pISSN: 0378-6471 eISSN: 2092-9374
http://dx.doi.org/10.3341/jkos.2013.54.11.1700
= 증례보고 =
망막혈관종성증식 환자에서 유리체강내 항혈관내피세포성장인자 주입술의 12개월 임상결과
김덕배1⋅김재휘2⋅정성헌2⋅이태곤2⋅김종우2⋅김철구2⋅조성원2⋅이동원2⋅한정일2 밝은안과21병원1, 건양대학교 의과대학 김안과병원 안과학교실2
목적: 항혈관내피세포성장인자를 이용하여 망막혈관종성증식을 치료한 12개월 임상 결과를 보고하고자 한다.
대상과 방법: 망막혈관종성증식으로 진단 후 유리체강내 항혈관내피세포성장인자 주입술로 치료받은 33안(33명)을 대상으로 후향적 의무기록 분석을 시행하였다. 진단 후 1개월 간격으로 3회의 주사를 시행하였고, 이후에는 재발하는 경우 추가 치료를 시행하였다.
치료 전 및 첫 번째 주사 후 3, 6, 12개월에 최대교정시력을 측정하였고, 이들 값을 서로 비교하였다.
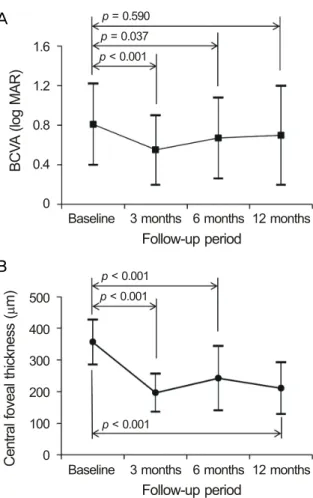
결과: 12개월 동안 평균 4.2 ± 1.7회의 주입술이 시행되었다. 치료 전 및 첫 번째 주사 후 3, 6, 12개월에 측정한 평균 최대교정시력은 각각 0.76 ± 0.49, 0.55 ± 0.35, 0.67 ± 0.41 및 0.70 ± 0.50으로, 첫 번째 주사 후 3개월 및 6개월에 측정된 시력은 치료 전보다 유의하게 호전된 결과를 보였으나(p<0.001, p=0.037), 12개월에 측정된 시력은 유의한 차이가 없었다(p=0.590). 12개월의 추적관찰 기간 동안 시력이 0.2 logMAR (logarithm of minimal angle of resolution) 이상 호전된 환자는 13명(39.4%)이었으며, 16명(48.5%)의 경우 비교적 안정적인 시력(<0.2 logMAR 이내의 변화)을 유지하였다.
결론: 항혈관내피세포성장인자 치료는 대부분의 망막혈관종성증식 환자에서 황반 두께를 정상화시키고 시력을 호전시키거나 유지시 키는 데 효과적인 방법으로 생각된다.
<대한안과학회지 2013;54(11):1700-1707>
■Received: 2013. 6. 21. ■ Revised: 2013. 9. 7.
■Accepted: 2013. 10. 28.
