관상동맥 중재술후 발생한 재발성 심낭 압전 동아대학교병원 순환기내과
5
0
0
전체 글
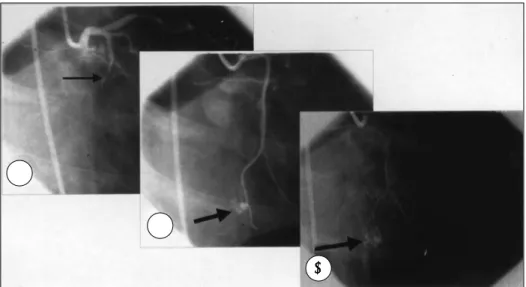
(2) 고 유도철심을 원위부까지 위치시키려고 여러번 시도하. 1예를 보고하는 바이다.. 였다. 유도철심을 원위부에 위치시킨 후 확인한 조영술에. 증. 례. 서 조영제 염색이 관찰되었다(Fig. 1). 더 이상의 시술을 중단하고 관찰하였으나 혈압과 맥박은 변화 없이 안정되. 내원 1년전에 관상동맥 스텐트 시술을 받았던 64세 남. 었고 심초음파검사에서 심낭삼출액의 저류는 관찰되지 않. 자 환자가 내원 1주전부터 전흉부 통증이 생겨 내원하였. 아서 protamine 30 mg 정주하고 aspirin과 ticlopidine. 다. 관상동맥 조영술에서 스텐트 재협착은 없었고 좌회선. 의 복용을 중지시킨 후 병실에서 관찰하였다. 시술 4시. 동맥에 새로운 완전협착이 관찰되었다. 환자는 관상동맥. 간후 혈압 90/50 mmHg까지 하강하며 빈맥, 흉통과 호. 조영술 3일전부터 aspirin(250 mg po Qd)과 ticlopidine. 흡곤란이 발생하였고 심초음파검사에서 소량의 심낭삼출. (250 mg po bid)를 복용하고 있었고, 중재술전 heparin. 액이 관찰되었다(Fig. 2). 임박 심낭 압전이 의심되어 우. 10000 IU를 정맥 투여하였고 활성응고시간(ACT)은. 심방압과 대퇴동맥압을 측정하면서 겸상돌기하 접근으로. 312초로 측정되었다.. 심낭천자를 하여 심낭내압을 측정하고 180 ml를 배액한. 근위부 좌회선동맥의 완전협착 병변에 대한 고식적 풍. 후 혈압 120/80 mmHg로 안정되었다(Fig. 3, 4 and 5).. 선확장술을 시행한 후 원위부에 대한 풍선확장을 계획하. 심낭천자 다음날 호흡시 흉통을 호소하여 관상동맥 조영. A. B C Fig. 1. After successful balloon angioplasty of the total occlusion of proximal left circumflex artery(LCx)(A), persistent contrast agent staining(B & C) was developed at distal LCx after guidewire manipulation.. A. B. Fig. 2. Small amount of pericardial effusion(arrows) was noted 4 hour after coronary intervention. A:modified parasternal long axis view, B:parasternal short axis view.. 2052. Korean Circulation J 1998;28(12):2051-2055.
(3) Fig. 3. Femoral artery pressure change before(A) and after(B) pericardiocentesis.. Fig. 4. Right atrial pressure(RAP) change before(A) and after(B) pericardiocentesis. A:RAP was increased and x descent(arrow) was prominent, B:RAP was in normal range but prominent x descent was still remained.. Fig. 5. Right atrial pressure(RAP) and intrapericardial pressure(IPP) change before(A) and after(B) pericardiocentesis. A:RAP and IPP were increased and x descent(arrow) was prominent, B:RAP was in normal range, but increased IPP and prominent x descent were still remained.. 2053.
