INTRODUCTION
Although the pathogenesis of myopic macular hole with retinal detachment is not fully understood,1several factors have been postulated as contributing to the development of the disease. The atrophy of the retinal pigment epithelium and choroids, posterior staphyloma and tangential macu- lar traction were thought to be causative factors of retinal detachment caused by a macular hole in the highly myopic eye.2,3
Many surgical techniques have been tried for the treatment of retinal detachment caused by macular hole in the high myopic eye.4,5 Since Gonvers reported a technique that involved vitrectomy and
gas tamponade in 1982, vitrectomy has become the preferred technique.4,6 Other modified methods have been introduced, including complete epiretinal membrane separation,3 vitrectomy with silicone oil tamponade,8,9 simplified method with subretinal fluid drainage and gas tamponade10and macular buckling.6,7
In this study, we evaluated whether vitrectomy with perifoveal internal limiting membrane (ILM) removal improves the anatomical outcome in myopic macular hole with retinal detachment.
MATERIALS AND METHODS
Nineteen eyes in 19 consecutive patients with high myopia and retinal detachment caused by mac- ular hole who visited the retina clinic of Samsung Seoul Hospital between November 2000 and December 2002 were studied retrospectively.
Inclusion criteria were myopia higher than -5.0 Vol. 18:141-147, 2004
Effect of Internal Limiting Membrane Removal in Treatment of Retinal Detachment Caused by Myopic Macular Hole
Heeyoon Cho, MD, Anho Choi, MD, Se Woong Kang, MD
Department of Ophthalmology, College of Medicine, Sungkyunkwan University, Seoul, Korea The purpose of this study was to evaluate the anatomical outcomes of vitrectomy with internal limiting membrane removal in highly myopic eyes with retinal detach- ment caused by a macular hole. Nineteen, consecutive, highly myopic eyes with full thickness macular hole with retinal detachment were treated by vitrectomy with internal limiting membrane removal, endolaser photocoagulation on the center of the hole and fluid gas exchange. In five eyes with other peripheral breaks, scleral buckling (3 cases), encircling (1 case) and barrier laser (1 case) were combined. In 15 eyes (79.0%) the macular hole was closed after the initial surgery. In 4 eyes (21%) the macular hole was reopened, but these were successfully treated with fluid gas exchange (1 case) or macular buckling (3 cases). The visual acuity was improved in 15 eyes (79.0%). In conclusion, these results suggest that the removal of the peri- foveal internal limiting membrane may be an important adjuvant in the treatment of the myopic macular hole with retinal detachment.
Key words: high myopia, internal limiting membrane, macular hole, retinal detachment
Reprint requests to Se Woong Kang, MD, Department of Ophthalmology, Sungkyunkwan University, Samsung Medical Center, 50 Ilwon-dong, Kangnam-ku, Seoul 135- 710, Korea.
diopters (D) and myopic change of the fundus.
Myopic change of fundus indicates the fundus with tigroid feature in the myopic eye or with chorioreti- nal atrophy. Eyes with a history of ocular trauma were excluded from study.
There were two males and 17 females, ranging in age from 41 to 82 years (mean age : 60.68 9.50 years). The spherical equivalent ranged from -5.25 D to -19.5 D (mean spherical equivalent : -10.68 4.72 D), excluding five cases in which the refractive error could not be checked due to total retinal detachment or cataract. A posterior staphyloma was present in 12 cases (63.1%) and peripheral tear(s) was (were) present in the detached retina in 5 cases (26.3%).
All patients were operated on by one surgeon (S.W. K.) A three-port standard pars plana vitrecto- my was performed in all eyes. Cataract extraction
was performed in three eyes, and intraocular lens (IOL) implantation was combined in two eyes. In the five eyes with peripheral tears, the encircling (1 case), scleral buckling (3 cases) or barrier laser (1 case) were combined. In all 19 eyes, perifoveal ILM removal was performed after indocyanine green dye staining. ILM was peeled in the curvilinear fashion by ILM forceps. The diameter of the ILM removal area was about 2 discs diameters. All excised speci- mens were submitted for processing for transmis- sion electron microscopy (TEM). Subretinal fluid was drained through the center of the macular hole.
Either 25% sulfur hexafluoride or 14% perfluoro- propane was injected after fluid-air exchange. All patients were instructed to remain in prone position for 2 weeks.
