http://dx.doi.org/10.14405/kjvr.2014.54.3.171
171
<Original Article>
Chemopreventive effects of garlic and mugwort mixture extract on Helicobacter pylori-associated mouse gastric carcinogenesis
So-Young Youm
1, Tae-Wang Kim
1, Sang Kyung Shin
1, Heon Sang Jeong
2, Jong-Koo Kang
1, Tae Myoung Kim
1, Kil Ho Kim
3, Byeongwoo Ahn
1,*
1
Colleges of Veterinary Medicine, and
2Agriculture, Life & Environment, Chungbuk National University, Cheongju 361-763, Korea
3
Cosan Institute of Water Science, Seoul 134-846, Korea
(Received: February 26, 2014; Revised: May 28, 2014; Accepted: June 2, 2014)
Abstract : Garlic and mugwort have long been used in traditional medicine to prevent various diseases. Several in vitro studies have reported protective efficacies of garlic and mugwort in cases of gastric cancer. In the present study, we investigated the cancer preventive effects of garlic and mugwort mixture extract (GME) in a Helicobacter (H.) pylori-associated gastric carcinogenesis mouse model. To induce gastric cancer, C57BL/6 mice were treated with N- methyl-N-nitrosourea and H. pylori. Various concentrations of GME (0, 100, 500, and 1,000 ppm) were then fed to the mice for 38 weeks, after which the tumor tissues were examined for histopathology, mucin histochemistry and β-catenin. The incidence of gastric tumors was significantly lower in the highest dose GME-treated mice (46.7%) than control mice (85.7%) (p < 0.05). The multiplicity and size of tumors were also significantly reduced by GME feeding in a dose-dependent manner (p < 0.01). Furthermore, GME suppressed the H. pylori-associated chronic inflammation measured by histologic grading of H. pylori density, chronic gastritis, glandular atrophy and intestinal metaplasia in non-tumorous gastric mucosae. Our data suggest that GME suppresses gastric tumorigenesis via suppression of H.
pylori-associated chronic inflammation.
Keywords: artemisia, garlic, gastric cancer, Helicobacter pylori, mouse
Introduction
Gastric cancer is the second most common cause of can- cer related mortality worldwide. Though the gastric cancer rates have been declining for the last 80 years, it remains still one of the most serious cancers in Korea [15].
Generally, the development of gastric cancer involves a multistep process from normal gastric mucosa to chronic gas- tritis, gastric atrophy, intestinal metaplasia (IM), dysplasia and neoplasia. Chronic gastritis leads to a loss of glandular lineages in the gastric fundus, especially acid-secreting pari- etal cells and pepsin-secreting chief cells. Parietal cell loss leads to goblet cell IM and seems to be a prerequisite for the gastric tumorigenesis [10]. Parietal cells are responsible for the secretion of critical growth factors such as TGF- α and amphiregulin [1, 3]. Thus, the loss of parietal cells may elim- inate important agents required for appropriate differentia- tion of gland lineages including mucous neck and chief cells, as well as increase the serum gastrin level as a result of hypochlorhydria [10]. Several studies revealed that the loss of parietal cells with rapid expansion of surface cell numbers
(foveolar hyperplasia) and hypergastrinemia leads to mucous cell metaplasia [10, 24]. In this regard, IM has been accepted as the most prominent candidate for the origination of gas- tric cancer. To confirm IM, the morphologic characteristics by H&E stain with analysis of the types of mucin expressed is necessary [8]. Histochemically, normal gastric mucin is stained with magenta by periodic acid-Schiff (PAS). How- ever, IM produces acidic mucin, of which stain is blue with alcian blue (AB) at pH 2.5. Therefore, AB/PAS staining can discriminate IM from normal gastric mucosa [8].
WHO/IARC classified Helicobacter (H.) pylori as a group 1 carcinogen. H. pylori causes chronic active gastritis and peptic ulcer disease, and its infection is linked to the gastric cancer development [4]. H. pylori directly contacts with gastric epi- thelial cells and stimulate to release various cytokines such as interleukin-1
β(IL-1
β), IL-2, IL-6, interferon-
γ, and tumor necrosis factor-
α[11]. These cytokines activate the pro- inflammatory COX-2, a key enzyme in the formation of inflammatory reaction [24].