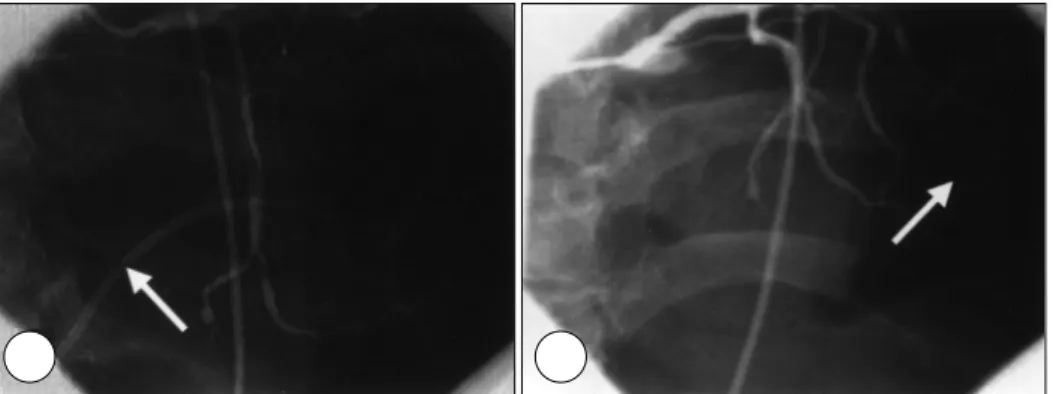
(4) A. B. Fig. 6. Follow-up coronary angiograms of one day after the first pericardiocentesis(A) and five days after the second pericardiocentesis(B). A:no leakage of contrast agent warranted the removal of drainage catheter (arrow). B:After the removal of the first drainage catheter, cardiac tamponade was recurred and second pericardiocentesis (arrow) was done.. 술을 다시 시행하여 심낭내로의 조영제의 누출(leakage). 관상동맥 천공 및 심낭 압전의 예방과 치료를 위한 권고. 이 없음을 확인하고(Fig. 6-A), 심낭천자후 16시간만. 유도철심의 조작과 연관하여 완전 폐쇄병변, 혈전이 포. 에 배액 도자를 제거하고 침상 안정을 권고하였다. 침상. 함된 병변 등에서는 유도철심을 무리하게 진행시켜 내. 안정 18시간후 다시 흉통을 호소하였고 19시간만에 수. 막하로 통과하거나 혈관의 박리 또는 천공이 생기지 않. 축기 혈압이 60 mmHg로 하강하였다. 재발성 심낭 삼출. 도록 주여하여야 겠다.. 을 확인하고 심낭 천자를 다시 시행하여 200 ml를 배액. Ajluni 등6)은 불량한 병변 특징(만성 완전 폐쇄, 분지. 한 후 안정되었다. 5일간에 걸쳐 240 ml가 더 배액되었. 병변, 심한 굴곡 병변)의 인지와 중재술 기구의 크기에 기. 고 관상동맥 조영술에서 더 이상의 누출이 없음을 확인. 초하여 다음과 같이 권고하였다. 첫째, 이러한 불량한 병변. 하고(Fig. 6-B), 배액 도자를 제거하였다. 이후 더 이상. 특징이 있는 경우 풍선확장술은 balloonartery ratio를 ~. 의 누출은 없었고 안정된 상태로 퇴원하였다.. 1.0으로, TEC와 ELCA은 device/artery ratio를 ~0.5~ 0.6으로 시작하여야 한다. 추가적인 확장이 필요한 경우는. 고. 찰. 큰 기구(D/A ratio >0.8)의 사용보다는 보조적인 PTCA (B/A ratio ~1.0)를 고려하여야 한다. 둘째, 관상동맥 천. 새로운 중재술 기구들은 경피적 혈관성형술의 기회를. 공 발생시 대부분에서 즉각적인 repeat PTCA(with or. 확장시킬 수 있지만 조직의 절제나 제거에 의한 관상동. without perfusion balloon)를 하여야 한다. 왜냐하면 이. 10-13). 또한 심낭 압. 러한 시술은 합리적이며 2/3의 경우에서 응급 관상동맥. 전은 급성 심근경색증에 대한 혈전용해요법후나 중재술. 우회로술의 필요를 피할 수 있었다고 하였다. 셋째, 유의한. 동안 예방적으로 삽입한 임시형 조율도자에 의한 우심실. 박리가 혈관조영에서 보이면 중재술 기구(laser, athere-. 맥의 천공 위험을 증가시킬 수 있다.. 14). 천공 으로도 일어날 수 있다. 그러나 표준 항응고제재. ctomy)의 사용은 혈관 벽의 integrity를 변화시켰기 때문. 의 사용하에서 관상동맥 파열이 심낭 압전을 초래하는 경. 에 지연 천공의 가능성을 의심해야 한다고 하였다. 이러한. 7). 우는 드물다고 알려져 있다.. 본 증례는 강력한 항혈소판제제(aspirin+ticlopidine). 경우에 혈역학적 허탈이 발생하면 급성 폐쇄 또는 천공과 심낭 압전을 고려하여야 한다고 하였다.. 를 미리 사용하는 최근의 관상동맥 중재술 전략하에서는. 중재술동안 조율도자의 예방적 삽입은 심낭 압전의 위. 유도철심에 의한 조영제의 단순한 염색 또는 누출은 비. 험이 있기 때문에 무분별한 사용을 자제하여야겠으며 Go-. 록 heparin 정주를 중단하고 protamine을 정주하더라. ldbaum 등14)은 심낭 압전의 위험을 피하기 위해 standby. 도 심낭삼출과 압전의 한 원인이 될 수 있으며 배액 도자. pacing의 세가지 방법을 권유하였다. 첫째, 임시형 조율. 의 제거때는 항혈소판제제의 지연 효과를 고려하여야 함. 도자를 하대정맥이나 우심방내에 두었다가 필요시에만. 을 보여준다.. 우심실로 진입시킬수 있으며, 둘째, Meier 등15)의 권유. 2054. Korean Circulation J 1998;28(12):2051-2055.