Fig. 1. Pre-operative (A,B) and post-operative (C,D) optical coherence tomographic(OCT) and fundus photog- raphy findings (case 10). Retinal detachment caused by macular hole was developed (A,B). Spherical equiva- lent was -5.875 diopters and there was no other break. After vitrectomy, internal limiting membrane peeling and fluid-gas exchange, the retina was reattached (C). OCT image confirms the reattachment of the retina and closure of the macular hole (D).
RESULTS
The mean postoperative follow-up time was 20.58 7.24 months (range : 12 to 35). The post- operative results are shown in Table 1. In 13 of the 19 eyes, the macular hole was closed and the retina was reattached with one operation. The hole was closed with one operation in 15 eyes (79.0%). In six eyes, retinal detachment recurred during the postop- erative follow up period due to reopened macular hole in four eyes and new or missed peripheral reti- nal break in two eyes. In one case of reopened mac- ular hole (#8), fluid-gas exchange with none-expan- sile sulfur hexafluoride and subsequent laser photo- coagulation on the edge of the macular hole was performed on an out-patient basis. In three cases of reopened macular hole (#4, 11, 16) with prominent posterior staphyloma, macular buckling was per- formed with silicone sponge (Mira type 506). After these procedures, the reopened macular hole was successfully closed and the retina was flattened.
Encircling was applied in two cases with recurred retinal detachment with peripheral retinal breaks (#6, 7) to reattach the retina. In all 19 cases, the macular hole was sealed and the retina was reat- tached after including the second operation. Macular hole closure was confirmed not only by slit lamp examination with +90 D lens but also by optical
coherence tomography (Fig. 1).
The best-corrected visual acuity was improved in 11 eyes (57.9%), unchanged in seven (36.8%), and deteriorated in one (5.3%). Preoperative mean visu- al acuity was 0.05 and postoperative mean visual acuity was 0.15. Cataracts developed in two eyes during the follow-up period and cataract surgery was performed.
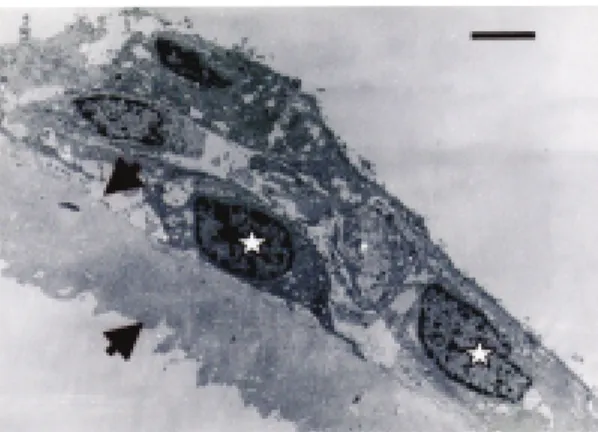
TEM photograph of the excised specimen revealed that ILM was present in all specimens (Fig.
2). Hyperplastic retinal pigment epithelial cells and/or fibrous astrocytes attached on the vitreous side of ILM were almost universally found.
DISCUSSION
The onset mechanism of retinal detachment caused by macular hole in the highly myopic eye is not fully understood.1 The theory that idiopathic senile macular hole is developed by traction caused by focal shrinkage of the vitreous cortex in the foveal area has been accepted so far.11It could be assumed that the onset mechanism of macular hole in high myopia might be similar to that of idiopathic macular hole.12However, some differences exist between the macular holes of high myopia and those of the senile idiopathic type. Development of retinal detachment is relatively common in myopic macular holes in contrast to idiopathic macular holes.
