Plasmacytomas, otherwise known as solitary myelo- mas, are malignant neoplasms arising from a single clone of plasma cells. They are commonly found in the axial skeleton; especially in the spine, pelvis, and skull and are characterized as expansile osteolytic bone le-
sions on radiography (1).
The MR imaging findings of plasmacytoma or multi- ple myeloma located in the spine has been well de- scribed, but nonspecifically (2, 3). Plasmacytomas usual- ly present as a marrow-replacing process with variable signal intensity on T1-weighted images and high signal intensity on T2-weighted images (1-4). Therefore, it is often indistinguishable from other marrow-replacing processes such as lymphoma or metastasis.
For extraspinal lesions, the MR imaging features of plasmacytoma were rarely reported and, to our knowl-
MR Imaging Features of Extraspinal Plasmacytoma of Bone
1Mi Hye Yu, M.D., Sung Hwan Hong, M.D., Ja-Young Choi, M.D., Jae Sung Myung, M.D., Su Jin Kim, M.D., Jung-Ah Choi, M.D., Heung Sik Kang, M.D.
1Department of Radiology and the Institute of Radiation Medicine, Seoul National University College of Medicine
Received April 21, 2009 ; Accepted June 7, 2009
Address reprint requests to : Sung Hwan Hong, M.D., Department of Radiology, Seoul National University College of Medicine, 101 Daehang- ro, Chongno-gu, Seoul, 110-744, Korea.
Tel. 82-2-2072-3217 Fax. 82-2-743-6385 E-mail: [email protected]
Purpose: To describe the MR imaging features of extraspinal plasmacytoma of the bone.
Materials and Methods: MR images of 10 lesions in 10 patients (3 men, 7 women; age range, 49-69 years) with extraspinal plasmacytoma of the bone were retrospectively reviewed. The bones involved included the pelvic bone (n = 7), humerus (n = 1), tibia (n = 1), and clavicle (n = 1). Signal intensity, contrast enhancement pattern, cortical bone abnormality, and surrounding bone marrow edema were analyzed.
Results: Compared to a muscle signal, the T1-weighted MR images showed either ho- mogeneous high (n = 9) or iso (n = 1) signal intensity. The gadolinium-enhanced T1- weighted images showed homogeneous enhancement (n = 9), with only one huge plasmacytoma that has a central nonenhancing area. Cortical thinning and expansion was seen in all the lesions, while cortical penetration was apparent in 5 lesions. Also, in 5 lesions, serrated endosteal erosions were demonstrated. In all cases, perilesional bone marrow edema was not observed.
Conclusion: At MR imaging, extraspinal plasmacytoma of the bone has a characteris- tic homogeneous high signal intensity on a T1-weighted image. Other remarkable MR features include bone expansion with or without focal cortical penetration and serrat- ed endosteal erosion.
Index words :Plasmacytoma
Magnetic resonance (MR) Bone and bones
edge, most of the reported literature was limited to sin- gle case reports (5-7). The purpose of this study was to describe the MR imaging findings of extraspinal plasma- cytoma of the bone.
Materials and Methods
We searched the pathological and radiological records of all patients who were diagnosed with plasmacytoma at our institution from January 2000 to December 2008.
From these, we chose the patients with a lesion in the extremities or pelvic bone and who underwent MR
imaging. Finally, 10 patients (3 men, 7 women; mean age, 60 years; age range, 49-69 years) with pathological- ly proven extraspinal plasmacytoma of the bone were selected for this study. The bones involved included the pelvic bone (n = 7), humerus (n = 1), tibia (n = 1), and clavicle (n = 1).