(5) 대로 혈관성형술 유도철심으로서 조율을 준비하여 우심도 자술을 전혀 하지 않을 수도 있으며, 셋째, 풍선이 달린. REFERENCES. 조율도자(balloon-tipped pacing catheter)를 주페동. 1) Kimbris D, Iskandrian AS, Goel I, Bemis CE, Gehl L,. 맥에 두고서 우심실유출로를 조율하는 방법을 제시하였다. 최근 스텐트 시술후는 풍선확장술때와는 달리 고압력 확장을 하는 경우가 많으며 혈소판 IIb/IIIa 수용체 차단. 2). 제를 포함한 강력한 항혈소판제제를 사용하므로 스텐 트 시술후 양호한 혈관조영 결과후에도 뚜렷한 원인없. 3). 이 혈역학적으로 불안정한 경우 심낭 압전의 발생 가능 성을 고려하여야겠다.7) 추정되는 원인으로 Bottner 등7). 4). 은 유도철심에 의한 관상동맥 천공은 혈관조영에 잘 나 타나지 않을 수 있으며 그 외 여러개의 스텐트 사용, 고 압력 확장, 임상적으로 발견되지 않았던 심낭 질환을 지. 5). 적하였다. 심낭 압전이 인지된 후 혈소판 IIb/IIIa 수용체 차단제의 주입을 중단하고 protamine으로 heparin의 효과를 없앤 후에도 지속적인 출혈이 있으면 혈소판 수. 6). 혈을 하여야 한다. 이는 출혈이 aspirin에 의한 혈소판 사 이클로옥시나제의 억제의 결과일 수도 있으나 혈소판 Iib/. 7). IIIa 수용체 차단제에 의한 혈소판 응집의 억제가 더 중 요한 원인이기 때문이다. EPILOG 연구16)는 심각한 출 혈성 합병증을 줄이기 위해서는 혈소판 IIb/IIIa 수용체. 8). 차단제의 사용과 연관하여서는 저용량(70 U/kg bolus) heparin을 사용하는 전략이 중요함을 보여주었다.. 요. 약. 9) 10) 11). 관상동맥 천공은 드물지만 경피적 관상동맥 중재술의 가 장 심각한 합병증의 하나이며 표준 항응고제제의 사용하에 서 심낭 압전을 초래하는 경우는 드물다고 알려져 있다. 그러나 최근 관상동맥 천공의 증거가 없더라도 고용량의 heparin 정주하에서 풍선확장술후와 혈소판 IIb/IIIa 수용. 12) 13). 체 차단제를 포함한 강력한 항혈소판제제의 사용하에서 스 텐트 시술후 자발적인 심낭 압전의 발생이 보고되고 있다.. 14). 저자들은 강력한 항응고제제와 항혈소판제제의 사용하 에서 관상동맥 중재술동안 유도철심의 조작후에 발생한 조영제 염색이 심낭 압전으로 진행하였고 심낭 천자후 조. 15). 기에 재발하였던 1예를 보고하는 바이다. 16). 중심 단어:심낭 압전・관상동맥 중재술・항혈소판 치료.. Owens J, et al. Transluminal coronary angioplasty complicated by coronary artery perforation. Cathet Cardiovasc Diagn 1982;8:481-7. Cowley MJ, Dorras G, Kelsey SF, Van Radon M, Detre KM. Acute coronary events associated with percutaneous transluminal coronary angioplasty. Am J Cardiol 1984; 53:12c-6c. Saffitz JE, Rose TE, Roberts WC. Coronary artery rupture during coronary angioplasty. Am J Cardiol 1983;51: 902-4. Topaz O, Cowley MJ, Vetrovec GW. Coronary perforation during angioplasty: angiographic detection and demonstration of complete healing. Cathet Cardiovasc Diagn 1992;27:284-8. Chou TM, Amidon TM, Ports TA. Contained rupture following percutaneous transluminal coronary angioplasty: Long-term outcome. Cathet Cardiovasc Diagn 1993;28: 152-4. Ajluni SC, Glazier S, Blankenship L, O’neill WW, Saflan RD. Perforation after percutaneous coronary interventions: clinical, angiographic, and therapeutic observations. Cathet Cardiovasc Diagn 1994;32:206-12. Bottner RK, Hardigan KR. Cardiac tamponade following stent implantation with adjuvant platelet IIb/IIIa receptor inhibitor administration. Cathet Cardiovasc Diagn 1997; 40:380-2. Meier B. Benign coronary perforation during percutaneous transluminal coronary angioplasty. Br Heart J 1985; 54:33-5. Howlett JG, Teskey RJ, O’neill BJ. Spontaneous pericardial tamponade during