237
전립선생검에서 비전형적작은꽈리증식증으로 진단된 환자의 재생검 결과
Prostate Cancer Detection Rate of Rebiopsy in Patients with an Initial Diagnosis of Atypical Small Acinar Proliferation of the Prostate
Jung Woo Oh, Yun Beom Kim, Seung Ok Yang, Jeong Ki Lee, Yoon Jung Kim1, Tae Young Jung, Hong Bang Shim
From the Departments of Urology, 1Pathology, Seoul Veterans Hospital, Seoul, Korea Purpose: Atypical small acinar proliferation (ASAP) denotes the presence of suspicious glands with insufficient cytological architecture for a definitive prostate cancer diagnosis. We evaluated the subsequent prostate cancer detection rate of rebiopsy in patients with an initial diagnosis of ASAP.
Materials and Methods: Between January 2003 and December 2006, 1,416 men with suspected prostate cancer underwent a transrectal ultrasound- guided prostate biopsy, and 214 (15.1%) were diagnosed as having ASAP.
Ninety-five of the 215 patients underwent at least one more biopsy. We evaluated the cancer detection rates after rebiopsy.
Results: In men with ASAP, 36 patients (37.9%) had prostate cancer. The cancer detection rates of the 1st, 2nd, and 3rd rebiopsies were 30.5%, 23.8%, and 40%, respectively. Mean patient age and prostate-specific antigen did not differ significantly between the prostate cancer and noncancer groups after rebiopsy. Prostate volume, however, was significantly smaller in the cancer group (p<0.05).
Conclusions: Our results showed a detection rate for prostate cancer of 37.9% after an initial diagnosis of ASAP, which indicates that an initial diagnosis of ASAP mandates rebiopsy. (Korean J Urol 2009;50:237-240)
Key Words: Atypical small acinar proliferation, Biopsy, Prostatic neoplasms
Korean Journal of Urology Vol. 50 No. 3: 237-240, March 2009 DOI: 10.4111/kju.2009.50.3.237
서울보훈병원 비뇨기과, 1병리과
오정우ㆍ김윤범ㆍ양승옥ㆍ이정기
김윤정1ㆍ정태영ㆍ심홍방
Received:December 17, 2008 Accepted:February 16, 2009 Correspondence to: Tae Young Jung
Department of Urology, Seoul Veterans Hospital, Dunchon 2-dong,Gangdong-gu, Seoul 134-791, Korea
TEL: 02-2225-1739 FAX: 02-484-4604
E-mail: [email protected]
Ⓒ The Korean Urological Association, 2009
서 론
경직장초음파유도 전립선침생검은 전립선암 진단을 위한 표준 시술로 인정되고 있다.1 전립선생검의 조직소견으로 는 전립선암 이외에 결절성비대 (nodular hyperplasia), 전립 선염 (prostatitis), 전립선상피내종양 (prostatic intraepithelial neoplasia; PIN), 비전형적선증 (atypical adenosis), 비전형적 꽈리증식증 (atypical small acinar proliferation; ASAP) 등이 있다.2 이 중 비전형적작은꽈리증식증은 전립선암이 의심 되지만 확진을 내리기에는 부족한 전립선 내의 작은 선 (gland) 조직을 말하는 것으로, 재생검 시 34-60%에서 전립 선암으로 보고되고 있어3-12 최근 임상적 중요성이 높아지고 있으나 국내에서는 아직 이와 관련된 보고가 매우 드문 실
정이다. 이에 저자들은 전립선생검에서 비전형적작은꽈리 증식증이 진단된 환자들을 대상으로 시행한 재생검의 결과 를 분석하여, 비전형적작은꽈리증식증의 임상적 중요성을 알아보고자 하였다.