■Address reprint requests to Jae Hui Kim, MD
Kim’s Eye Hospital, #136 Yeongsin-ro, Yeongdeungpo-gu, Seoul 150-034, Korea
Tel: 82-2-2671-7665, Fax: 82-2-2671-6359 E-mail: [email protected]
망막혈관종성증식은 삼출성 연령관련환반변성의 일종으 로 망막-망막 혹은 망막-맥락막 혈관의 문합이 특징인 질 환이다.1-4망막혈관종성증식은 전체 삼출성 연령관련환반 변성의 약 5-20% 정도를 차지하는데,2-4 다른 종류의 삼 출성 연령관련환반변성에 비해 예후가 나쁘며 양안성으로 발생하는 경우가 많은 것으로 알려졌다.1,5,6
유리체강내 항혈관내피세포성장인자 주입술은 최근 삼 출성 연령관련환반변성의 치료에 가장 널리 이용되고 있는 효과적이고 안전한 방법이다.7-12기존의 연구들에 따르면, 삼출성 연령관련환반변성으로 진단된 환자들에게 유리체강 내 항혈관내피세포성장인자 주입술을 1개월 간격으로 계속 시행하거나 1개월 간격으로 추적관찰하면서 삼출이 재발할 때마다 바로 치료를 시행하면, 많은 경우에서 시력이 호전 되거나 최소한 더 악화되지 않는 것으로 나타났다.7,8 그러 나 실제 임상현장에서는 삼출성 연령관련환반변성 환자들 에게 1개월 간격으로 주사치료를 지속하거나 혹은 1개월
간격의 정기적 추적관찰은 어려운 경우가 많다. 반면에 초 기 치료가 성공적으로 이루어져 황반부의 삼출이 소실된 경우에는 더 이상의 주사 치료를 시행하지 않고 2개월 이상 의 비교적 긴 간격을 두고 외래 추적관찰을 시행하는 경우 가 많다. 이러한 실제임상경험을 바탕으로 한 연구들의 경 우에는 더 많은 횟수의 치료와 추적관찰을 자주 시행한 초 기 연구들에 비해 시력 예후가 좋지 않은 경향이 있는 것으 로 알려졌다.10-12
해외 연구자들의 보고에 따르면 망막혈관종성증식 환자 를 대상으로 유리체강내 항혈관내피세포성장인자 주입술을 시행하면, 상당수 안에서 시력이 유지 혹은 개선되는 것으 로 나타났다.13-17그러나 ‘이러한 연구 결과가 국내 환자를 대상으로 한 실제 임상에서 그대로 재현될 수 있을 것인 가?’라는 물음에 대해서는 아직 완전한 결론이 내려져 있지 않은 상태이다. 망막혈관종성증식으로 진단된 국내 환자를 대상으로 한 연구의 경우 7안을 대상으로 유리체강내 항혈 관내피세포성장인자 주입술을 시행한 후 평균 약 8.4개월 경과관찰 한 Kang et al18의 연구, 10안을 대상으로 광역학 치료와 유리체강내 항혈관내피세포성장인자 주입술 병합요 법을 시행한 후 12개월 경과관찰 한 Lee et al19의 연구, 1 단계 망막혈관종성증식으로 진단된 9안을 광역학치료, 국 소레이저, 유리체강내 트리암시놀론 주입술 등 다양한 방법
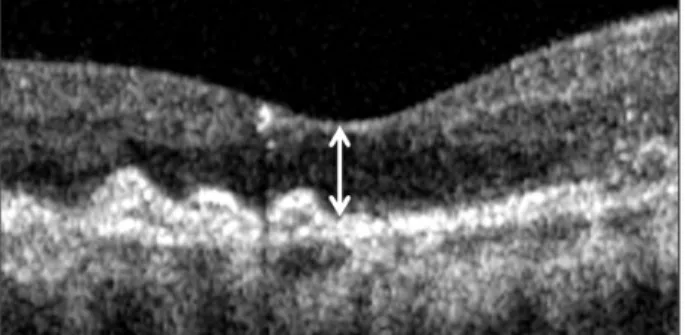
Figure 1. Central foveal thickness (double-head arrow) was
defined as the vertical distance between internal limiting mem- brane and retinal pigment epithelium at foveal center based on optical coherence tomography image centered at the center of the fovea.으로 치료한 후 평균 25개월 경과관찰한 Lee and Lee20의 연구 및 9안을 대상으로 광역학치료를 시행한 후 평균 17 개월 경과관찰한 Byeon et al21의 연구가 보고되어 있으나 다수의 망막혈관종성증식 환자를 대상으로 유리체강내 항 혈관내피세포성장인자 주입술 단일요법을 시행 후의 장기 임상결과는 아직 국내에 보고된 바 없다. 본 연구에서는 망막혈관종성증식으로 진단 받고 유리체강내 항혈관내피 세포성장인자 주입술을 시행 받은 환자들의 12개월 임상 결과를 알아보고자 한다.
