제2형 당뇨병은 전세계적으로 많은 인구가 앓고 있으 며 당뇨병 치료약물들은 췌장의 인슐린 분비 이상, 간에 서의 포도당 생성 증가, 근육 및 말초조직의 포도당 흡 수 감소 등 여러 발병 원인에 대응하는 기전을 약효로 하여 다양하게 개발되어 왔다. 그러나 기존 혈당강하제 들의 치료 한계로 인하여 새로운 기전의 당뇨치료제 필 요성이 제기되었고 다양한 연구가 시행되고 있다. 최근 다양한 발병 인자들이 밝혀지고 있으며 이에 대응하는 새로운 당뇨병약의 개발이 이루어지고 있다. 그 중 dapagliflozin이 현재 국내에서“포시가 정 10 mg” 으로 출시되었으며 미국에서“Farxiga” , 유럽에서“Forxi- ga” 의 상품명으로 출시되어 운동과 식이요법을 병용하 는 제2형 성인 당뇨환자를 위한 혈당강하제로 쓰이고 있다. 본 리뷰에서는 기존의 당뇨병약과 더불어 새로운 당뇨병약의 약물학적 특징과 임상적인 치료 결과에 대 해 살펴보고자 한다.
1. 기존의 제2형 당뇨병약(Table 1, 2)
1)-4)1) Biguanides
현재 1
stline agent로 널리 사용되는 약물로서 인슐린 감작제로 표적조직에 의한 포도당 흡수 및 이용을 증가
시켜 인슐린 저항성을 감소시키며 sulfonylureas계 약 물과 달리 인슐린 분비를 촉진시키지 않는다. 주요 작 용기전은 간에서의 당 생성을 억제하고 위장관에서 당 흡수를 지연시키며 말초 조직의 당 이용을 증가시켜 혈 당강하작용을 나타내며, 종종 식욕감퇴를 유발하여 체 중감소 효과를 나타낸다. 주로 위장장애가 부작용으로 나타나며, 신부전, 간부전, 불안정 심부전, 젖산산증의 기왕력자, 임산부, 저산소증, 당뇨성 케톤산증이 있는 당뇨병 환자에게는 금기이다.
이 계열의 약물에는 metformin이 있다.
1)-4)2) Thiazolidinediones-Glitazones
인슐린 감작제인 thiazolidinedione 계열의 경구용 혈당강하제로 약물 그룹으로 peroxisome prolifera- tor-activated receptor-gamma (PPAR-γ ) 핵 수용 체를 활성화시킴으로써 지질과 포도당 대사에 관여된 gene product의 생성을 촉진시키며 인슐린의 췌장분 비를 증가시키지 않고도 target cell의 인슐린 반응을 증진시켜 혈당 강하작용을 나타낸다. 부작용으로는 저 혈당 증상은 유발하지 않으나 체중증가와 부종이 유발 될 수 있다. 부종은 체액저류를 일으키기 때문에 glita- zones은 심부전 환자에게 금기이다.