대상 및 방법
2003년 1월부터 2006년 12월까지 혈중 전립선특이항원치 가 4 ng/ml 이상으로 상승되었거나 경직장초음파에서 저반 향소견을 보인 1,416명에서 전립선생검을 시행하였고, 비전 형적작은꽈리증식증은 214명 (15.1%)에서 진단되었다. 그 중 전립선암이나 전립선상피내종양이 동반되거나 직장수 지검사에서 결절이 촉진된 경우를 제외한 1회 이상의 전립 선 재생검을 시행 받은 95명의 환자를 대상으로 하였으며,
238 Korean Journal of Urology vol. 50, 237-240, March 2009
Table 1. Characteristics of the patients
Total ASAP(rebiopsy)
No. of patients 1416 95 Mean age (years) 70.3 (48-90) 69.4 (57-77) Median PSA (ng/ml) 18.7 (0.047-3479) 12.7 (2.9-89.9) Median prostate
volume (cc) 43.1 (10.9-154.2) 47.1 (12.6-141.9) PSA: prostate-specific antigen, ASAP: atypical small acinar pro- liferation
Table 2. Results of rebiopsy
Rebiopsy No. of patients Rebiopsy diagnosis
Negative ASAP Cancer
1st 95 39 27 29 (30.5%) 2nd 21 9 7 5 (23.8%) 3rd 5 2 1 2 (40.0%) ASAP: atypical small acinar proliferation
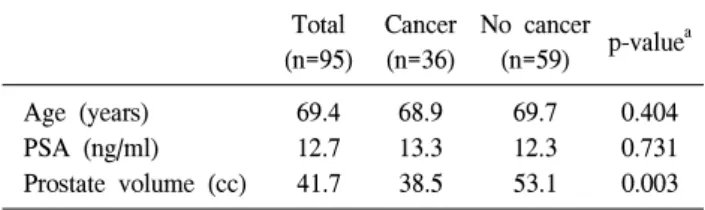
Table 3. Median parameters in patients after rebiopsy Total
(n=95)
Cancer (n=36)
No cancer
(n=59) p-valuea
Age (years) 69.4 68.9 69.7 0.404
PSA (ng/ml) 12.7 13.3 12.3 0.731
Prostate volume (cc) 41.7 38.5 53.1 0.003 PSA: prostate-specific antigen. ap-value: Student's t-test 이들의 기록을 후향적으로 분석하였다. 재생검을 시행 받
은 환자의 평균 연령은 69.4세 (57-77)였고, 평균 전립선특 이항원은 12.7 ng/ml (2.9-89.9)였으며, 경직장초음파에서 평 균 전립선 용적은 47.1 cc (12.6-141.9)였다 (Table 1). 전립선 생검은 환자가 측와위를 취한 상태에서 경직장초음파 (IU-22; PHILIPS, U.S.A) 유도하에 18 Gauge 침을 장착한 생 검총 (ACECUT; TSK laboratory, Japan)을 이용하여 시행하 였으며, 전립선 용적의 계측은 경직장초음파에서 측정한 전립선의 전후 길이x상하 높이x좌우 직경에 0.523을 곱한 공식을 이용하였다. 생검개수는 경직장초음파에서 전립선 용적이 30 cc 이하인 경우 6개, 30 cc 이상인 경우 10-12개로 하였다. 첫 재생검은 비전형적작은꽈리증식증으로 진단받 은 후 평균 6.8개월 (2-57), 2회 재생검은 평균 8.3개월 (1-16), 3회 재생검은 평균 8개월 (3-10) 후에 시행되었다. 모 든 병리검사는 1명의 병리학자에 의해 시행되었고, 기본 H&E 염색 이외에 진단이 힘든 경우에는 기저세포 특이염 색을 위해 34βE12 (high molecular weight cytokeratin)와 p63 으로 면역조직화학염색을 시행하였다. 비전형적작은꽈리 증식증의 임상적 중요성을 알아보기 위해 각 재생검 시 전 립선암의 검출률 및 전립선암이 진단된 군과 생검에서 음 성으로 진단된 군에서의 나이, 혈청 전립선특이항원, 경직 장초음파에서 전립선용적 등의 임상적 인자에 따른 차이를 비교 분석하였다. 통계처리는 Student's t-test (paired)를 시행 하였고, p값이 0.05 미만인 경우에 통계학적으로 유의한 것 으로 판정하였다.