In addition, H. pylori affects intracellular signal transduc- tion in host cells, leading to the activation of transcriptional
*Corresponding author
Tel: +82-43-261-2508, Fax: +82-43-271-3246 E-mail: [email protected]
factors. H. pylori-host interaction and disease progression depend on different bacterial factors such as VacA and CagA [25, 29]. These genes have effect of the increase phosphory- lation of glycogen synthase kinase 3
β(GSK3
β) via the acti- vation of phosphoinositide-3-kinase/Akt, with subsequent release of β-catenin from a GSK3β/β-catenin complex and its nuclear translocation, which leads to activation of various oncogenes, including c-myc, cyclin D1 and matrix metallo- proteinase-3 which have been reported to be target mole- cules of the unphosphorylated β-catenin [28]. Consistent with these findings, altered expression and intracellular redistribu- tion of β-catenin are important for gastric cancer develop- ment as well [6]. Thus, nuclear expression of β-catenin appears to have prognostic value in the evaluation of gastric tumors [20].
Garlic has been intensively studied for the past few decades for their ability to impart beneficial effects on several human diseases including antimicrobial [5, 12], anti-inflammatory and various antitumor effects on hepatic cancer [30], and col- orectal cancer [2, 19]. Artemisia montana is a kind of mug- wort belonging to the family Asteraceae, which has 500 or more species of Artemisia in the world. In Korea, it has tra- ditionally been used for human health possibly as home rem- edies. Some Artemisia spp. have been reported to have some beneficial effects such as anti-inflammation, anti-microbial, anti-cancer, and anti-oxidant activities [7, 13, 18]. Some components such as terpenoids, flavonoids, coumarins, gly- cosides, sterols and polyacetylens were known to be respon- sible for those effects [27].
In this study, therefore, we investigated the chemopreven- tive effects of garlic and mugwort (Artemisia montana) extract on H. pylori-associated gastric cancer in a mouse model.
Materials and Methods
Animals
Specific pathogen-free, 6-week-old male C57BL/6 mice were obtained from Japan SLC (Shizuoka, Japan). All ani- mal experiments were performed in accordance with Stan- dard Operation Procedures of Laboratory Animals that were approved by the Institutional Animal Care and Use Commit-
tee of the Laboratory Animal Research Center of Chungbuk National University, Cheongju, Korea. All mice were given a Teklad Global 18% protein rodent diet (Harlan Laboratories, USA) ad libitum and were maintained under specific patho- gen-free conditions.
Reagents and H. pylori culture
N-methyl-N-nitrosourea (MNU) was purchased from Sigma- Aldrich (USA) and a solution was prepared by dissolving MNU in distilled water at a concentration of 200 ppm.
Mouse-adapted H. pylori (Sydney strain 1, SS1) was inocu- lated on Brucella agar (Becton and Dickinson company, USA) containing 10% heat-inactivated fetal bovine serum and Skirrow medium (Difco, USA). They were kept at 37
oC under micro-aerobic conditions using GasPak jar and Campypak (Becton and Dickinson company).
Preparation of garlic and mugwort extract
The garlic and Artemisia montana were purchased from Kyungdong Market in Seoul. Voucher specimens are depos- ited at College of Agriculture, Life and Environmental Sci- ences, Chungbuk National University, Cheongju, Korea.
Fresh garlic (20 g) and dried leaves of Artemisia montana (40 g) were mixed with 800 mL of 70% ethanol and extracted three times with 30 min ultrasonication. The extracts were then filtered through Whatman No. 2 paper to remove the debris. The filtrates were concentrated using rotary evapora- tion (Rotovapor R-114, BÜCHI Labortechnik, USA) and then freeze-dryed. The yield of the ethanolic extract was measured to be 22.14% of the raw material. For solvent frac- tionation, it was suspended in water, and then extracted suc- cessively with equal volumes of n-hexane, chloroform, and ethylacetate, leaving residual aqueous fraction. Each fraction was evaporated in vacuo to yield the residues of hexane (4.39%), chloroform (6.52%), ethylacetate (3.94%), aqueous (85.15%) fractions, respectively. The chloroform fraction of the ethanol extract was used for the experiment.
