 침 범의 경우에는 각각 림프절 전이와 관련이 있었지만 종양 의 크기와의 관련성은 혈관계 침범에서만 관찰되었다. 그 러나 림프-혈관 침범은 그 해당 환자수가 적어서 통계적 의 의가 떨어졌다. 다발성 및 양측성은 종양의 크기 및 림프절 전이와의 관계에서 통계적 의의를 보이지 못했다. 45세의 나이를 기준으로 병기가 바뀌게 되며 Hundahl 등(12)이 유 두상 갑상선암 환자의 나이가 45세 이하인 경우 생존율이 좋다고 보고한 바와 같이 본 연구에서도 연령을 45세를 기 준으로 나누어 여러 예후인자들과 비교해 보았다. 그러나 나이는 다른 인자들과의 연관성을 보이지 않았다. Lee 등 (13)은 종양의 크기는 림프절 전이와 통계적 의의가 없었고 연령, 성별, 피막 침범이 림프절 전이와 관련이 있다고 보고 했고, Lee 등(14)은 피막침범, 갑상선 외 조직침범, 림프절 전이를 국소 재발에 영향을 주는 위험요인으로 언급했으며 유두상 갑상선 미세암이라도 이러한 소견을 보이는 경우에 적극적인 치료가 필요하다 하였다.
본 연구에서는 종양의 크기에 따라 세 개의 그룹으로 분 류한 결과 유두상 갑상선 미세암이 절반을 넘는 수(67.9%) 를 차지했으며 이 중 5 mm 이하인 경우도 21%로 작지 않은 빈도를 차지했다. 최근 늘어나는 갑상선 종양 환자에서 조 기진단으로 인해 무증상이며 크기가 5 mm 이하인 종양이 발견되는 빈도가 높아지는 추세이므로 본 연구에서는 유두 상 갑상선암을 5 mm를 기준으로 분류하여 크기에 따른 분 석을 하고자 하였다. group 1, 2, 3에서 림프절 전이는 각각 15 (31.9%), 35 (34.7%), 48 (68.6%)명으로 크기가 증가할수 록 림프절 전이가 통계적으로 의미 있게 나타났으며 림프 절 전이 외에도 피막침범, 갑상선 외 침범이 통계적으로 관 련이 있었다. Park 등(7)도 종양의 크기와 관련된 인자로 피 막침범, 림프절 전이, 갑상선 외 침범, 양측성을 보고하였는
데, 본 연구와의 차이점은 종양의 크기가 커질수록 양측성 이 증가된다는 것이었다. 저자들은 5 mm 이하의 유두상 갑 상선 미세암의 분석에서 림프절 전이가 15명(31.9%), 갑상 선 외 조직침범 5명(10%), 그리고 8명(17%)에서 피막침범 이 있음을 관찰했다. 갑상선 외 조직침범이나 피막침범은 그렇게 많지 않았지만 비교적 높은 빈도를 차지했고, 특히 림프절 전이가 31.9%로서 문헌에서 보고되는 20∼50%와 비교하면 비교적 높은 수치라 할 수 있겠다. 그러므로 이러 한 작은 크기의 종양에서도 항상 림프절 전이의 가능성을 염두에 둬야 할 것으로 생각한다.
유두상 갑상선암이 림프절 전이를 잘 한다는 것은 이미 알려진 사실로서 20∼50%로 전이의 빈도가 보고되며, level VI인 중앙 경부림프절이 가장 흔히 전이되는 부위라고 알 려져 있다.(15) 중앙 경부림프절은 level VI의 림프절로 그 범위는 위쪽은 목뿔뼈(hyoid bone)이며 아래쪽은 복장패임 (sternal notch) 상부이고, 양쪽측면은 온목동맥(common car- otid artery)에 해당되어서 기도주위의 림프절, 델피안 림프 절(Delphian node), 그리고 갑상선주위의 림프절을 포함한 다.(16) 일부 문헌에서는 갑상선 전절제를 받은 10∼15%의 환자에서 경부림프절이 만져진다고 보고하였고(17) 국소적 재발의 75%가 경부림프절 전이로 나타난다고 보고하였 다.(18) Lundgren 등(19)은 림프절 전이는 사망률을 높이는 요인으로 보고하였다. 수술 전에 만져지는 림프절 또는 조 직검사로 전이가 확인된 림프절은 꼭 절제를 해야 하지만 그 외의 예방적 림프절 절제술은 필요 없다는 의견도 있 다.(20) 본 연구에서 기본적으로 중앙 경부림프절 절제술을 시행 받은 218명의 환자 가운데 중앙 경부림프절 전이가 관 찰된 경우는 98명으로 45%에 해당되었다. Park 등(7)은 260 명의 환자 중 55명(21.2%)에서, Lee 등(13)은 123명의 환자 중 55명(44.7%)에서 림프절 전이를 보고했고, Lee 등(14)은 26.9%의 림프절 전이를 보고하였다. 본 연구에서 림프절 전 이가 45%로 타 연구에 비하여 높은 빈도로 나타난 바, 저자 들은 갑상선 수술 시 중앙 경부림프절 절제를 기본적으로 같이 시행하는 것이 좋을 것으로 생각하는 바이다.