학술강좌
새로운 제2형 당뇨병약: Dapagliflozin
이민철
a, 윤현옥
a, b경상대학교 약학대학 약학과
a, 경상대학교 약학연구소
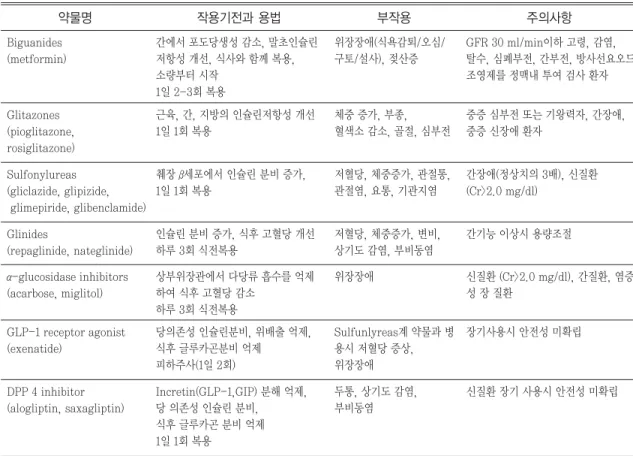
b약물명 작용기전과 용법 부작용 주의사항 Table 1. The characteristics of the existing antidiabetics
1),2),8),9)GFR 30 ml/min이하 고령, 감염, 탈수, 심폐부전, 간부전, 방사선요오드 조영제를 정맥내 투여 검사 환자 위장장애(식욕감퇴/오심/
구토/설사), 젖산증 간에서 포도당생성 감소, 말초인슐린
저항성 개선, 식사와 함께 복용, 소량부터 시작
1일 2-3회 복용 Biguanides
(metformin)
중증 심부전 또는 기왕력자, 간장애, 중증 신장애 환자
체중 증가, 부종, 혈색소 감소, 골절, 심부전 근육, 간, 지방의 인슐린저항성 개선
1일 1회 복용 Glitazones
(pioglitazone, rosiglitazone)
간장애(정상치의 3배), 신질환 (Cr>2.0 mg/dl)
저혈당, 체중증가, 관절통, 관절염, 요통, 기관지염 췌장 β세포에서 인슐린 분비 증가,
1일 1회 복용 Sulfonylureas
(gliclazide, glipizide, glimepiride, glibenclamide)
간기능 이상시 용량조절 저혈당, 체중증가, 변비,
상기도 감염, 부비동염 인슐린 분비 증가, 식후 고혈당 개선
하루 3회 식전복용 Glinides
(repaglinide, nateglinide)
신질환 (Cr>2.0 mg/dl), 간질환, 염증 성 장 질환
위장장애 상부위장관에서 다당류 흡수를 억제
하여 식후 고혈당 감소 하루 3회 식전복용 α-glucosidase inhibitors
(acarbose, miglitol)
장기사용시 안전성 미확립 Sulfunlyreas계 약물과 병
용시 저혈당 증상, 위장장애 당의존성 인슐린분비, 위배출 억제,
식후 글루카곤분비 억제 피하주사(1일 2회) GLP-1 receptor agonist
(exenatide)
신질환 장기 사용시 안전성 미확립 두통, 상기도 감염,
부비동염 Incretin(GLP-1,GIP) 분해 억제,
당 의존성 인슐린 분비, 식후 글루카곤 분비 억제 1일 1회 복용
DPP 4 inhibitor (alogliptin, saxagliptin)
약물명 장점 단점
Table 2. The pros and cons of the existing antidiabetics
1),2),8),9)Biguanides (Metformin) 식전혈당 감소, 가격 저렴, 체중감소 위장장애, 젖산증유발
Glitazones (pioglitazone, rosiglitazone) 식후혈당 감소, 저혈당증상 없음 체중 증가, 부종, 혈색소 감소, 골절, 심부전
GLP-1 receptor agonist (exenatide) 식후혈당 감소, 체중감소, 저혈당증상 없음 피하주사투여 Sulfonylureas
(gliclazide, glipizide, glimepiride, glibenclamide)
공복혈당 감소 저혈당, 체중증가, 관절통, 관절염, 요통,
기관지염 유발
Glinides
(repaglinide, nateglinide)
식후혈당 감소 저혈당, 체중증가, 변비, 상기도 감염, 부비동
염 유발, 매 식사마다 복용필요 α-glucosidase inhibitors
(acarbose, miglitol)
식후혈당 감소 저혈당증상 없음
위장장애, 매 식사마다 복용
DPP 4 inhibitor (alogliptin, saxagliptin)
체중감소, 저혈당증상 ,위장장애 없음 식사와 상관없이 복용가능
장기적인 안전성 미확립
이 계열의 약물로는 pioglitazone, rosiglitazone이
있다.
1)-4)3) Sulfonylureas
췌장의 β -cell에서 인슐린의 분비를 자극하고, 간세포 에서 포도당 생성을 저해하며, 말초 장기에서의 인슐린 에 대한 감수성을 증가시켜 즉각적인 혈당강하작용을 나타내는 인슐린 분비촉진제이다. Sulfonylureas계 약 물의 단점으로는 체중증가, 고인슐린혈증 및 저혈당증 이다.
이 계열의 약물로는 tolbutamide, glipizide, gly- buride, glimepiride, gliclazide가 있다.