Mouse gastric cancer model
The gastric cancers were induced by co-treatment of MNU and H. pylori [21]. The experimental protocol was illustrated
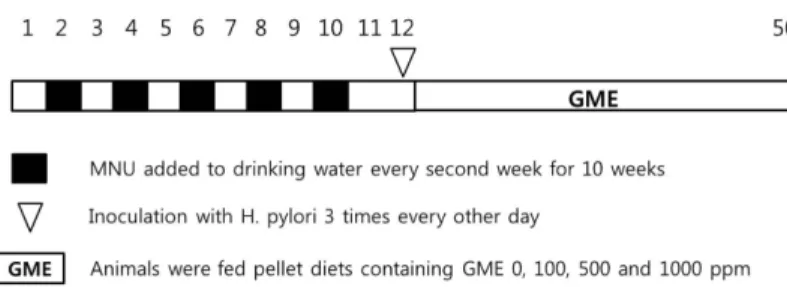
Fig. 1. Study design. All mice were given N-methyl-N-nitrosourea (MNU) that was mixed in their drinking water at concentration of 200 ppm for a total five cycles one-week regimens with a one-week pause. After completion of the MNU administration, they were further inoculated with Helicobacter (H.) pylori three times every other day. Animals of groups 1, 2, 3, 4 were then given a basal diet containing garlic and mugwort mixture extract (GME) 0 ppm, 100 ppm, 500 ppm, 1,000 ppm, respectively. Mice were sacrificed after 38 week GME treatment.
in Fig. 1. Briefly, 80 mice were randomized into 4 groups, which were positive control group (group 1) and GME administration groups (group 2, group 3, group 4). The total mice were given the solution of MNU (200 ppm) ad libitum in place of drinking water every other week for 10 weeks.
One week after the completion of the MNU administration, they were further inoculated with 0.1 mL of H. pylori suspen- sion containing 1 × 10
9colony-forming units/mL by intragastric intubation three times every other day. Then, the mice were given a basal diet containing GME at the concentrations of 0 ppm (group 1), 100 ppm (group 2), 500 ppm (group 3), 1,000 ppm (group 4) throughout the experiment. All mice were sacrificed at 50th week from the start of the experiment.
Histological analysis
At sacrifices, the stomachs were inflated with buffered for- malin and opened along the greater curvature. The numbers of neoplastic nodules were counted under a stereoscopic microscope, and the sizes of the nodules were measured with a vernier-caliper. The excised stomachs were fixed in neutral buffered 10% formalin and processed by routine methods for paraffin embedment. The tissues were sectioned at a thick- ness of 4 µm and stained with haematoxylin and eosin (H&E). Histopathologic typing of gastric tumors was deter- mined by Lauren’s classification [17].
Histologic analysis of chronic inflammation
To determine the effects of GME on chronic inflamma- tion, histologic grades for chronic gastritis, glandular atro- phy, IM and H. pylori density were examined. H&E and May Grünwald Giemsa stains were used for histopathology of chronic inflammation. Warthin-Starry silver stain and AB/
PAS were performed for H. pylori colonization and the pres- ence of IM, respectively. The histologic grades including H.
pylori density were scored according to the histologic classi- fication of the updated Sydney system [10] into four grades (0~3; 0, none; 1, mild; 2, moderate; 3, severe).
Immunohistochemical staining
Immunohistochemistry for β-catenin was performed with monoclonal antibody against β-catenin (clone 14, 1 : 200 dilution; BD Transduction Laboratories, USA) after antigen retrieval protocol [26]. The reactivity of β-catenin in nucleus was classified into negative, scattered, focal positive and dif- fuse positive as described by Kobayashi et al. [16]. The neg-
ative was defined as localization limited to cytoplasmic membranes. The scattered pattern presented as nuclear stain- ing less than 5% of the cells without any cluster. The focal positive pattern was defined as positive cells clustered in focal area and diffuse positive as positive cells distributed diffusely. Cytoplasmic immunoreactivity was not considered in the present study because this expression was variable and not clearly related to the shift from membranous to nuclear staining [22].