The MRI systems and pulse sequences varied, but all MR imaging was performed using 1.0-T or 1.5-T ma- chines. The sequences consisted of T1-weighted images,
C D
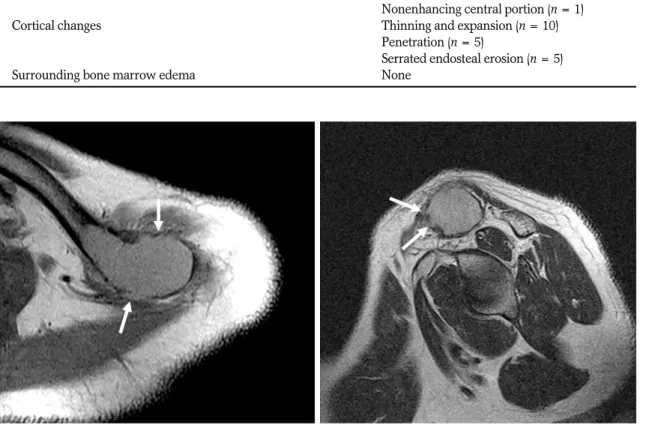
Fig. 1. A 65-year-old female with plasmacytoma in the right proximal humerus.
A. Plain radiograph shows an expansile osteolytic lesion with cortical thinning (arrows) in the right proximal humerus.
B. A coronal fat-suppressed T2-weighted image shows a well-demarcated high signal-intensity lesion in the right proximal humerus with no accompanying perilesional bone marrow edema. Soft tissue edema (arrows) associated to pathologic fracture (not shown here) is observed in the periphery of the humerus.
C. An axial T1-weighted image shows a slightly high signal-intensity lesion relative to adjacent muscles. Serrated endosteal ero- sions (arrows) in the lateral cortex of the humerus are also observed.
D. Axial gadolinium-enhanced fat-suppressed image shows homogeneous enhancement within the tumor. Serrated endosteal ero- sions (black arrows) and surrounding soft tissue enhancement (white arrows), more likely related to pathologic fracture, were ob- served.
A B
T2-weighted images, and gadolinium-enhanced T1- weighted images with or without fat suppression.
Moreover, the imaging planes included axial and at least one longitudinal plane in all the patients.
An experienced musculoskeletal radiologist retrospec- tively reviewed the MR images for characteristic mor- phologic features including signal intensity on T1- and T2-weighted images, gadolinium-enhancement patterns, cortical change of the lesion, presence of perilesional bone marrow edema (surrounding bone marrow edema of low signal intensity on T1-weighted images and high signal intensity on T2-weighted images), and surround- ing soft tissue edema (soft tissue abnormality of high sig- nal intensity on T2-weighted images and/or soft tissue enhancement on gadolinium enhanced T1-weighted im- ages).
The signal intensity of plasmacytoma was qualitative- ly compared with that of muscle on T1-weighted images and we observed a low, iso, or high signal intensity.
Moreover, the cortical change, cortical thinning, expan- sion, penetration, or serrated endosteal erosion were an-
alyzed and recorded. Cortical penetration was defined as a focal cortical discontinuity, whereas serrated en- dosteal erosion was defined as the saw tooth-like ap- pearance of endosteal erosion.
Results
The MR imaging findings of 10 lesions are summa- rized in Table 1. All 10 lesions showed high signal inten- sity on T2-weighted MR images, and either homoge- neous high (n = 9) or iso (n = 1) signal intensity on T1- weighted MR images compared with muscle signal in- tensity (Figs. 1-3). All the lesions had homogeneous en- hancement on the gadolinium-enhanced T1-weighted images (Fig. 1D, 3B) except for one huge plasmacytoma, which appeared to have a central nonenhancing necrot- ic area.
The MR imaging showed cortical thinning and expan- sion in all the lesions (Figs. 1-3). Among them, cortical penetration was apparent in 5 of the 10 patients (50%) (Figs. 2, 3). Endosteal erosion with a serrated appear-
Table 1. Summary of MR Imaging Findings of Extraspinal Plasmacytoma (n = 10)
Signal intensity on T1-weighted images High (n = 9), Iso (n = 1) Signal intensity on T2-weighted images High (n = 10)
Gadolinium enhancement Homogeneous enhancement (n = 9)
Nonenhancing central portion (n = 1)
Cortical changes Thinning and expansion (n = 10)
Penetration (n = 5)
Serrated endosteal erosion (n = 5)
Surrounding bone marrow edema None
A B
Fig. 2. A 54-year-old male with plasmacytoma in the left clavicle
A. An axial T1- weighted image shows an expansile mass (arrows) with homogeneous high signal intensity in the left distal clavicle.