Several factors have been postulated as contributing to the development of retinal detachment in myopic macular hole. The atrophy of the retinal pigment epithelium and choroids, posterior staphyloma, and tangential vitreous traction were thought to be important factors of this disease.2,3The active trans- port of ions across the retinal pigment epithelium and oncotic pressure from the protein-rich choroidal fluid are the major forces which draw fluid out of the subretinal space.13The atrophy of the retinal pigment epithelium and choroids would eventually weaken the adherence of the sensory retina to the retinal pigment epithelium. The myopic chorioreti- nal change may represent a spectrum evolving from tigroid to the widespread diffuse atrophy. The myopic eye with tigroid fundus provides a base con- ducive to the development of retinal detachment, and severe chorioretinal atrophy further increases the incidence.12
Fig. 2. Internal limiting membrane removed from the retina surrounding the macular hole. Notice the cells, which shows fibrous astrocytes (asterisk) attached to the inner surface of the internal limiting membrane (arrow). (TEM, bar 8µm) (×1000)
Table 1.Preoperative clinical characteristics and postoperative results CaseRefractionAxial PosteriorPeripheralExtentBest correctedRecurred RDReopeningSecondFollow No(SE)lengthstaphylomatearsof RDvisual acuity(postop date)of MHsurgeryup (mm)Pre-opPost-op(months) 1-5.25**-+Total0.030.05---27 2-7.62529.05-+6DD0.10.03---26 3-19.526.78+-5DD0.030.15---29 4-19.528.30+-5DD0.050.2+ (14 months)+PEBP29 5***+-Total0.010.15---35 6-10.0**+-Half totalHM0.2+ (10)-E30 7-6.2527.24-+Half total0.10.15+ (40)-E27 8-8.026.6+-5DD0.10.1+ (70)+FGE23 9*25.28-+TotalHM0.3---18 10-5.875*++Total0.030.1---1811 *29.88+-5DD0.050.07+ (30)+PEBP1712 -9.75**+-TotalHMFC 30cm---1613 -10.028.70+-6DD0.060.1---1314 -8.62530.83+-Half total0.060.06---1215 -9.2527.54+-Half total0.070.15---1416 -15.2531.60+-3DD0.10.3+ (40)+PEBP1617 -14.7530.53--Total0.040.02---1318 *30.99--Total0.050.2---1319 *26.75--4DD0.060.15---15 *: Refraction could not be checked due to total retinal detachment or cataract. **: No data, SE: spherical equivalent, DD: disc diameter, RD: retinal detach- ment, MH: macular hole, PEBP: posterior episcleral buckling procedure, FGE: fluid gas exchange.
Akiba et al revealed that retinoschisis and retinal detachment often develop in highly myopic eyes without macular holes by optical coherence tomo- graphic study.14It could be thought that a macular hole evokes retinal detachment more easily, and adversely, that a macular hole may form as a result of preexisting retinoschisis or retinal detachment.15 They found that extensive retinal detachment devel- oped in 95% of eyes with macular holes and myopia (over -6D) with a posterior staphyloma, compared to in only 7% of eyes without posterior staphyloma.
They concluded that posterior staphyloma rather than anteroposterior vitreomacular traction may contribute to the development of retinal detachment associated with a macular hole in severely myopic eyes.16The ectatic sclera in high myopia is associat- ed with a number of abnormalities such as extreme thinning, absent interweaving of the fiber bundles, and their dissociation.17The sclera of the posterior pole is stretched in the eyes with posterior staphylo- ma, resulting in a disproportion among sclera, choroid and retina. In this situation, due to “inverse traction”, the sensory retina becomes easily detached from the pigment epithelium.4,12
Although the tangential and anteroposterior vitre- ous traction were thought to be eliminated through the removal of perifoveal ILM, redetachment via reopening of the myopic macular hole was still sub- stantial incidence (21%) in our study. This may sug- gest the role of the posterior staphyloma.
Ishida et al investigated the ultrastructure of sur- gically removed epiretinal membrane.1The epireti- nal membrane consists of cortical vitreous and vari- ous cellular components. The active synthesis of new collagen aggregates regulated by fibrous astro- cytes in a synchronized cellular network, with com- munication by gap junctions and active cell-matrix interactions, may lead to a diffusely condensed pos- terior cortical vitreous. This cell-mediated remodel- ing of the collagen matrix of the posterior cortical vitreous may generate tangential traction and play an important role in the pathogenesis of myopic macular hole with retinal detachment.1 Stirpe et al reported that tangential traction from the epiretinal tissue was the apparent cause of recurrent retinal detachment in highly myopic eyes with macular hole.18 In this study, TEM photographs similarly showed that fibrous astrocytes were adhered to
removed ILM(Fig. 2).