결 과
비전형적작은꽈리증식증으로 재생검을 시행 받은 총 95 명 중 최종적으로 36명 (37.9%)에서 전립선암이 진단되었 다. 첫 재생검에서는 95명 중 29명 (30.5%)이 전립선암, 27 명 (28.4%)에서 비전형적작은꽈리증식증이, 39명 (41.1%)에 서 음성으로 보고되었고, 첫 재생검에서 전립선암으로 진 단된 29명을 제외한 비전형적작은꽈리증식증 또는 음성으
로 진단된 환자 (66명) 중 21명에서 2회 재생검이 시행되었 는데, 5명 (23.8%)에서 전립선암, 7명 (33.3%)에서 비전형적 작은꽈리증식증, 9명 (42.9%)에서 음성으로 보고되었다. 3 회 재생검은 2회 재생검에서 전립선암으로 진단된 5명을 제외한 비전형적작은꽈리증식증 또는 음성으로 진단된 환 자 (16명) 중 5명에서 시행되었고, 그 중 2명 (40%)이 전립 선암으로, 1명 (20%)이 비전형적작은꽈리증식증, 2명 (40%) 이 음성으로 보고되었다 (Table 2). 환자들의 평균 연령과 혈청 PSA수치는 전립선암으로 진단된 환자군에서는 68.9 세 (57-77), 13.3 ng/ml (3.93-89.9)였고, 전립선암으로 진단되 지 않은 환자군에서는 69.7세 (55-77), 12.3 ng/ml (2.9-82.5) 로 통계적으로 유의한 차이가 없었으나 (p=0.404, p=0.731), 경직장초음파로 측정한 평균 전립선용적은 전립선암으로 진단된 환자군에서는 38.5 cc (17.3-83.1), 전립선암으로 진 단되지 않은 환자군에서는 53.1 cc (12.6-141.9)로 통계학적 으로 유의한 차이가 있었다 (p<0.05)(Table 3). 전립선암으 로 진단된 환자군의 Gleason 점수는 7 미만이 22명, 7 이상 이 14명이었다.
고 찰
통상적으로 전립선암은 혈청 전립선특이항원, 직장수지 검사, 경직장초음파 등의 검사에서 이상소견이 보일 때 전 립선생검을 통해 진단된다. 전립선생검 조직의 병리소견 중 비전형적작은꽈리증식증은 세포학적이나 구조적인 비 정형성으로 전립선암이 의심되지만 확진을 내리기에는 부 족한 전립선 내의 작은 선 (gland) 조직을 말하는 것으로,
Jung Woo Oh, et al:Atypical Small Acinar Proliferation of the Prostate 239
하나의 병리학적 진단 자체라기보다는 기저세포과형성 (basal cell hyperplasia), 샘증 (adenosis), 양성군집선 (benign crowded glands), 반응성비정형 (reactive atypia), 작은 전립선 용적의 구조적 왜곡 (artifactual distortion) 등의 소견을 포함 할 수 있다.13 또한 다른 보고들에서는 위에서 기술한 소견 이 보이는 경우, 전립선암이 의심되지만 핵소체와 핵의 비 대가 없거나 구조적인 왜곡을 보이고 확진하기에는 선의 개수가 너무 적을 때, 그리고 조직이 소실되거나 기저세포 의 염색이 불가능한 경우와 같은 소견들로 인해 비전형적 작은꽈리증식증이라는 용어가 빈번하게 사용되고 있다고 주장하였다.4,10,14
비전형적작은꽈리증식증의 빈도는 보고자마다 다양하여 0.7-23.4%까지 보고되었으나,15 면역조직화학염색의 발달로 최근에는 1.5-9%로 보고되고 있다.7,9,16.17 본 연구에서는 전 립선생검을 시행한 총 1,416명 중 214명 (15.1%)이 비전형 적작은꽈리증식증으로 진단되었다.