Statistical analyses
The data were analyzed with SAS software (ver. 9.1.2;
SAS Institute, USA). Tests for statistical analyses were Fisher’s exact test for tumor incidence, malignancy and nuclear β-catenin expression data, Tukey t test after ANOVA for tumor multiplicity and size, Dunn’s multiple comparison test after Kruskal-Wallis’ nonparametric ANOVA for histo- logic scores of chronic inflammation. For all comparisons, p values < 0.05 were considered statistically significant.
Results
Tumor incidence, multiplicity and sizes
Table 1 summarizes the incidence, multiplicity and sizes of gastric tumors. Mice from group 1 showed 85.7% in the inci- dence, 7 in the multiplicity and 6.8 mm in the sizes of the gastric tumors induced by the MNU and H. pylori regimen.
Treatment of GME 1,000 ppm (group 4) significantly impaired the incidence to 46.7% (p < 0.05). In tumor multiplicity, the treatment of GME 500 ppm and 1000 ppm significantly decreased the number of tumors in tumor bearing mice (p <
0.05). In addition, tumor sizes significantly impaired in all GME treatment groups (p < 0.01) when compared to group 1.
Histological classification of gastric tumors
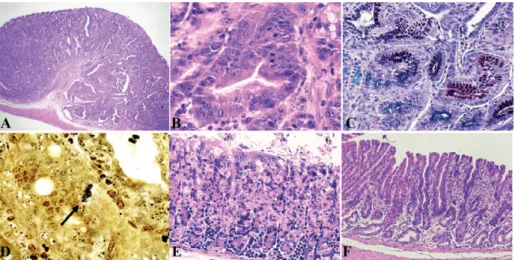
As shown in Table 2, the incidences of adenocarcinoma in the all GME treatment groups were significantly reduced when compared to group 1 (p < 0.01). Histological typing of adenocarcinoma was mainly intestinal type in group 1 (81.8%). Gastric adenocarcinoma showed an irregular glan- dular proliferation and stromal invasion of tumor cells (Fig.
2A). The hyperplastic irregular gland was composed of hyperchromatic atypical tumor cells showing loss of colum- nar orientation and cell stratification (Fig. 2B). In this lesion, there were increased intestinal type acidic mucins (blue) in
Table 1. Tumor incidence, multiplicity and tumor size
Groups Incidence (%) Multiplicity Size (mm)
1 12/14 (85.7) 7.0± 0.10 6.83± 0.49
2
16/12 (50.0)
5.0± 0.76 3.27± 0.23**3
16/12 (50.0)
4.3± 0.33* 3.19± 0.17**4
17/15 (46.7)*
2.8± 0.29* 3.00± 0.17***, **Significantly different from group 1 at p < 0.05 and p < 0.01, respectively. Data represent the mean± SD.
the oxyntic mucosa (Fig. 2C).
Chronic atrophic gastritis and intestinal metaplasia Since GME treatment suppressed the development of gas- tric tumors, the gastric mucosae of non-neoplastic lesion were examined histologically to determine whether GME affected the development of precursor lesions of dysplasia (glandular atrophy, chronic inflammation and intestinal metaplasia). GME also significantly suppressed the histologic grades of those lesions in high dose groups determined by quantitative histo- pathological scoring (p < 0.05) (Table 3). The density of H.