대상과 방법
2010년 1월부터 2012년 1월까지 망막혈관종성증식으로 유리체강내 항혈관내피세포성장인자 주입술을 시행 받고 1 년 이상 경과관찰된 환자를 대상으로 후향적 의무기록 분 석을 시행하였다. 환자를 대상으로 최대교정시력을 측정하 고, 세극등을 이용한 안저검사, 형광안저혈관조영 및 인도 시아닌그린 혈관조영술(HRA-2; Heidelberg Engineering, Dossenheim, Germany)을 시행하였으며, 스펙트럼 도메 인 빛간섭단층촬영(Spectral OCT/SLO®; OTI Ophthalmic Technologies Inc. Miami, FL)을 시행하였다. 비록 황반하 출혈이 동반된 삼출황반변성에서도 유리체강내 항혈관내피 세포성장인자 주입술이 도움이 될 수 있음을 보여준 연구 들이 발표되어 있으나22-24일반적으로 황반하 출혈이 동반 된 경우 그렇지 않은 경우에 비해 예후가 더 좋지 않은 것 으로 알려졌다.25,26따라서 본 연구에서는 중심와를 침범한 3 유두직경크기 이상의 망막하 출혈이 동반된 경우 연구에 서 제외하였다. 망막혈관종성증식이 아닌 다른 종류의 삼출 성 황반변성에서도 질환이 진행된 경우 망막-맥락막 문합 이 나타날 수 있는 것으로 알려졌다.27따라서 황반중심에 지도모양 위축이나 원반형 반흔이 관찰되는 경우 또는 증
상 발생 후 6개월 이상 경과한 경우 연구에서 제외하였다.
증식당뇨망막병증, 망막혈관폐쇄가 관찰된 경우, 황반원공 이나 망막전막 등 황반미세구조와 시기능에 영향을 미칠 수 있는 기타 유리체망막 질환이 동반된 경우에는 연구에 서 제외하였다. 이전에 유리체망막 수술을 시행 받은 경우 혹은 이전에 삼출성 연령관련황반변성으로 진단받고 치료 를 시행 받은 경우 역시 연구에서 제외하였다. 양안에 망막 혈관종성증식이 발생한 경우 먼저 발병한 한 쪽 눈만 연구 에 포함하였다.
인도시아닌그린 혈관조영술 결과는 2명의 전문의가 함께 판 독하였으며, 특징적인 망막-망막 혹은 망막-맥락막 문합이 발견되는 경우 망막혈관종성증식으로 진단하였고, Yannuzziet al1이 정한 기준에 따라 1형, 2형, 3형으로 각각 구분하였 다. 중심망막두께는 빛간섭단층촬영 결과를 이용하여 중심 와 위치에서 내경계막으로부터 망막색소상피까지의 거리를 수직으로 측정하였다(Fig. 1).
유리체강내 주입술은 외래 수술실에서 시행되었고, 시술 전 0.5% proparacaine (Alcaine®, Alcon)을 점안한 뒤 1.25% 혹은 5% povidone iodine을 시술 할 눈에 점안하고 속눈썹을 포함하여 눈 주위를 닦았다. 개검기를 끼우고 생 리식염수로 충분히 세척한 뒤 주사기의 바늘 끝이 눈꺼풀 가장자리나 속눈썹에 닿지 않도록 주의하면서 각막 윤부에 서 3.0 mm 혹은 3.5 mm 하측 사분면 혹은 상측 사분면에 30게이지 일회용 바늘을 이용하여 0.05 cc의 ranibizumab (Lucentis®, Genentech, USA) 혹은 bevacizumab (Avastin®, Genentech, USA)을 주사하였다. 모든 환자들은 초기 치료 로 1개월 간격으로 3회의 유리체강내 ranibizumab 주입술 을 시행 받았다. 이후, 망막내액과 망막하액이 소실되고 중 심망막두께가 250 μm 이하로 정상화된 경우에는 추가적인 주사 치료를 시행하지 않고 질병의 상태에 대한 의사의 판 단과 환자의 사정을 종합적으로 고려하여 1-4개월 간격으 로 경과관찰하였다. 경과관찰기간 동안 내원 시마다 황반부 빛간섭단층촬영을 시행하였으며, 형광안저혈관조영술은 의 사의 판단에 따라 시행하였다. 빛간섭단층촬영에서 망막하 출혈, 망막하액, 망막내액의 재발과 함께 중심망막두께가 증가하는 경우 유리체강내 ranibizumab 혹은 bevacizumab 추가 주입술을 고려하였는데, 형광안저혈관조영술에서의 누출이 뚜렷하게 나타나면서 시력의 저하가 동반된 경우 즉시 주입술을 시행하였으며, 누출이 뚜렷하지 않으면서 시 력의 변화가 없는 경우 1개월 경과관찰하며 망막두께가 지 속적으로 증가하거나, 누출 양상이 보다 뚜렷해지거나 시력 이 저하되는 경우 주입술을 시행하였다.