B. An oblique sagittal T2-weighted image shows expansile bone lesion with focal cortical penetrations (arrows) in the left clavicle.
ance was demonstrated in 5 lesions (50%) (Fig. 1).
Moreover, one of the 10 lesions had perilesional bone marrow edema and the 5 lesions with cortical penetra- tion revealed accompanying soft tissue edema.
Discussion
In our study, most cases of extraspinal plasmacytoma of the bone demonstrated relatively high signal intensity on T1-weighted images compared with muscle signal in- tensity. Solitary plasmacytoma of the bone was known to have a similar signal intensity to muscle on T1- weighted images and spinal multiple myeloma is of sim- ilar or higher signal intensity to muscle signal intensity (2, 3). The difference in signal intensity between our study and previous studies could be a attributed to im- proved tissue contrast of the MR imaging. This high sig- nal intensity on T1-weighted images was found in some reports about primary lymphoma of the bone as well as osseous metastasis from renal cell carcinoma and was considered to have likely been attributed high cellularity and hypervascularity (8-10). We believe that plasmacy- toma has the high signal intensity on T1-weighted im- ages for the same reason.
Another MR imaging feature of extraspinal plasmacy- toma was cortical expansion with or without focal corti- cal penetration. These cortical changes may suggest an intermediately aggressiveness tumor, which grows nei- ther too slowly nor too rapidly. A periosteal reaction and surrounding soft tissue edema were observed in 5 pa- tients, however we could hardly determine whether they were part of the tumor’s natural processes or the
result of a pathologic fracture. Even more, it was diffi- cult to distinguish a pathologic fracture from cortical penetration in the 5 patients with cortical disruption.
Because of these features we were not able to definitive- ly identify soft tissue edema or enhancement around the plasmacytomas.
One of the remarkable MR imaging features of plas- macytoma was the serrated endosteal erosion. This ap- pearance resembles the undermining osteoclastic re- sorption of cortical bone in renal osteodystrophy, lead- ing to a highly irregular endosteal surface and spongio- sation of the cortical bone (11). A destructive bone lesion in plasmacytomas generally begins in the medullary cavity, moves on to erode the cancellous bone, and fi- nally, progressively destroys the cortical bone. The bone resorption results from the secretion of certain cytokines (e.g., IL-1 , tumor necrosis factor, IL-6) by myeloma cells (12). We postulate that the serrated endosteal ero- sion in plasmacytoma is caused by the local effect of these substances, which in turn facilitate osteoclast-me- diated bone resorption (13). We also assume that this ap- pearance is associated with the intracortical canal sys- tem, especially Volkman’s canals.