일반적으로 비전형적작은꽈리증식증이 병리학적 실체로 받아들여지고 있음에도 불구하고 다음과 같은 비판들이 존 재한다. 첫째, 비전형적작은꽈리증식증을 마치 진단처럼 기 술함으로 인해 병리학적인 불확실성을 정당화한다는 견해 이고18 둘째, 몇몇 대규모 연구에서 비전형적작은꽈리증식 증으로 진단된 이후 재생검률이 제일 높은 보고에서도 70%
를 넘지 못함으로써3,4,9-11 의사와 환자 모두에게 조직검사 결 과의 심각성을 적절히 전달해 주지 못한 점이며 셋째, 판독 자 간의 높은 다양성이 존재한다는 사실이다.13 Brausi 등19 은 비전형적작은꽈리증식증의 판독에 있어 병리학자 간에 동일 병소에 대한 일치율이 각각 84%, 78%라고 주장하였 는데 이는 비전형적작은꽈리증식증의 병소들을 해석하는 데에 어려움이 있어 병리학자 간에도 서로 다른 판독 소견 이 나올 수 있음을 시사한다. 이러한 문제점이 있음에도 불 구하고 비전형적작은꽈리증식증이 임상에서 중요시 되는 이유는, 재생검 시 전립선암의 진단율이 34-60%에 이른다 는 점이다.3-12
Mancuso 등20은 1994년부터 2004년 동안 전립선생검을 받은 1,632명 중 첫 생검에서 비전형적작은꽈리증식증을 진단받은 61명 (4.0%) 중 추적관찰이 가능하였던 31명을 대 상으로 후향적으로 조사하였고 이 중 22명의 환자에서 한 번 이상의 재생검이 시행되었는데, 첫 재생검을 시행 받은 22명의 환자 중 13명, 2회 재생검에서는 5명 중 3명, 3회 재 생검에서는 4명 중 1명이 전립선암으로 진단되었으며 총 31명 환자 중 17명 (55%)이 전립선암으로 진단되었다고 보 고하였다. 본 연구에서는 첫 재생검에서 비전형적작은꽈리 증식증으로 보고된 환자 중 44.4%가 재생검을 시행 받았고 이 중 37.9%가 전립선암으로 진단되었다. 본 연구의 경우
재생검에서 전립선암의 진단율이 다른 연구자들이 발표한 결과 안에 포함되어 있기는 하지만 약간 낮은 이유를 들자 면 첫째, 생검을 영상의학과에 의뢰하여 시행하므로 비전 형적작은꽈리증식증이 나온 부위에 대한 집중적인 추가생 검 및 확장생검 (extended biopsy)을 하지 못한 점과, 전립선 의 용적이 큰 경우 포화생검 (saturation biopsy)을 하는 등의 전체 생검 수를 늘리지 못한 점이고 둘째, H&E 염색외에 면역조직화학검사로 34βE12 및 p63을 이용하였으나, 전립 선암 조직에서 단백발현의 민감도가 97%, 특이도가 100%
인 AMACR (P504S)은 시행하지 못한 점이 있고 셋째, 고령 및 동반질환이 많아 재생검을 받지 못하고 추적 관찰만 받 고 있는 환자가 많은 점 등을 원인으로 생각한다.
비전형적작은꽈리증식증의 진단 후에 재생검 시기에 대 해 확실히 정해진 원칙은 없지만 3개월 이내 혹은 가급적 조기에 해야 한다는 보고가 많다.20,21 본 연구에서는 3개월 에서 6개월 사이에 재생검을 권유하였지만 동반 질환, 환자 의 고통 및 비용 문제로 첫 재생검은 평균 6.8개월, 2회 재생 검은 평균 8.3개월, 3회 재생검은 평균 8개월 후에 시행되었 다. 저자들의 경우 병리학적 보고에서 강력히 전립선암이 의심되거나 (ASAP, highly suspicious for malignancy) 혈청 전립선특이항원이 지속적으로 상승되는 경우, 혹은 추적검 사 중 직장수지검사에서 결절이 촉지된 경우 최대 5회까지 재생검을 시행하기도 하였다.