진단 시 및 첫 번째 주사 후 3개월, 6개월 및 12개월의 최대교정시력과 중심망막두께를 측정하였다. 시술 전 측정
Table 1. Characteristics of 33 included eyes (33 patients) with
retinal angiomatous proliferationCharacteristics
Age (years) 75.2 ± 6.1
Sex (n, %)
Male 5 (15.2)
Female 28 (84.8)
Classification (n, %)
Type 1 12 (36.4)
Type 2 14 (42.4)
Type 3 7 (21.2)
Best-corrected visual acuity (log MAR) 0.76 ± 0.49 Central foveal thickness (μm) 356.8 ± 70.9 No. of anti-VEGF injections 4.2 ± 1.7
No. of hospital visit 7.3 ± 0.9
Values are presented as mean ± SD.
SD = standard deviation; VEGF = vascular endothelial growth factor; log MAR = logarithm of minimal angle of resolution.
A C1
B C3
C2
C4
Figure 2. Fundus photography (A), indocyanine green angiography (B), and optical coherence tomography (C) im-
ages in an eye with retinal angiomatous proliferation. Arrow (B) on indocyanine green angiography image indicates retinal angiomatous proliferation lesion. Optical coherence tomography images showing macular microstructure be- fore treatment (C1) and 3 months (C2), 8 months (C3), and 12 months (C4) after the first intravitreal anti-vascular en- dothelial growth factor injection. Recurrence of exudation was noted at 8 months following the first treatment. The best-corrected visual acuity measured before treatment was 20/40. The visual acuity was improved to 20/30 after three monthly injections, but deteriorated to 20/60 after the recurrence of exudation. At 12-month after the first treat- ment, the visual acuity was measured as 20/40.한 값들을 시술 후 각 시기에 측정한 값과 서로 비교하였다.
최대교정시력은 통계분석을위해 logarithm of minimal an- gle of resolution (logMAR) 값으로 변환하였고, 안전수지 는 20/2000의 시력으로 변환하였다.28
통계는 SPSS 프로그램(SPSS ver. 12.0 for Windows;
SPSS Inc., Chicago, IL, USA)을 이용하였다. Repeated Measures Analysis of Variances (ANOVA) 분석 방법을 이용하여 서로 다른 시점에 측정된 값을 비교하였다. 0.05 미만의 p값을 통계적으로 유의한 값으로 정의하였다.
결 과
대상안은 총 33명 33안이었는데, 남자가 5명, 여자는 28 명이었으며, 평균 연령은 73.7 ±5.4세(63-85세)였다. 진 단 시 평균 logMAR 시력은 0.76 ±0.49 (Snellen equiv-
BCVA (log MAR) 1.6
1.2
0.8
0.4
0
Baseline 3 months 6 months 12 months p = 0.590
p = 0.037 p < 0.001
Follow-up period
Central foveal thickness (m)µ 500 400 300 200 100
0 Baseline 3 months 6 months 12 months Follow-up period
p < 0.001 p < 0.001
p < 0.001
Figure 3. Twelve-month changes in logarithm of minimal an-
gle of resolution (log MAR) best-corrected visual acuity (A, BCVA) and central foveal thickness (B) in eyes with retinal angiomatous proliferation that were treated with anti-vascular growth factor mono-treatment, according to the follow-up period. Statistical analysis was performed using repeated measures analysis of variances.Table 2. Distribution of eyes according to the degree of visual
acuity change between at diagnosis and at 12-month following the first anti-vascular endothelial growth factor injection (N = 33)Degree of change No. of eyes (%)
≥0.2 log MAR of gain 13 (39.4)
Stable 16 (48.5)
≥0.2 log MAR of loss 4 (12.1)
alent, 20/115)였으며, 중심망막두께는 356.8 ± 70.9 μm (n=33)였다. 망막혈관종성증식의단계별 분포는 1단계, 2 단계 및 3단계가 각각 36.4% (12/33안), 42.4% (14/33 안) 및 21.2% (7/33안)로 나타났다(Table 1). 모든 환자 들은 진단 직후부터 1개월 간격으로 3회의 유리체강내 ranibizumab 주입술을 시행 받았고, 이후 12개월까지의 추 적관찰 기간 동안 평균 1.2 ± 1.2회(0-4회)의 유리체강 내 항혈관내피세포성장인자 주입술이 추가로 시행되어, 진
단 후 12개월 동안 평균 4.2 ±1.7회(3-7회)의 유리체강 내 항혈관내피세포성장인자 주입술을 시행 받았으며, 첫 주사 후 12개월까지의 평균 내원 횟수는 7.3 ±0.9회였다 (6-9회). 69.7% (23/33안)에서 추적관찰 기간 사이에 재 발이 관찰되었다(Fig. 2). 최초 재발 시기는 3회째 주사 후 부터 평균 4.7 ±1.9개월(2-9개월)이 경과한 시점이었는 데, 이전 외래 방문과 재발이 확인된 외래 방문 사이의 기 간은 평균 2.6 ±0.8개월(1-4개월)이었다. 추적관찰 기간 동안 망막박리 혹은 안내염과 같은 심각한 합병증은 발생 하지 않았다.