Major et al. (14) proposed that the ‘mini brain’appear- ance is a characteristic MR imaging features of plasma- cytoma in the spine. They suggested that the thickened cortical struts are a secondary compensatory reponse of cortex to a combination of bony destruction. Recently, Subhas et al. (7) reported the ‘mini brain’appearance of plasmacytoma in the proximal femur as a first report outside of the spine. In our series, however, we could not identify the characteristic ‘mini brain’sign of plas-
A B
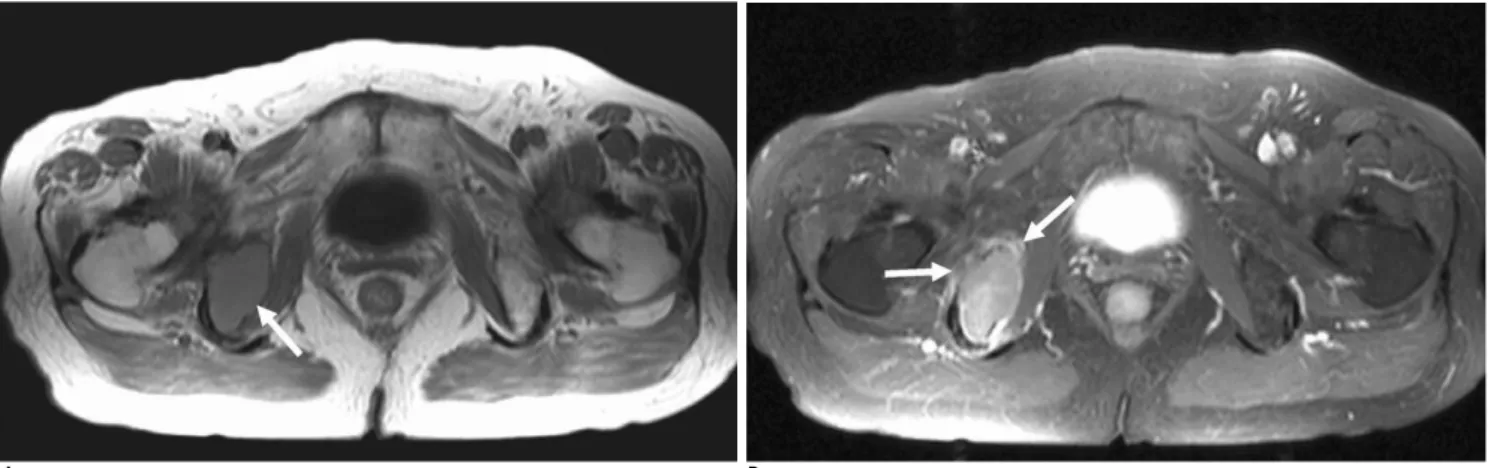
Fig. 3. A 76-year-old female with plasmacytoma in the right ischium.
(A) An axial T1- weighted image shows an expansile mass with homogeneous high signal intensity (arrow) in the right ischium (B) An axial gadolinium-enhanced fat-suppressed image shows homogeneous enhancement of the lesion and surrounding soft tis- sue enhancement (arrows) at the focal cortical penetration regions.
macytoma in the extraspinal lesions.
Extraspinal plasmacytoma did not show perilesional bone marrow edema in this study. Tumorigenic bone marrow edema is secondary to direct capillary trauma from trabecular destruction, with the release of intravas- cular fluid and associated hemorrhage (15). Another re- port proposed that peritumoral edema was caused by chemical mediators and is significantly correlated with prostaglandin levels of primary bone tumor (16). The ab- sence of perilesional bone marrow edema in extraspinal plasmacytoma is supposed to be attributable to the less aggressive nature of the tumor and absent or little prostaglandin production. This characteristic could be another differential feature which excludes other benign or malignant bone tumors showing perilesional bone marrow edema.
In summary, high signal intensity on T1-wighted im- ages, expansile osteolytic lesions, with or without focal cortical penetration, and serrated endosteal erosion, are the common MR findings of extraspinal plasmacytoma of the bone and does not accompany surrounding bone marrow edema. These findings can be helpful to differ- entiate plasmacytomas from other tumors in the ex- traspinal skeleton.
References
1. Resnick D. Plasma cell dyscrasias and dysgammaglobulinemias. In:
Resnick D. Diagnosis of bone and joint disorders, 4th ed.
Philadelphia: Saunders, 2002:2188-2216
2. Moulopoulos LA, Dimopoulos MA, Weber D, Fuller L, Libshitz HI, Alexanian R. Magnetic resonance imaging in the staging of solitary plasmacytoma of bone. J Clin Oncol 1993;11:1311-1315 3. Libshitz HI, Malthouse SR, Cunningham D, MacVicar AD,
Husband JE. Multiple myeloma: appearance at MR imaging.