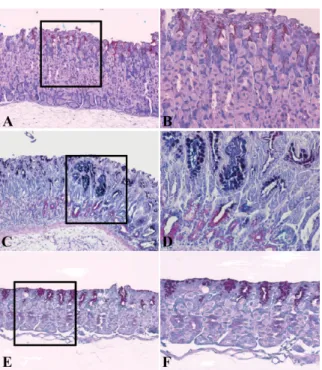
pylori colonization was also significantly impaired by GME treatment (Table 3, Fig. 2D). Chronic gastritis was character- ized by moderate-to-severe infiltration of lymphocytes, plasma cells and neutrophils (Fig. 2E) and the loss of parietal cells and chief cells, and replacement with proliferating epithelial cells (Fig. 2F). The histochemical pattern of IM was different between group 1 and GME treatment groups. In group 1, gas- tric mucosa was exhibited the change of mucin type to the acidic and mixed mucin stained by AB/PAS (Figs. 3C and D) and GME treated groups are tend to exhibit PAS positive (neu-
Table 2. Incidences of gastric tumors according to histopathologic classificationGroups Adenoma
(%)
Adenocarcinoma (%)
Adenocarcinoma subtype Intestinal (%) Mixed (%)
1 1/14 (7.1) 11/14 (78.6) 9/11 (81.8) 2/11 (18.2)
2 2/12 (16.7)
14/12 (30.8)**
4/4 (100) 0/4 (0)3 3/12 (25.0)
13/12 (25.0)**
3/3 (100) 0/3 (0)4 4/15 (26.7)
13/15 (20.0)**
3/3 (100) 0/3 (0)**Significantly different from positive control group (group 1) at p < 0.01.
Fig. 2. Histopathology of the gastric lesions. (A) A representative adenocarcinoma. Note the irregular glandular proliferation and stro- mal invasion. (B) In high magnification of A, tumor cells are showing the loss of columnar orientation and cell stratification. (C) The glandular epithelial cells in the neoplastic lesion secrete intestinal type acidic mucins (blue). (D) Colonized H. pylori between the nuclei of the epithelial cells and basement membrane (arrow). (E) Frequently, severe inflammatory cells infiltration in the gastric mucosa was observed in group 1. (F) A representing lesion of glandular atrophy. Note the loss of parietal cells and chief cells and the replacement with proliferating epithelial cells. H&E stain, ×20 (A); ×200 (B); ×100 (E and F). AB/PAS stain, ×100 (C); Warthin- Starry stain, ×1,000 (D).
Table 3. Scoring of histologic grade of gastritis according to the updated Sydney system
Groups Histologic score
H. pylori density Chronic inflammation Glandular atrophy Intestinal metaplasia
1 1.50± 0.65 2.43± 0.51 2.50± 0.52 2.29± 0.47
2 1.29± 0.76 2.14± 0.69 2.14± 0.69 1.74± 0.95
3 1.00± 0.81* 1.86± 0.76 1.83± 0.76 1.43± 0.53*
4 0.74± 0.76** 1.43± 0.41* 1.74± 0.41* 1.00± 0.63*
*, **Significantly different from positive control group (group 1) at p < 0.05 and p < 0.01, respectively. Data represent the mean± SE.
tral mucin) with more pink staining reaction (Figs. 3E and F).
Nuclear β-catenin expression
A variation of the nuclear staining was detected in the epi- thelial cells of the neoplastic mucosa (Table 4). The strong cytoplasmic and nuclear β-catenin immunoreactivity was observed in the epithelial cells of polyps (Fig. 4B) in group 1 (57.14%). On the other hand, following GME treatment, the expression β-catenin was more tend to be observed in the cell-to-cell border (Fig. 4D) and then the number of cells with nuclear β-catenin expression was significantly lower in group 3 (16.66%) and group 4 (13.33%) compared with
group 1.
Discussion
In the present study, we investigated the preventive effects of GME on gastric cancer with MNU-treated H. pylori-asso- ciated gastric cancer mouse model. The incidence of tumors, multiplicity and tumor sizes were lowered by GME treat- ment. Histological typing of adenocarcinomas was mostly intestinal type according to the Lauren’s classification.
The development of gastric carcinoma involves multiple processes from chronic gastritis to atrophy, intestinal meta- plasia, dysplasia, and, finally, adenocarcinoma. Therefore, to examine the preventive effect of GME on gastric cancer, non-neoplastic lesions of the gastric mucosa were evaluated according to the Updated Sydney System to confirm the pre- neoplastic changes. As results, GME feeding significantly alleviated the severity of H. pylori colonization, chronic gas- tritis, glandular atrophy, and intestinal metaplasia. Extensive inflammation of the infected mucosa and submucosa by var- ious immune cell populations observed in group 1 was sig- nificantly reduced by 1,000 ppm of GME treatment. Also
Fig. 3. Mucin changes in non-neoplastic gastric lesions by AB/PAS staining. (A) Neutral mucin was predominant in normal gastric mucosa. (B) High magnification of rectangle in A. (C) A representative lesion of group 1. Note the reduced parietal cell zone and change of mucin type from neutral mucin to the acidic and mixed mucin. (D) High magnification of rectangle in A shows marked acidic mucin. (E) A representative lesion of group 4. The acidic mucin was almost disappeared by GME treatment.