1)-4)4) Meglitinides (Glinides)
Sulfonylureas계와 같이, 췌장의 인슐린 분비를 촉진 시켜 혈당을 조절하는 약물이다. Sulfonylureas계 약 물과 대조적으로 glinides계 약물은 신속한 발현과 짧 은 작용지속시간을 갖고 있으며 특히 식후에 일어나는 초기 인슐린 유리에 유효하다. 따라서 식후 글루코스 조절제로서 분류한다. 이들 약물은 sulfonylureas계 약물과 비슷한 부작용이 나타나지만 부작용 발생빈도 는 sulfonylureas계 약물보다 낮게 나타난다.
이 계열의 약물로는 repaglinide, nateglinide, mit- iglinide가 있다.
1)-4)5) α -glucosidase inhibitors
췌장의 α -amylase와 membrane bound intestinal α -glucosidase에 경쟁적이고 가역적인 억제제로 작용 하여 탄수화물, 이당류, 단당류의 가수분해를 지연시켜 포도당 흡수를 저해한다. 이 약물은 식후 고혈당 개선 에 충분한 효과를 얻을 수 없는 경우, 또는 식사요법,
운동요법에 추가하여 경구용 당뇨병약 또는 인슐린 제 제를 사용하고 있는 환자가 충분한 효과를 얻을 수 없 는 경우에 사용한다. 매 식사 전에 복용해야 하며 부작 용으로 위장관장애가 올 수 있으나 metformin처럼 저 혈당 증상이 부작용으로 나타나지 않는다.
이 계열의 약물로는 acarbose, miglitol, voglibose 가 있다.
1)-4)6) GLP-1 receptor agonist
Incretin 유사 약물 (glucagon-like peptide 1 or GLP-1)로 인슐린의 분비, β -cell 성장 및 복제를 증가 시키고, 위배출을 느리게 하며, 음식물 섭취를 감소시 킨다. 이 약물은 제2형 당뇨병 환자의 metformin, sulfonylurea 등 단독 또는 병용요법으로 혈당조절 효 과가 불충분한 경우에 병용 투여하며, 피하주사로 투여 한다.
이 계열의 약물로는 exenatide, liraglutide가 있다.
1)-4)7) Dipeptidyl peptidase-4 (DPP-4) inhibitors
GLP-1 receptor agonist와 달리 GLP-1의 분해를 억제하여 GLP-1의 작용을 향상시켜 혈당강하작용을 나타낸다. GLP-1 receptor agonist보다 효과는 덜하 지만 경구로 하루 1번 복용하는 장점이 있다.
이 계열의 약물로는 sitagliptin, vildagliptin, alogliptin, saxagliptin 등이 있다.
1)-4)2. 새로운 제2형 당뇨병약 (Table 3)
5)-19)1) 작용기전
Dapagliflozin은 신장에서 포도당 90% 이상을 재흡 수하는 역할을 하는 sodium-glucose co-trans-
약물명 작용기전과 용법 장점 부작용 주의사항
Table 3. The characteristics of dapagliflozin
8)-10)요로감염, 생식기 감염, 비인두염
장기적인 안전성 미확립 저혈당증상 없음, 혈압감소, 체중
감소, 식사와 상관없이 복용가능 SGLT2의 억제를 통한 당의 요배설
1일 1회(아침) 복용 Dapagliflozin
porter subtype 2 (이하, SGLT2)를 억제하여 혈중 포 도당을 요로 배설하게 함으로서 혈당강하작용을 나타 내는 SGLT2 inhibitor이다 (Fig. 1). Dapagliflozin은 sulfonylurea계 약물과 달리 인슐린에 의존하지 않고 혈당을 조절하며 소변으로 당을 배출시켜 체중감소 효 과도 나타낸다.
3),4),6)2) 약동학
Dapagliflozin은 정제 형태로 복용 시 흡수율이 높고 생체 이용률 78%이며 다른 약동학적 인자들이 음식에 의해 영향을 거의 받지 않는다. 혈장 최대 농도는 투여 2시간 이내 나타나고, 약물 반감기는 12.9시간이며 하 루 1회 투여가 추천된다. Dapagliflozin은 간에서 uri- dine 5’ -diphospho-glucouronosyltransferase 1-9 (UDP-glucuronosyltransferase 1-9, UGT1A9)에 의해 대사되어 비활성화가 된다. Dapagliflozin의 약 75%는 신장에 의해 배설되고, 나머지는 변에 의해 배 설이 되는데, 거의 비활성 대사체로 배설된다. Dapagli- flozin은 나이, 성별, 인종, 복용시간 등이 약동학에 크 게 영향을 미치지 않는다.