In 2000, Gonvers, based on his experience of treatment for retinal detachment owing to myopic macular hole, reported that the choice of the surgical technique is best based on (1) the presence or absence of a posterior staphyloma and/or (2) chori- oretinal degenerations and on (3) the axial length of the globe.19A recent report by Ripandelli et al indi- cates that the vitreous anatomy such as posterior vit- reous detachment or posterior vitreous schisis should be considered in deciding the surgical approach.20
The role of the posterior vitreous detachment in the development of retinal detachment in myopic eyes with macular hole is controversial. Morita et al suggested that posterior vitreous detachment does not act as substantial causative factor in producing retinal detachment from macular hole.12 On the other hand, Akiba et al reported that extensive reti- nal detachment developed in 89% of cases with complete posterior vitreous detachment and in 31%
of cases without posterior vitreous detachment, and that the difference was significant.16
Many surgical techniques have been tried for the treatment of retinal detachment caused by macular hole in the highly myopic eye.4,5Macular buckling and a method of retinopexy, with cryotherapy, diathermy, or photocoagulation macular diathermy, were used for treatment of the disease. The chief disadvantage of these techniques is the difficulty of approaching the macula due to the buckling and per- manent destruction of the macular area.4 In 1982, Gonvers reported a new surgical technique for the treatment of retinal detachment due to myopic mac- ular hole. This approach was based on the concept that vitreous traction plays a major role in the devel- opment of many of these detachments.4 In 1986, Miyake described a simplified method - subretinal fluid drainage and gas tamponade - of treating reti- nal detachment with macular hole. The advantages of this procedure are that it is easy, safe and requires no sophisticated instruments.10 Eyes with low myopia (<-10.0D) and without posterior staphyloma are best treated with vitrectomy and air/gas injection alone, whereas eyes with more marked (>-15.0D) and extensive atrophy and/or posterior staphyloma are best treated with vitrectomy, laser photocoagula- tion of the macular hole rim under perfluorocarbon
liquid, and a temporary tamponade with silicone oil.
Against the effect of posterior staphyloma, macular buckling has been tried. However, it was not easy to gain access to the macular area without vitrectomy, so a special exoplant and the surgical technique of posterior episcleral buckling were introduced.6,7 In our four cases, reopening of macular hole with reti- nal detachment was developed after initial surgery.
In three of these cases, macular buckling was per- formed to release the reverse traction due to severe posterior staphyloma. In the other case, retinal reat- tachment was achieved by additional intravitreal gas injection followed by photocoagulation to the mar- gin of the macular hole.
Tangential macular traction may play an impor- tant role in macular hole formation and subsequent retinal detachment.3,21In this regard, it is important to perform epiretinal membrane separation as com- pletely as possible.3,21Recently, Kadonosono et al revealed the contraction of myofibroblasts on the ILM surface around the macular hole in highly myopic eyes with macular hole.2This suggests that ILM surrounding the myopic macular hole plays a role in reopening of the hole and subsequent devel- opment of retinal detachment. The removal of ILM and overlying epiretinal membrane may increase the flexibility of the detached retina and it may con- tribute to sealing of the macular hole even in the presence of posterior staphyloma.2Primary removal of ILM of the detached retina may also allow com- plete removal of the overlying epiretinal membrane.
Overall initial reattachment rates of 60% to 91%
have been reported for the treatment of myopic reti- nal detachment caused by a macular hole in the pre- vious literature.2,3,5In 1990, Kuriyama et al evaluat- ed reattachment rates of the transscleral and trans- vitreal techniques for treating retinal detachment due to macular hole and reported that the transscler- al approach was superior in initial success rate (83%
vs. 56%).5Other initial success rates that have been reported include vitrectomy with or without an adju- vant agent such as transforming growth factor-β2or platelet extract (60.0%),22vitrectomy with complete epiretinal membrane separation (64.7%),3 vitrecto- my with fluid-gas exchange and endolaser around the macular hole (62.5%),23simplified gas injection method (83%)10, and vitrectomy with ILM removal (70~91%).2, 24The previous reports indicated that
the incidence of recurrent retinal detachment increases with a longer follow-up period. Although the initial reattachment was hindered due to the postoperative development of peripheral retinal breaks in a few cases, the initial macular hole clo- sure rate of 79.0% is encouraging. However, the closure of the macular hole is sometimes difficult to attain, despite the complete relief of traction by the removal of ILM. This result suggests that the imbal- ance between the retina and the choroid-sclera com- plex associated with axial elongation and posterior staphyloma might be involved in the development of retinal detachment by myopic macular hole.
Overall, the initial success rate of myopic macu- lar hole closure after vitrectomy with ILM removal seems higher than that of the previous studies.
Moreover, this technique eliminates the necessity of a second vitreous surgical procedure, even in the case of recurred retinal detachment. We think that perifoveal ILM may be an important adjuvant to treat the myopic macular hole with retinal detach- ment.
REFERENCES
1. Ishida S, Yamazaki K, Shinoda K, Kawashima S, Oguchi Y. Macular hole retinal detachment in highly myopic eyes: ultrastructure of surgically removed epiretinal membrane and clinicopathologic correla- tion. Retina. 2000;20:176-183.