(F) High magnification of rectangle in C reveals almost normal condition in the gastric cell lineage. ×100(A, C and E). ×200 (B, D and F).
Table 4. The localization of β-catenin
Groups Nuclear β-catenin expressioin (%) Patterns of nuclear β-catenin expression
Negative/scattered Focal Diffuse
1 8/14 (57.14) 2 8 0
2 6/12 (50.00) 0 6 0
3 2/12 (16.66)* 1 2 0
4 2/15 (13.33)* 1 2 0
The nuclear pattern of
β-catenin expression was subdivided into negative/scattered, no or few scattered positive cells; focal, positive cells
clustered in focal area; diffuse, positive cells distributed diffusely. *Significantly different from positive control group (group 1) at p < 0.05.Fig. 4. β-catenin expression in gastric adenocarcinomas. Rep- resentative staining sections of group 1 (A and B) and group 4 (C and D). Note the nuclear translocation of β-catenin in group 1 (B) and the expression of β-catenin in cell to cell border in group 4 (D). H&E stain, ×100 (A); ×200 (C). Immunohis- tochemistry by ABC method, ×100(B); ×200 (D).
severe atrophy characterized by the loss of the parietal cell and chief cell lineages was impaired by treatment of GME.
In addition, alcian blue-positive metaplasia mostly found in group 1 was significantly reduced by 500 and 1,000 ppm of GME treatment.
The protective effect of GME against chronic inflamma- tion of the gastric mucosa was paralleled by significant inhi- bition of gastric atrophy and IM. These data strongly support that GME inhibits gastric carcinogenesis by suppressing the H. pylori colonization, the attendant gastric atrophy and chronic inflammation. In line with this, GME reduces the risk of metaplastic change of the gastric mucosa. In addition, GME inhibited the nuclear translocation of β-catenin in ade- nocarcinomas. The intense β-catenin expression in nuclear and cytoplasm of epithelial cells in tumors of group 1 was significantly reduced in 500 and 1,000 ppm of GME treat- ment groups. β-catenin is known to have important roles related with cell adhesion. It has been documented that muta- tion of β-catenin closely associated with the development of gastric cancer occurs at a higher rate in intestinal type gas- tric cancer rather than the diffuse type [23]. Furthermore, recent studies demonstrated that β-catenin is selectively acti- vated by H. pylori cytotoxin-associated gene (Cag)-A depen- dent manner [9] and abnormal expression of β-catenin is correlated with poor prognosis [14]. Thus, considering the changes of β-catenin expression, it is anticipated that GME reduces H. pylori-associated β-catenin regulation. Therefore, the suppression of gastric cancer in our study may be the result of suppressed gastric inflammation caused by H. pylori infection. This suggestion is consistent with the observed impaired oxyntic atrophy and metaplastic changes by GME.
Therefore, it can be postulated that regression of H. pylori activity by GME inhibits β-catenin nuclear translocation, leading to the suppression of malignancy. In conclusion, GME inhibited the development of gastric tumorigenesis via suppression of H. pylori infection-associated chronic inflam- mation.
GME treatment inhibited the gastric carcinogenesis in MNU and H. pylori-associated mouse gastric cancer model.
In addition to the tumor incidence, multiplicity and sizes, GME treatment also suppressed H. pylori colonization and the development of preneoplastic lesions such as chronic gas- tritis, glandular atrophy and intestinal metaplasia. These results suggest that GME inhibited mouse gastric tumorigen- esis via the suppression of H. pylori infection-associated chronic inflammation.
Acknowledgments
This work was supported by a research grant of Chungbuk National University in 2011.