3),4),6)3) 상호작용
Dapagliflozin의 대사는 주로 UGT1A9에 의해 매개 되는 글루쿠로니드 접합을 통해 이루어지고 간의 CYP450을 억제하거나 유도하지 않는다. 따라서 dapagliflozin은 이러한 효소들에 의해 대사되는 약물 들과 병용투여 하더라도 약물의 대사에 영향을 끼치지
않을 것으로 예상된다.
5)-10)Dapagliflozin은 기존의 혈당강하제의 기전과 다른 기전으로 혈당강하작용을 나타내므로 기존의 당뇨병약 과 약물 상호작용은 없다. 다만, 인슐린 및 sulfony- lurea계 약물과 같은 인슐린 분비 촉진제는 저혈당을 일으킬 수 있기 때문에 dapagliflozin과 병용 투여시, 인슐린이나 인슐린 분비 촉진제의 용량을 줄여야 한 다.
5)-10)Dapagliflozin은 thiazide계와 loop계 이뇨제의 이뇨 작용을 증가시킬 수 있으며, 탈수 및 저혈압의 위험을 증가시킬 수 있다. 따라서 dapagliflozin 사용시 체액 량, 전해질을 모니터링 해야 한다.
5)-10)주로 단 회 투여 디자인을 이용한 건강한 피험자를 대 상으로 실시한 상호작용 연구에서, dapagliflozin은 metformin, pioglitazone, sitagliptin, glimepiride, hydrochlorothiazide, bumetanide, valsartan, rifampicin (다양한 활성 수송체 및 약물 대사 효소의 유도제)과 다른 유도제 (예, carbamazapine, pheny- toin, phenobarbital), mefenamic acid (UGT1A9의 저해제), digoxin (P-gp 기질)의 병용투여 시험결과 임 상적인 영향은 나타나지 않았다. 그리고 warfarin (S- warfarin, CYP2C9 기질)과의 상호작용 연구에서도 응 고효과에 영향을 주지 않았다.
5)-10)흡연, 식이, 천연물 의약품 및 알코올과의 상호작용이나 소아에 대한 임상 시험은 아직 연구되지 않았다.
4) 안전성
Dapagliflozin의 투여가 고위험군 환자, 즉 중증 신장 애, 소아, 임신 및 수유부에서의 안전성은 아직 확립되 지 않았다. 이 약물의 가장 중요한 부작용은 저혈당과 요로감염이다. 이 약물을 단독으로 사용할 경우에는 저 혈당 증상이 거의 나타나지 않으나 sulfonylurea계 약 물 또는 인슐린과 병용 시 저혈당 발생률이 증가한다.
Dapagliflozin을 복용하면 당이 소변을 통해 배설되며, 소변은 평균기준치보다 높은 당을 함유하게 되어 세균 증식이 쉬운 환경이 마련됨으로써 요로 감염이 발생할 수 있게 된다.
5)-10)또한, 비인두염과 여성에게 곰팡이균 에 의한 생식기 감염이 발생되기도 한다.
6)고령 환자의 경우 신기능 및 체액량 감소의 위험을 고
Fig. 1 Mechanism of SGLT2 inhibitor
20)려해야 한다. 고령 환자들은 이뇨제를 투여하고 있을 가능 성이 높기 때문에 75세 이상의 환자에게는 dapagliflozin 을 권장하지 않는다. 이 약물과 pioglitazone을 병용투 여 시 방광암의 발병 위험이 약간 증가하였다는 보고가 있어 사용에 주의를 해야 하며 방광암의 전력이 있는 환자나, 방광암 환자에게 dapagliflozin이 사용되어서 는 안된다.