PTCA. Can J Cardiol 1995;11:927-30. Bittl JA, Ryan TI, Keaney JF, et al. Coronary artery perforation during excimer laser coronary angioplasty. J Am Coll Cardiol 1993;21:1158-65. Phillips HR, Sketch MH Jr, Meany TB, et al. Coronary transluminal extraction endarterectomy: a multicenter experience. Circulation 1991;84(Suppl II):II-82. Velter J, Robertson G, Selmon M, et al. Perforation with directional coronary atherectomy. J Am Coll Cardiol 1992; 19:76A. Ellis SG, Arnold AZ, Raymond RE, et al. Increased coronary perforation in the new device era: incidence, classification, management and outcome. Circulation 1992;86 (Suppl I):I-787. Goldbaum TS, Jacob AS, Smith DF, Pichard A, Lindsay J Jr. Cardiac tamponade following percutaneous transluminal coronary angioplasty: four case reports. Cathet Cardiovasc Diagn 1985;11:413-6. Meier B, Rutishauser W. Coronary pacing during percutaneous transluminal coronary angioplasty. Circulation 1985; 71:557-61. Ferguson JJ. EPILOG and CAPTURE trials halted because of positive interim results. Circulation 1996;93:637.. 2055.
(6)
수치

관련 문서
Argentine randomized trial of percutaneous transluminal coronary angioplasty versus coronary artery bypass surgery in multivessel disease (ERACI): in-hospital results and
Results of percutaneous transluminal coronary angioplasty in patients ≥65 years of age (from 1985-1986 national heart, lung, and blood institute’s coron- ary angioplasty).
Results of coronary angioplasty of chronic total occlusion (the National Heart, Lung, and Blood Institute 1985-1986. Percutaneous Transluminal Angioplasty Registry). Risk
Clinical experience with primary percutaneous transluminal coronary angioplasty compared with alteplase (recumbinant tissue-type plasminogen activator) in patients with
We report a case of percutaneous transluminal coronary angioplasty PTCA and stent implantation to the left anterior descending artery LAD and left circumflex artery LCX in a
1) Thornton MA, Gruentzig AR, Hollman J, King SB III, Douglas JS. Coumadin and aspirin in prevention of recurrence after transluminal coronary angioplasty : A randomized study. 2)
유도도관을 깊게 삽관시키는 기법(deep intubat- ion technique)은 19명(18%)에서 시도되었다. Percutaneous radial artery approach for cor- onary angiography. Transradial
The effect of structured informational supportive nursing on stress and pain reduction in patient undergoing percutaneous transluminal coronary