References
1. Akagi M, Yokozaki H, Kitadai Y, Ito R, Yasui W,
Haruma K, Kajiyama G, Tahara E. Expression of amphiregulin in human gastric cancer cell lines. Cancer 1995, 75 (Suppl 6), 1460-1466.
2. Alpers DH. Garlic and its potential for prevention of colorectal cancer and other conditions. Curr Opin Gastroenterol 2009, 25, 116-121.
3. Beauchamp RD, Barnard JA, McCutchen CM, Cherner JA, Coffey RJ Jr. Localization of transforming growth factor alpha and its receptor in gastric mucosal cells.
Implications for a regulatory role in acid secretion and mucosal renewal. J Clin Invest 1989, 84, 1017-1023.
4. Blaser MJ, Chyou PH, Nomura A. Age at establishment of Helicobacter pylori infection and gastric carcinoma, gastric ulcer, and duodenal ulcer risk. Cancer Res 1995, 55, 562-565.
5. Cellini L, Di Campli E, Masulli M, Di Bartolomeo S, Allocati N. Inhibition of Helicobacter pylori by garlic extract (Allium sativum). FEMS Immunol Med Microbiol 1996, 13, 273-277.
6. Chen XY, Wang ZC, Li H, Cheng XX, Sun Y, Wang XW, Wu ML, Liu J. Nuclear translocations of β-catenin and TCF4 in gastric cancers correlate with lymph node metastasis but probably not with CD44 expression. Hum Pathol 2005, 36, 1294-1301.
7. Choi EJ, Kim GH. Antioxidant and anticancer activity of Artemisia princeps var. orientalis extract in HepG2 and Hep3B hepatocellular carcinoma cells. Chin J Cancer Res 2013, 25, 536-543.
8. Correa P, Piazuelo MB, Wilson KT. Pathology of gastric intestinal metaplasia: clinical implications. Am J Gastroenterol 2010, 105, 493-498.
9. Franco AT, Israel DA, Washington MK, Krishna U, Fox JG, Rogers AB, Neish AS, Collier-Hyams L, Perez-Perez GI, Hatakeyama M, Whitehead R, Gaus K, O’Brien DP, Romero-Gallo J, Peek RM Jr. Activation of β-catenin by carcinogenic Helicobacter pylori. Proc Natl Acad Sci U S A 2005, 102, 10646-10651.
10. Goldenring JR, Nomura S. Differentiation of the gastric mucosa III. Animal models of oxyntic atrophy and metaplasia.
Am J Physiol Gastrointest Liver Physiol 2006, 291, G999- 1004.
11. Hahm KB, Song YJ, Oh TY, Lee JS, Surh YJ, Kim YB, Yoo BM, Kim JH, Han SU, Nahm KT, Kim MW, Kim DY, Cho SW. Chemoprevention of Helicobacter pylori-associated gastric carcinogenesis in a mouse model:
is it possible? J Biochem Mol Biol 2003, 36, 82-94.
12. Iwalokun BA, Ogunledun A, Ogbolu DO, Bamiro SB, Jimi-Omojola J. In vitro antimicrobial properties of aqueous garlic extract against multidrug-resistant bacteria and Candida species from Nigeria. J Med Food 2004, 7, 327-333.
13. Jeong D, Yi YS, Sung GH, Yang WS, Park JG, Yoon K, Yoon DH, Song C, Lee Y, Rhee MH, Kim TW, Kim JH, Cho JY. Anti-inflammatory activities and mechanisms of Artemisia asiatica ethanol extract. J Ethnopharmacol 2014, 152, 487-496.
14. Joo YE, Park CS, Kim HS, Choi SK, Rew JS, Kim SJ.
Prognostic significance of E-cadherin/catenin complex expression in gastric cancer. J Korean Med Sci 2000, 15, 655-666.
15. Kim YJ, Chung JW, Lee SJ, Choi KS, Kim JH, Hahm KB. Progression from chronic atrophic gastritis to gastric
cancer; tangle, toggle, tackle with Korea red ginseng. J Clin Biochem Nutr 2010, 46, 195-204.