5)-10)5) 역할 및 응용
Dapagliflozin의 단독요법과 병용요법에 대해서 비교 한 주요 대규모 임상시험은 다음과 같다 (Table 4). 단 독으로 사용한 경우 fasting plasma glucose (FPG) (24-28 mg/dL)과 oral glucose tolerance test (OGTT)(33-52 mg/dL)의 감소효과를 확인할 수 있었 다. 다른 계열의 당뇨 치료약을 단독 사용하였을 때와
Study Methods A1c reduction (% adjusted mean change from baseline)*
Other statistically significant
� findings Table 4. Large-scale comparative clinical trials of dapagliflozin
11)-19)Dapagliflozin monotherapy11)
24-week, placebo-controlled RCT485 treatment-naive patients
AM 2.5 mg: not statistically significant, AM 5 mg: -0.77% (P=0.0005), AM 10 mg: -0.89% (P<0.0001), Placebo: -0.23%
PM doses had similar reductions (-0.79% to -0.83%) (extrapolated data).
Patients with baseline, A1c $10% had mean change in A1c of -2.88% (for 5 mg) and -2.66% (for 10 mg) (extrapolated data)
FPG reductions:AM 2.5 mg: -15.2 mg/dL, AM 5 mg: -24.1 mg/dL, AM 10 mg: -28.8 mg/dL PM dose reductions (-26 to -30 mg/dL) (extrapolated data) Patients with baseline A1c $10%
had FPG reductions of -77 to -84 mg/dL. (extrapolated data)
Dapagliflozin monotherapy12)
24-week, double-blind, placebo-controlled RCT282 treatment-naive patients
5 mg: -0.82%, 2.5 mg: -0.72%, 1 mg: -0.68%, Placebo: 0.02%
(P<0.0001, for all doses)
FPG reductions: 1 mg: -11 mg/dL, 2.5 mg: -22 mg/dL, 5 mg: -28 mg/dL OGTT reductions (with all doses): -33 to -52 mg/dL
Dapagliflozin + metformin vs placebo + metformin13-14)
24-week, double-blind, placebo-controlled RCTE xtension study to 102 weeks 546 patients inadequately controlled on metformin monotherapy ($1,500 mg/day)
2.5 mg: -0.65% (P=0.0008), 5 mg: -0.67% (P<0.0001), 10 mg: -0.82% (P<0.0001), Placebo: -0.31%
At 102 weeks, reductions were maintained: -0.48% to -0.78%
FPG reductions: 5 mg: -26 mg/dL, 10 mg: -24 mg/dL
Dapagliflozin + metformin vs placebo + metformin15)
24-week double-blind, placebo-controlled RCT 182 patients inadequately controlled on metformin
10 mg: -0.39%,
Placebo: -0.10% (P<0.0001)
FPG reductions: 10 mg: -15 mg/dL
Dapagliflozin + glimepiride vs placebo + glimepiride16)
24 week double-blind, placebo-controlled RCT 597 patients inadequately controlled on SU ($ half the maximum recommended dose)
2.5 mg: -0.58%, 5 mg: -0.63%, 10 mg: -0.82%, Placebo: -0.13%
P<0.0001,
For all doses hypoglycemic episodes were more frequent in the dapagliflozin arm (6.9%-7.9% vs 4.8% placebo).
FPG reductions:5 mg: -21 mg/dL, 10 mg: -28 mg/dL
OGTT reductions (-32 to -35 mg/dL) were statistically signifi- cant for 5 mg and 10 mg.
Study Methods A1c reduction (% adjusted mean change from baseline)*
Other statistically significant
� findings
Dapagliflozin +insulin vs placebo + insulin17)
24-week, placebo-controlled RCT with blinded oral administration 808 patients inadequately controlled on insulin ($30 units/day) Mean daily insulin dose was 77.1 units/day, with 17% using basal insulin and 83% using sliding- scale
2.5 mg: -0.79%, 5 mg: -0.89%, 10 mg: -0.96%, Placebo: -0.39%
P<0.0001,
For all doses after 48 weeks, A1c reduction was maintained with all doses (-0.79% to -1.01%).
(P<0.001) Hypoglycemic episodes were 53.6% for dapagliflozin 10 mg vs 51.8% with placebo.
FPG reductions: 2.5 mg: -12 mg/dL, 5 mg: -20 mg/dL, 10 mg: -20 mg/dL At 48 weeks, FPG reduction was - 12 to -17 mg/dL.