재생검에서 진단되는 전립선암은 대부분 비전형적작은 꽈리증식증이 있었던 부위였다는 보고가 있지만,12,16 비전 형적작은꽈리증식증이 있었던 반대편 부위에서도 재생검 시행 시 17-27%에서 전립선암으로 진단되었다는 다른 보고 도 있어,5,6,8,16 최소한 비전형적작은꽈리증식증이 나온 부위 에 추가적인 생검 및 확장생검을 시행해야 할 것으로 생각 한다. 최근 저자들은 재생검을 하는 경우에는 전립선용적 에 상관없이 최소한 이전 병변부위의 추가생검을 포함하여 확장생검을 시행하고 있다.
전립선생검에서 비전형적작은꽈리증식증으로 진단된 경 우 이전의 보고들에 따르면 환자의 연령, 직장수지검사에 서 이상소견, 총 PSA에 대한 유리 PSA 비율, 전립선용적이 전립선암의 예측인자로 작용한다고 알려져 있다.12 또한 Scattoni 등22은 위에서 기술한 예측인자 중 비전형적작은꽈 리증식증으로 진단된 경우의 재생검에서 전립선용적만이 의미 있는 예측인자라고 주장하였다. 본 연구에서는 전립 선생검에서 비전형적작은꽈리증식증이 진단된 경우 전립 선암 검출률에 초점을 맞추어 환자의 연령, 혈청 전립선특 이항원, 전립선용적의 인자에 따른 차이를 알아보고자 하 였으며, 저자들의 경우에도 전립선용적이 작은 경우보다 큰 경우 재생검 후 전립선암 검출률이 낮은 것으로 나타났
240 Korean Journal of Urology vol. 50, 237-240, March 2009
다. 따라서 비전형적작은꽈리증식증으로 보고되어 재생검 이 필요한 경우 전립선용적이 클수록 포화생검 및 병변부 위를 포함한 확장생검이 전립선암의 검출률을 높이기 위해 필요하다고 생각되며, 향후 예측인자에 대한 추가적인 연 구가 필요하다고 생각한다.
결 론
본 연구의 결과 전립선생검을 통해 첫 번째 생검에서 비전 형적작은꽈리증식증으로 나온 214명 중 95명 (44.4%)의 환 자가 1회 이상의 재생검을 시행받았고, 이 중 36명 (37.9%) 이 전립선암으로 진단되었다. 전립선생검에서 비전형적작 은꽈리증식증으로 보고된 경우 첫 재생검 시 30.5%, 2회 재 생검 시 23.8%, 3회 재생검 시 40%에서 전립선암이 진단되 어, 반드시 이전 병변부위의 추가생검을 포함한 재생검이 필요할 것으로 생각되며, 전립선용적이 큰 경우는 재생검 시 12개 이상의 확장생검을 고려해야할 것으로 생각한다.
REFERENCES
1. Kang MY, Park JH, Kwak C, Paick JS, Kim HH. Transrectal needle biopsy of the prostate: the efficacy of a pre-biopsy enema. Korean J Urol 2008;49:248-51
2. Hyun CL, Lee HE, Kim HR, Lee HS, Park SY, Chung JH, et al. Pathological analysis of 1,000 cases of transrectal ultrasound guided systematic prostate biopsy: establishment of new sample processing method and diagnostic utility of immunohistochemistry. Korean J Pathol 2006;40:406-19 3. Iczkowski KA, Chen HM, Yang XJ, Beach RA. Prostate cancer
diagnosed after initial biopsy with atypical small acinar proliferation suspicious for malignancy is similar to cancer found on initial biopsy. Urology 2002;60:851-4
4. Fadare O, Wang S, Mariappan MR. Practice patterns of clinic- ians following isolated diagnoses of atypical small acinar proliferation on prostate biopsy specimens. Arch Pathol Lab Med 2004;128:557-60
5. Schlesinger C, Bostwick DG, Iczkowski KA. High-grade pro- static intraepithelial neoplasia and atypical small acinar proliferation: predictive value for cancer in current practice.