Radiology 1992;182:833-837
4. Moulopoulos LA, Dimopoulos MA. Magnetic resonance imaging of the bone marrow in hematologic malignancies. Blood 1997;90:2127-2147
5. Kosaka N, Maeda M, Uematsu H, Matsumine A, Koshimoto Y, Itoh H. Solitary plasmacytoma of the sacrum. Radiologic findings of three cases. Clin Imaging 2005;29:426-429
6. Ly JQ, Sandiego JW, Beall DP. Plasmacytoma of the proximal humerus. Clin Imaging 2005;29:367-369
7. Subhas N, Bauer TW, Joyce MJ, Sundaram M. The “Mini brain”
appearance of plasmacytoma in the appendicular skeleton. Skeletal Radiol 2008;37:771-774
8. Negendank WG, al-Katib AM, Karanes C, Smith MR.
Lymphomas: MR imaging contrast characteristics with clinical- pathologic correlations. Radiology 1990;177:209-216
9. Mulligan ME, McRae GA, Murphey MD. Imaging features of pri- mary lymphoma of bone. AJR Am J Roentgenol 1999;173:1691- 1697
10. Choi JA, Lee KH, Jun WS, Yi MG, Lee S, Kang HS. Osseous metas- tasis from renal cell carcinoma: “flow-void” sign at MR imaging.
Radiology 2003;228:629-634
11. Krempien B. Bone modeling processes at the endosteal surface of human femora. Scanning electron microscopical studies in normal bone and in renal osteodystrophy. Virchows Arch A Pathol Anat Histol 1979;382:73-88
12. Aster JC. The hematopoietic and lymphoid system. In: Kumar V.
Robbins basic pathology. 8th ed. Philadelphia: Saunders, 2007:453- 456
13. Mitsiades CS, Mitsiades N, Munshi NC, Anderson KC. Focus on multiple myeloma. Cancer Cell 2004;6:439-444
14. Major NM, Helms CA, Richardson WJ. The “Mini brain”: plasma- cytoma in a vertebral body on MR imaging. AJR Am J Roentgenol 2000;175:261-263
15. O’Hare A, Shortt C, Napier N, Eustace SJ. Bone marrow edema:
Patterns and clinical implications. Semin Musculoskelet Radiol 2006;10:249-257
16. Yamamura S, Sato K, Sugiura H, Katagiri H, Ando Y, Fukatsu H, et al. Prostaglandin levels of primary bone tumor tissues correlate with peritumoral edema demonstrated by magnetic resonance imaging. Cancer 1997;79:255-261
대한영상의학회지 2009;61:257-262
척추 외 골에서 발생한 형질세포종의 자기공명소견1
1서울대학교병원 영상의학과
유미혜∙홍성환∙최자영∙명재성∙김수진∙최정아∙강흥식
목적: 이 연구에서는 척추 외 골에 발생한 형질세포종의 자기공명영상 소견을 알아보고자 하였다.
대상과 방법: 척추를 제외한 사지골이나 골반뼈에 발생한 형질세포종으로 진단된 환자 10명(남녀비 = 3:7, 49-69 세)을 대상으로 하여 자기공명영상 소견을 후향적으로 분석하였다. 병변의 위치는 골반뼈(n = 7), 상완골(n = 1), 경골(n = 1), 그리고 쇄골(n = 1)이었다. 자기공명영상에서 병변의 신호강도, 조영증강 유형, 피질골의 이상, 그 리고 골수부종 동반 여부 등을 분석하였다.
결과: 근육의 신호강도와 비교하였을 때, T1 강조영상에서 높거나(n = 9) 또는 동일하고(n = 1) 균질한 신호강도 를 보였다. 조영증강 후 T1 강조영상에서는 9개의 병변에서 균질한 조영증강을 보였고, 1개의 병변에서 내부에 조 영증강되지 않는 괴사 부위가 있었다. 모든 병변에서 피질골이 얇아졌고 피질골의 팽창을 보였으며 5개(50%)의 병 변에서는 부분적으로 피질골을 뚫고 나가는 모양을 보였다. 이와 함께 톱니바퀴 모양의 골내막 미란을 5개(50%)의 병변에서 볼 수 있었다. 모든 병변에서 병변 주변의 골수 부종은 보이지 않았다.
결론: 자기공명영상에서 척추 외 골의 형질세포종은 T1 강조영상에서 특징적인 균질한 고 신호강도를 보이며, 골피 질 관통이나 톱니바퀴 모양의 골내막 미란을 동반하는 팽창성 골병변으로 나타나는 경우가 많다.