최초 주사치료 후 3개월, 6개월, 및 12개월에 측정된 평 균 시력은 각각 0.55 ±0.35 (Snellen equivalent, 20/70), 0.67 ±0.41 (20/93), 및 0.70 ± 0.50 (20/100)이었다 (Fig. 3A). 각 시기에 측정된 시력은 서로 유의한 차이가 있었는데(p<0.001), 최초 주사 후 3개월 및 6개월에 측정 된 시력의 경우 치료 전 측정된 시력에 비해 유의하게 호전 된 결과를 보였으나(p<0.001, p=0.037) 12개월에 측정된 시력은 치료 전 측정된 시력과 비교하여 유의한 차이가 없 었다(p=0.590). 12개월의 추적관찰 기간 동안 시력이 0.2 logMAR 이상 호전된 환자는 13명(39.4%)이었으며, 0.2 logMAR 이상 악화된 환자는 4명(12.1%)이었다. 나머지 16명(48.5%)의 경우 비교적 안정적인 시력을 유지하였다 (Table 2). 최초 주사치료 후 3개월, 6개월, 및 12개월에 측정된 평균 중심망막두께는 각각 196.2 ±60.3 μm (n=33), 242.4 ±102.1 μm (n=33), 및 210.9 ±81.2 μm (n=33) 였다(Fig. 3B). 각 시기에 측정된 중심망막두께는 서로 유 의한 차이가 있었는데(p<0.001), 치료 후 3개월, 6개월 및 12개월에 측정된 중심망막두께는 치료 전 측정된 값에 비 해 유의하게 줄어든 결과를 보였다(p<0.001, p<0.001, p<0.001). 12개월 추적관찰 시점의 빛간섭단층촬영에서 중심망막두께가 250 μm 이상이면서 망막하액, 망막내액이 뚜렷하게 관찰된 경우는 6안(18.2%)이었다. 이들 중 1안 은 2개월 전 재발 진단 후 항혈관내피세포성장인자 치료를 시행 받고 있던 경우였으며, 나머지 5안은 12개월 시점에 재발이 의심되는 경우였다.
12개월에 형광안저혈관조영술을 시행한 안은 13안(39.4%) 이었는데, 이들 중 질환의 재발이 의심되어 검사를 시행한 경우는 앞서 기술한 5안이었으며, 나머지 8안의 경우 의사 의 판단에 따라 질병의 활동성 여부를 확인하기 위해 조영 술을 시행하였다. 빛간섭단층촬영에서 망막하액, 망막내액 이 뚜렷하게 관찰된 5안 모두에서 형광 누출이 관찰되었으 며, 나머지 8안의 경우 형광 누출은 관찰되지 않았다(Fig.
4).