16. Kobayashi M, Honma T, Matsuda Y, Suzuki Y, Narisawa R, Ajioka Y, Asakura H. Nuclear translocation of beta- catenin in colorectal cancer. Br J Cancer 2000, 82, 1689- 1693.
17. Lauren P. The two histological main types of gastric carcinoma: diffuse and so-called intestinal type carcinoma.
An attempt at a histo-clinical classification. Acta Pathol Microbiol Scand 1965, 64, 31-49.
18. Masadeh MM, Alkofahi AS, Alzoubi KH, Tumah HN, Bani-Hani K. Anti-Helicobactor pylori activity of some Jordanian medicinal plants. Pharm Biol 2014, 52, 566-569.
19. Matsuura N, Miyamae Y, Yamane K, Nagao Y, Hamada Y, Kawaguchi N, Katsuki T, Hirata K, Sumi S, Ishikawa H. Aged garlic extract inhibits angiogenesis and proliferation of colorectal carcinoma cells. J Nutr 2006, 136 (Suppl 3), 842S-846S.
20. Nabais S, Machado JC, Lopes C, Seruca R, Carneiro F, Sobrinho-Simões M. Patterns of β-catenin expression in gastric carcinoma: clinicopathological relevance and mutation analysis. Int J Surg Pathol 2003, 11, 1-9.
21. Nam KT, Hahm KB, Oh SY, Yeo M, Han SU, Ahn B, Kim YB, Kang JS, Jang DD, Yang KH, Kim DY. The selective cyclooxygenase-2 inhibitor nimesulide prevents Helicobacter pylori-associated gastric cancer development in a mouse model. Clin Cancer Res 2004, 10, 8105-8113.
22. Osterheld MC, Bian YS, Bosman FT, Benhattar J, Fontolliet C. Beta-catenin expression and its association with prognostic factors in adenocarcinoma developed in Barrett esophagus. Am J Clin Pathol 2002, 117, 451-456.
23. Park WS, Oh RR, Park JY, Lee SH, Shin MS, Kim
YS, Kim SY, Lee HK, Kim PJ, Oh ST, Yoo NJ, Lee JY. Frequent somatic mutations of the beta-catenin gene in intestinal-type gastric cancer. Cancer Res 1999, 59, 4257- 4260.
24. Peek RM Jr, Blaser MJ. Helicobacter pylori and gastrointestinal tract adenocarcinomas. Nat Rev Cancer 2002, 2, 28-37.
25. Penta R, De Falco M, Iaquinto G, De Luca A. Helicobacter pylori and gastric epithelial cells: from gastritis to cancer. J Exp Clin Cancer Res 2005, 24, 337-345.
26. Shi SR, Chaiwun B, Young L, Cote RJ, Taylor CR.
Antigen retrieval technique utilizing citrate buffer or urea solution for immunohistochemical demonstration of androgen receptor in formalin-fixed paraffin sections. J Histochem Cytochem 1993, 41, 1599-1604.
27. Turi CE, Shipley PR, Murch SJ. North American Artemisia species from the subgenus Tridentatae (Sagebrush):
a phytochemical, botanical and pharmacological review.
Phytochemistry 2014, 98, 9-26.
28. Utsunomiya T, Doki Y, Takemoto H, Shiozaki H, Yano M, Inoue M, Yasuda T, Fujiwara Y, Monden M. Clinical significance of disordered beta-catenin expression pattern in human gastric cancers. Gastric Cancer 2000, 3, 193-201.
29. Yamaoka Y, Ojo O, Fujimoto S, Odenbreit S, Haas R, Gutierrez O, El-Zimaity HM, Reddy R, Arnqvist A, Graham DY. Helicobacter pylori outer membrane proteins and gastroduodenal disease. Gut 2006, 55, 775-781.
30. Zhang ZM, Yang XY, Deng SH, Xu W, Gao HQ. Anti- tumor effects of polybutylcyanoacrylate nanoparticles of diallyl trisulfide on orthotopic transplantation tumor model of hepatocellular carcinoma in BALB/c nude mice. Chin Med J (Engl) 2007, 120, 1336-1342.