Patients continued usual daily dose of insulin with titrations, and up to two existing oral antidiabetic drugs (.50% on existing orals, mostly metformin)
Dapagliflozin + pioglitazone vs placebo + pioglitazone18)
24 week, placebo-controlled RCT480 patients inadequately controlled on pioglitazone 30-45 mg/day
5 mg: -0.82% (P=0.0007), 10 mg: -0.97% (P<0.00001), Placebo: -0.42%
After 48 weeks, A1c reductions were maintained (-0.95% to -1.21%).
However, statistical tests were not performed.
FPG reductions:5 mg: -24.9 mg/dL, 10 mg: -29.6 mg/dL
Dapagliflozin + sitagliptin vs placebo + sitagliptin19)
24-week, placebo-controlled RCT451 patients inadequately controlled on sitagliptin 100 mg/day ± metformin $1,500 mg/day
Without metformin: 10 mg:
-0.5%, Placebo: -0.1% (P,0.0001) With metformin: 10 mg: -0.4%.
Placebo: 0.0% (P<0.0001) Patients with baseline A1c $8%
had mean change in A1c of -0.8%
compared to 0.0% (P<0.0001)
FPG reductions (combined ± metformin) 10 mg: -24.1 mg/dL, Placebo: 3.8 mg/dL
* Versus placebo
�Statistical significance at P < 0.05
Abbreviations: A1c, hemoglobin A1c; RCT, randomized controlled trial; AM, morning; PM, evening; FPG, fasting plasma glucose; OGTT, oral glucose tolerance test; vs, versus; SU, sulfonylureas
dapagliflozin을 병용하였을 때를 비교하면 dapa- gliflozin과 병용 시에 HbA1c 감소, FPG 감소, 체중 감소를 확인할 수 있었다.
7),11)-19)이 외에도 현재 장기적인 안전성에 대한 임상연구가 진행 중이다. 여러 대규모 임상연구를 통해 기존의 치 료에 대비하여 dapagliflozin이 다른 당뇨치료약과 마 찬가지로 효과가 있음이 입증되었고 새로운 작용기전 으로 기존의 약물치료요법에 추가될 수 있어 더욱 효과 적인 혈당 조절 효과를 나타낼 수 있을 것이다.
이러한 새로운 당뇨치료약의 임상적 도입은 환자의 측면에서 치료비용 및 치료선택의 폭을 넓혀 혈당조절 의 성공률을 상승시킬 수 있다는 이점을 가지고 있다.
하지만 아직 장기적 안전성에 대한 정보가 부족하기 때 문에 사용시 주의가 필요하다.
3. 결론
현재 혈당을 조절하기 위해서 여러 종류의 제2형 혈
당강하제가 국내에서 이미 사용되고 있다. Dapagli-
flozin은 기존에 적용되고 있던 기전이 아닌 새로운 기
전을 통해 혈당을 조절할 수 있고, 약동학적 변화가 적
으며, 기존의 당뇨병약이나 다른 약물들간의 상호작용
발생 가능성이 낮다는 장점이 있다. 그러나 pioglita-
zone과 병용 시에 방광암이 유발될 수 있다는 가능성
Table 4. Large-scale comparative clinical trials of dapagliflozin
11)-19)(continued)
이 제기되는 등 안전성 관련 문제나 약물학적 치료효과 에대한 임상적 근거가 부족하기 때문에 더 많은 연구들 을 통해 치료적 근거를 확립할 필요가 있다고 생각된 다.
참고문헌
1) Harve y, Ric hard A. : Lippinc otts’s Illustrated Review Pharmacology, 5th ed.
Lippincott Williams, Seoul, 301-315 (2012) 2) Terry Schwinghammer : Pharmacotherapy
Casebook: Patient Focused Approach, 8th ed. McGraw-Hill Professional, Seoul, 1255- 1302 (2011)
3) Kimsonline
�, http://www.kimsonline.co.kr 4) Micromedexsolutions
�, http://www.micro-
medexsolutions.com
5) List J.F., Woo V., Morales E., Tang W., Fiedorek F.T. : Sodium-glucose cotransport inhibition with dapagliflozin in type 2 dia- betes. Diabetes Care, 32(4), 650-657 (2009) 6) FDA
�, http://www.accessdata.fda.gov
/scripts/cder/drugsatfda
7) Sun Y.N., Zhou Y., Chen X., Che W.S., Leung S.W. : The efficacy of dapagliflozin combined with hypoglycaemic drugs in treating type 2 diabetes mellitus: meta- analysis of randomised controlled trials.