이러한 유두상 갑상선암은 높은 생존율을 보이기도 하지 만 원격전이나 재발을 보이는 경우도 있기 때문에 치료방 법에 있어서 여러 의견이 있고, 이를 밝히기 위한 전향적 연구가 없는 상태이다.(18) Ito 등(21)은 유두상 갑상선 미세 암의 경우 환자의 생존에 영향을 주지 않는 잠재성을 갖기 도 하므로 수술적 치료를 하지 않고 지켜볼 수도 있다고 하 였다. 수술적 치료로 갑상선 미세암의 경우 갑상선 전절제
보다는 한쪽 엽절제를 권유하는 경우도 있으며,(22) Grigsby 등(23)은 한쪽 엽절제술을 하고 이후 반대쪽 엽에 병변이 발견되어서 잔여 갑상선절제술(completion thyroidectomy) 및 방사성동위원소 치료를 시행하여도 처음부터 갑상선 전 절제를 한 경우와 비교하여 재발이나 생존율에 영향을 주 지 않는다고 하였다. Park 등(7)은 반대측의 재발을 줄이기 위해서 일측엽 절제술보다는 반대측엽을 포함한 아전절제 술 이상의 수술이 추천된다고 하였다. Grodski 등(18)은 다 른 부위보다 level VI인 중앙 경부림프절이 전이의 위험성 이 높기 때문에 갑상선 전절제와 함께 항상 동측의 중앙 경부림프절 절제를 시행할 것을 권하였다. Sywak 등(24)은 이런 중앙 경부림프절 절제를 갑상선 전절제와 함께 기본 적으로 시행할 경우 더욱 철저한 병변의 제거가 되어서 갑 상샘글로불린(thyroglobulin)의 수치를 더욱 낮출 수 있다고 하였고 Pereira 등(25)은 양측의 중앙 경부림프절 절제를 하 는 경우 재발을 낮출 수 있다고 보고했다. 중앙 경부림프절 절제를 권하는 또 다른 이유로는, 중앙 경부림프절로 재발 을 해서 다시 수술을 하는 경우, 중앙 경부림프절 절제술을 하는 과정에서 되돌이 후두신경(recurrent laryngeal nerve) 손 상 및 부갑상선 기능저하의 위험성이 높아진다는 것이 다.(26) 하지만 아직까진 유두상 갑상선암의 재발과 예후에 중앙경부림프절 절제술이 어떤 영양을 미치는지에 대한 전 향적, 무작위시험은 없는 실정이다.(27) 수술의 범위를 결정 하는 데 있어서도 Haigh 등(28)은 절제 범위가 환자의 생존 에 영향을 주지 못한다고 한 반면, Bilimoria 등(29)은 전절 제를 시행한 경우 재발이나 사망률이 감소되었다고 보고하 였다.
결 론
유두상 갑상선암에서 경부림프절 전이는 예후의 위험인 자로 알려져 있으며 이와 관련 있는 인자로 종양의 크기, 피막침범, 갑상선 외 침범, 림프-혈관 침범을 들 수 있는데 10 mm 이하인 유두상 갑상선 미세암, 특히 5 mm 이하의 작은 종양도 비교적 높은 빈도로 경부림프절 전이 및 피막 침범, 갑상선 외 조직침범을 보인다. 그러므로 저자들은 종 양의 크기가 작더라도 전절제 또는 일측 엽절제와 함께 반 드시 중앙 경부림프절 절제를 시행할 것을 권장하는 바이 다.
REFERENCES
1) Zuo H, Tang W, Yasuoka H, Nakamura Y, Ito Y, Miyauchi A, et al. A review of 227 cases of small papillary thyroid carcinoma. Eur J Surg Oncol 2007;33:370-5.
2) Cooper DS, Doherty GM, Haugen BR, Kloos RT, Lee SL, Mandel SJ, et al. Management guidelines for patients with thy- roid nodules and differentiated thyroid cancer. Thyroid 2006;
16:109-42.
3) Hedinger C, Williams ED, Sobin LH. The WHO histological classification of thyroid tumors: a commentary on the second edition. Cancer 1989;63:908-11.
4) Chow SM, Law SC, Chan JK, Au SK, Yau S, Lau WH.
Papillary microcarcinoma of the thyroid-Prognostic sig- nificance of lymph node metastasis and multifocality. Cancer 2003;98:31-40.
5) Renshaw AA. Papillary carcinoma of the thyroid <or=1.0 cm:
rarely incidental or occult any more. Cancer 2005;105:217-9.
6) Schlumberger MJ. Papillary and follicular thyroid carcinoma.
N Engl J Med 1998;338:297-306.
7) Park HL, Kwak JY, Kang SS, Kim DY, Kang HG, Shim JY, et al. The analysis of tumor aggressiveness according to tumor size in occult papillary thyroid carcinoma. J Korean Surg Soc 2007;73:470-75.