2. Kadonosono K, Yazama F, Itoh N, Uchio E, Nakamura S, Akura J, Sawada H, Ohno S. Treatment of retinal detachment resulting from myopic macular hole with internal limiting membrane removal. Am J Ophthalmol. 2001;131:203-207.
3. Oshima Y, Ikuno Y, Motokura M, Nakae K, Tano Y.
Complete epiretinal membrane separation in highly myopic eyes with retinal detachment resulting from a macular hole. Am J Ophthalmol. 1998;126:669-676.
4. Gonvers M, Machemer R. A new approach to treat- ing retinal detachment with macular hole. Am J Ophthalmol. 1982;94:468-472.
5. Kuriyama S, Matsumura M, Harada T, Ishigooka H, Ogino N. Surgical techniques and reattachment rates in retinal detachment due to macular hole. Arch oph- thalmol. 1990;108:1559-1561.
6. Ripandelli G, Maria A, Fedeli R, Parisi V, D’Amico DJ, Stirpe M. Evaluation of primary surgical proce- dures for retinal detachment with macular hole in highly myopic eyes. Ophthalmology. 2001;108:2258-
2265.
7. Sasoh M, Yoshida S, Ito Y, Matsui K, Osawa S, Uji Y. Macular buckling for retinal detachment due to macular hole in highly myopic eyes with posterior staphyloma. Retina. 2000;20:445-449.
8. Wolfensberger TJ, Gonvers M. Long-term follow-up of retinal detachment due to macular hole in myopic eyes treated by temporary silicone oil temponade and laser photocoagulation. Ophthalmology. 1999;106:
1786-1791.
9. Sholda C, Egger SF. Silicone oil tamponade in eyes with posterior staphyloma and retinal detachment caused by macular hole. Acta Ophthalmol Scand.
1998;76:704-706.
10. Miyake Y. A simplified method of treating retinal detachment with macular hole. Arch Ophthalmol.
1986;104:1234-1236.
11. Gass JDM. Idiopathic senile macular hole. Arch oph- thalmol. 1988;106:629-639.
12. Morita H, Ideta H, Ito K, Yonemoto J, Sasaki K, Tanaka S. Causative factors of retinal detachment in macular holes. Retina. 1991;11:281-284.
13. Negi A, Marmor MF. Quantitative estimation of metabolic transport of subretinal fluid. Invest Ophthalmol Vis Sci. 1986;27:1564-1568.
14. Akiba J, Konno S, Sato E, Yoshida A. Retinal detachment and retinoschisis detected by optical coherence tomography in myopic eye with a macular hole. Ophthalmic Surg Lasers. 2000;31:240-242.
15. Takano M, Kishi S. Foveal retinoschisis and retinal detachment in severely myopic eyes with posterior staphyloma. Am J Ophthalmol. 1999;128:472-476.
16. Akiba J, Konno S, Yoshida A. Retinal detachment
associated with a macular hole in severely myopic eyes. Am J Ophthalmol. 1999;128:654-655.
17. Curtin BJ. Posterior staphyloma development in pathologic myopia. Ann Ophthalmol. 1982;14:655- 658.
18. Stirpe M, Michels RG. Retinal detachment in highly myopic eyes due to macular holes and epiretinal trac- tion. Retina. 1990;10:113-114.
19. Wolfensberger TJ, Gonvers M. Surgical treatment of retinal detachment owing to macular hole. Semin Ophthalmol. 2000;15:122-127.
20. Ripandelli G, Parisi V, Friberg TR, Coppe AM, Scassa C, Stripe M. Retinal detachment associated with macular hole in high myopia: using the vitreous anatomy to optimize the surgical approach.
Ophthalmology. 2004;111:726-731.
21. Seike C, Kusaka S, Sakagami K, Ohashi Y.
Reopening of macular holes in highly myopic eyes with retinal detachments. Retina. 1997;17:2-6.
22. Patel SC, Loo RH, Thompson JT, Sjaarda RN.
Macular hole surgery in high myopia. Ophthalmolo- gy. 2001;108:377-380.
23. Kwok AK, Cheng LL, Gopal L, Sharma T, Lam DS.
Endolaser around macular hole in the management of associated retinal detachment in highly myopic eyes.
Retina. 2000;20:439-444.
24. Ichibe M, Yoshizawa T, Murakami K, Ohta M, Oya Y, Yamamoto S, Funaki S, Funaki H, Ozawa Y, Baba E, Abe H. Surgical management of retinal detachment associated with myopic macular hole:
anatomic and functional status of the macula. Am J Ophthalmol. 2003;136:277-284.