Am J Surg Pathol 2005;29:1201-7
6. Borboroglu PG, Sur RL, Roberts JL, Amling CL. Repeat bio- psy strategy in patients with atypical small acinar proliferation or high grade prostatic intraepithelial neoplasia on initial prostate needle biopsy. J Urol 2001;166:866-70
7. Cheville JC, Reznicek MJ, Bostwick DG. The focus of "aty- pical glands, suspicious for malignancy" in prostatic needle biopsy specimens: incidence, histologic features, and clinical follow-up of cases diagnosed in a community practice. Am J
Clin Pathol 1997;108:633-40
8. Iczkowski KA, Bassler TJ, Schwob VS, Bassler IC, Kunnel BS, Orozco RE, et al. Diagnosis of "suspicious for malig- nancy" in prostate biopsies: predictive value for cancer.
Urology 1998;51:749-58
9. Iczkowski KA, MacLennan GT, Bostwick DG. Atypical small acinar proliferation suspicious for malignancy in prostate needle biopsies: clinical significance in 33 cases. Am J Surg Pathol 1997;21:1489-95
10. Chan TY, Epstein JI. Follow-up of atypical prostate needle biopsies suspicious for cancer. Urology 1999;53:351-5 11. Renshaw AA, Santis WF, Richie JP. Clinicopathological cha-
racteristics of prostatic adenocarcinoma in men with atypical prostate needle biopsies. J Urol 1998;159:2018-22
12. Park S, Shinohara K, Grossfeld GD, Carroll PR. Prostate cancer detection in men with prior high grade prostatic intraepithelial neoplasia or atypical prostate biopsy. J Urol 2001;165:1409-14
13. Epstein JI. How should atypical prostate needle biopsies be reported? Controversies regarding the term ‘ASAP'. Hum Pathol 1999;30:1401-2
14. Thorson P, Vollmer RT, Arcangeli C, Keetch DW, Humphrey PA. Minimal carcinoma in prostate needle biopsy specimens:
diagnostic features and radical prostatectomy follow-up. Mod Pathol 1998;11:543-51
15. Epstein JI, Herawi M. Prostate needle biopsies containing pro- static intraepithelial neoplasia or atypical foci suspicious for carcinoma: implications for patient care. J Urol 2006;175:
820-34
16. Allen EA, Kahane H, Epstein JI. Repeat biopsy strategies for men with atypical diagnoses on initial prostate needle biopsy.
Urology 1998;52:803-7
17. Halushka MK, Kahane H, Epstein JI. Negative 34betaE12 stain- ing in a small focus of atypical glands on prostate needle biopsy:
a follow-up study of 332 cases. Hum Pathol 2004;35:43-6 18. Murphy WM. ASAP is a bad idea. Atypical small acinar
proliferation. Hum Pathol 1999;30:601
19. Brausi M, Castagnetti G, Dotti A, De Luca G, Olmi R, Cesinaro AM. Immediate radical prostatectomy in patients with atypical small acinar proliferation. Over treatment? J Urol 2004;172:906-8
20. Mancuso PA, Chabert C, Chin P, Kovac P, Skyring T, Watt WH, et al. Prostate cancer detection in men with an initial diagnosis of atypical small acinar proliferation. BJU Int 2007;99:49-52
21. Epstein JI, Potter SR. The pathological interpretation and significance of prostate needle biopsy finding: implication and current controversies. J Urol 2001;166:402-10
22. Scattoni V, Roscigno M, Freschi M, Briganti A, Fantini GV, Bertini R, et al. Predictors of prostate cancer after initial diagnosis of atypical small acinar proliferation at 10 to 12 core biopsies. Urology 2005;66:1043-7