8) Besic N, Pilko G, Petric R, Hocevar M, Zgajnar J. Papillary thyroid microcarcinoma: prognostic factors and treatment. J Surg Oncol 2008;97:221-5.
9) Roti E, Rossi R, Trasforini G, Bertelli F, Ambrosio MR, Busutti L, et al. Clinical and histological characteristics of papillary thyroid microcarcinoma: results of a retrospective study in 243 patients. J Clin Endocrinol Metab 2006;91:
2171-8.
10) Hay ID, Grant CS, van Heerden JA, Goellner JR, Ebersold JR, Bergstralh EJ. Papillary thyroid microcarcinoma: a study of 535 cases observed in a 50-year period. Surgery 1992;
112:1139-46.
11) Baudin E, Travagli JP, Ropers J, Mancusi F, Bruno-Bossio G, Caillou B, et al. Microcarcinoma of the thyroid gland: the Gustave-Roussy Institute experience. Cancer 1998;83:553-9.
12) Hundahl SA, Fleming ID, Fremgen AM, Menck HR. A National Cancer Data Base report on 53,856 cases of thyroid carcinoma treated in the U.S., 1985-1995 [see commetns].
Cancer 1998;83:2638-48.
13) Lee SJ, Park BS, Kim JS, Park JS. Analyses of cervical lymph node metastases from papillary thyroid cancer. J Korean Surg Soc 2003;64:115-20.
14) Lee JD, Yun JS, Nam KH, Chung WY, Soh EY, Park CS.
Papillary thyroid microcarcinoma: clinicopathologic character- istics and treatment strategy. J Korean Surg Soc 2007;72:
276-82.
15) Machens A, Holzhausen HJ, Dralle H. Skip metastases in thy- roid cancer leaping the central lymph node compartment. Arch Surg 2004;139:43-5.
16) Robbins KT, Medina JE, Wolfe GT, Levine PA, Sessions RB, Pruet CW. Standardizing neck dissection terminology. Official report of the Academy's Committee for Head and Neck Surgery and Oncology. Arch Otolaryngol Head Neck Surg 1991;117:601-5.
17) McConahey WM, Hay ID, Woolner LB, van Heerden JA, Taylor WF. Papillary thyroid cancer treated at the Mayo Clinic, 1946 through 1970: initial manifestations, pathologic findings, therapy, and outcome. Mayo Clin Proc 1986;61:
978-96.
18) Grodski S, Cornford L, Sywak M, Sidhu S, Delbridge L.
Routine level VI lymph node dissection for papillary thyroid cancer: surgical technique. ANZ J Surg 2007;77:203-8.
19) Lundgren CI, Hall P, Dickman PW, Zedenius J. Clinically sig- nificant prognostic factors for differentiated thyroid carcinoma:
a population-based, nested case-control study. Cancer 2006;
106:524-31.
20) Stulak JM, Grant CS, Farley DR, Thompson GB, van Heerden JA, Hay ID, et al. Value of preoperative ultrasonography in the surgical management of initial and reoperative papillary thyroid cancer. Arch Surg 2006;141:489-94.
21) Ito Y, Uruno T, Nakano K, Takamura Y, Miya A, Kobayashi K, et al. An observation trial without surgical treatment in pa- tients with papillary microcarcinoma of the thyroid. Thyroid 2003;13:381-7.
22) Elaraj DM, Clark OH. Changing management in patients with
papillary thyroid cancer. Curr Treat Options Oncol 2007;8:
305-13.
23) Grigsby PW, Reddy RM, Moley JF, Hall BL. Contralateral papillary thyroid cancer at completion thyroidectomy has no impact on recurrence or survival after radioiodine treatment.
Surgery 2006;140:1043-7.
24) Sywak M, Cornford L, Roach P, Stalberg P, Sidhu S, Delbridge L. Routine ipsilateral level VI lymphadenectomy re- duces postoperative thyroglobulin levels in papillary thyroid cancer. Surgery 2006;140:1000-5.
25) Pereira JA, Jimeno J, Miquel J, Iglesias M, Munne A, Sancho JJ, et al. Nodal yield, morbidity, and recurrence after central neck dissection for papillary thyroid carcinoma. Surgery 2005;138:1095-100.
26) Ito Y, Higashiyama T, Takamura Y, Miya A, Kobayashi K, Matsuzuka F, et al. Risk factors for recurrence to the lymph node in papillary thyroid carcinoma patients without pre- operatively detectable lateral node metastasis: validity of pro- phylactic modified radical neck dissection. World J Surg 2007;31:2085-91.
27) White ML, Gauger PG, Doherty GM. Central lymph node dis- section in differentiated thyroid cancer. World J Surg 2007;31:895-904.
28) Haigh PI, Urbach DR, Rotstein LE. Extent of thyroidectomy is not a major determinant of survival in low- or high-risk pap- illary thyroid cancer. Ann Surg Oncol 2005;12:81-9.
29) Bilimoria KY, Bentrem DJ, Ko CY, Stewart AK, Winchester DP, Talamonti MS, et al. Extent of surgery affects survival for papillary thyroid cancer. Ann Surg 2007;246:375-81.