BMJ Open, 4(4), e004619 (2014)
8) Salvo M.C., Brooks A.D., Thacker S.M. : Patient considerations in the management of type 2 diabetes - critical appraisal of dapagliflozin. Patient Prefer Adherence, 22(8), 493-502 (2014)
9) Nair S.,Wilding J.P. : Sodium glucose cotransporter 2 inhibitors as a new treatment for diabetes mellitus. J Clin Endocrinol Metab, 95(1), 34-42 (2010)
10) S. Nair, F. Joseph, D. Ewins, J. Wilding, N. Goenka : From history to reality: sodi-
um glucose co-transporter 2 inhibitors - a novel therapy for type 2 diabetes mellitus.
Practical Diabetes, 27(7), 311-316 (2010) 11) Ferrannini E., Ramos S.J., Salsali A., Tang
W., List J.F. : Dapagliflozin in monothera- py in type 2 diabetes patients with inade- quate glycemic control by diet and exer- cise: a randomized, double-blind, placebo- controlled, phase 3 trial. Diabetes Care, 33(10), 2217-2224 (2010)
12) Bailey C.J., Iqbal N., T’ joen C., List J.F. : Dapagliflozin monotherapy in drug-naive patients with diabetes: a randomized- c ontrolled trial of low-dose range.
Diabetes Obes Metab, 14(10), 951-959 (2012)
13) Bailey C.J., Gross J.L., Pieters A., Bastien A., List J.F. : Effect of dapagliflozin in patients with type 2 diabetes who have inadequate glycaemic control with met- formin: a randomized, double-blind, plac e bo-c ontrolle d trial. Lanc e t, 375(9733), 2223-2233 (2010)
14) Clifford J. Bailey, Jorge L. Gross, Delphine Hennicken, Nayyar Iqbal, Traci A. Man- sfield, James F. List : Dapagliflozin add- on to metformin in type 2 diabetes inade- quately controlled with metformin: a ran- domized, double-blind, placebo-controlled 102-week trial. BMC Med, 11, 193 (2013) 15) Bolinder J., Ljunggren O, Kullberg J.,
Johansson L., Wilding J., Langkilde A.M., Sugg J., Parikh S. : Effects of dapa- gliflozin on body weight, total fat mass, and regional adipose tissue distribution in patients with type 2 diabetes mellitus with inadequate glycemic control on metformin.
J Clin Endocrinol Metab, 97(3), 1020-1031 (2012)
16) Strojek K., Yoon K.H., Hruba V., Elze M.,
Langkilde A.M., Parikh S. : Effect of dapagliflozin in patients with type 2 dia- betes who have inadequate glycaemic con- trol with glimepiride: a randomized, 24- week, double-blind, placebo-controlled trial. Diabetes Obes Metab, 13(10), 928- 938 (2011)
17) Wilding J.P., Woo V., Soler N.G., Pahor A., Sugg J., Rohwedder K., Parikh S. : Long-term efficacy of dapagliflozin in patients with type 2 diabetes mellitus receiving high doses of insulin. Ann Intern Med, 156(6), 405-415 (2012)
18) Rosenstock J., Vico M., Wei L., Salsali A., List J.F. : Effects of dapagliflozin, an SGLT2 inhibitor, on HbA(1c), body weight, and hypoglycemia risk in patients with type 2 diabetes inadequately controlled on pioglitazone monotherapy. Diabetes Care, 35(7), 1473-1478 (2012)
19) Jabbour S.A., Hardy E., Sugg J., Parikh S.
: Dapagliflozin is effective as add-on therapy to sitagliptin with or without metformin: a 24 week, multicenter, ran- domized, double-blind, placebo-controlled study. Diabetes Care, 37(3), 740-750 (2014)
20) Nature Reviews Drug Discovery
�, http://
www.nature.com
문 제