A
B
A B C
D E
F G
Figure 4. (A-D) Baseline fundus photography (A), fluorescein angiography (B), indocyanine green angiography (C), and op-
tical coherence tomography (D) findings of an eye with retinal angiomatous proliferation. (E-G) Twelve months after an- ti-vascular endothelial growth factor treatment, resolution of retinal hemorrhage (E) cessation of leakage (F) and resolution of intraretinal and subretinal fluid (G) was noted. The visual acuity was improved from 20/400 to 20/100.고 찰
본 연구에서는 망막혈관종성증식 진단 후 1개월 간격으 로 3회의 유리체강내 항혈관내피세포성장인자 주입술을 시 행하고, 이후 경과관찰을 시행하면서 질병의 활동성이 재발 하는 경우 재주사하는 방법을 통해 최초 6개월 동안은 중심 망막두께의 유의한 감소와 함께 시력의 유의한 호전을 얻 을 수 있었다. 치료 후 12개월 동안 중심망막두께는 유의하 게 감소된 상태로 유지되었으며, 약 88%의 환자에서 추적 관찰 기간 동안 시력이 호전되거나 안정적으로 유지되는
결과를 보였다.
유리체강내 항혈관내피세포성장인자 주입술 단일요법을 이용해 망막혈관종성증식을 치료한 기존 연구들의 경우 치 료 직전 측정한 시력과 비교하여 9-12개월 후 측정한 시력 이 유의하게 호전되는 결과를 보였다.5,15-17그러나 본 연구 에서는 이들 해외 연구에 비해 12개월의 시력 호전 정도가 상대적으로 뚜렷하지 않은 결과를 보였다. 특히 본 연구의 초기 시력(20/107)과 비슷한 수준의 초기 시력(20/104)을 보인 Konstantinidis et al15의 연구의 경우 본 연구와는 달 리 초기 치료를 시행한 후 매달 추적관찰을 시행하였는데,
이러한 추적관찰 방식의 차이에 의해 상기 연구에서 우리 연구에 비해 병변의 재발을 보다 빨리 진단할 수 있었을 것 으로 생각되며, 이는 시력 두 연구 사이의 예후 차이의 가 장 큰 원인으로 판단된다. 망막혈관종성증식으로 진단된 국 내 환자를 대상으로 광역학치료와 유리체강내 항혈관내피 세포성장인자 주입술 병합요법을 시행한 Lee et al19의 연 구의 경우 평균 시력은 치료 전 20/125에서 12개월 후 20/63으로 유의하게 호전되었다. 우리 연구의 경우 치료 전 평균 시력은 20/107으로 기존 연구에 비해 오히려 조금 더 나은 값을 보였으나 12개월 시력의 경우 20/84로 유의한 시력 호전이 나타나지 않았다.
삼출성 황반변성에서 치료의 지연은 시력 예후를 악화시 킬 수 있는 것으로 알려졌다.29-31 특히 최근 연구 결과에 의하면 증상 발생부터 1개월 이내에 치료받은 경우 그 이후 에 치료받은 경우에 비해 더 나은 시력 예후를 보이는 것으 로 나타났다.31본 연구에서 재발한 환자들의 경우 이전 외 래 방문과 재발이 확인된 외래 방문 사이에는 평균 약 2.6 개월의 기간이 있었는데, 비록 재발 시기를 정확하게 알 수 는 없었으나 상당수 안의 경우 최소한 수주 이상 치료가 지 연되었을 가능성이 있으며, 누적된 망막 손상이 최종 시력 예후의 악화에 일부 기여하였을 것으로 생각된다. 보다 나 은 임상 결과를 기대하기 위해서는 초기에 1개월 간격으로 4-5회 이상의 주입술을 시행하거나 2개월 미만의 짧은 기 간으로 보다 면밀하게 추적관찰을 시행하는 방법이 도움이 될 수 있을 것으로 생각된다.
후향적 의무기록 분석이라는 점 이외에도 본 연구의 결 론은 단일 병원의 임상 경험을 반영한다는 제한점이 있다.
조금 다른 간격의 추적관찰을 시행하는 병원의 경우 본 연 구의 결론을 그대로 적용하기 어려운 부분이 있을 것이다.
또한 일부 환자에서 증상 발생 기간이 정확히 평가되지 못 했을 가능성이 있으며, 따라서 삼출성 연령관련환반변성이 진행되어 망막-맥락막 문합이 발생한 경우가 일부 포함되 었을 가능성을 완전히 배제할 수 없을 것이다.
결론적으로, 1개월 간격으로 3회의 유리체강내 항혈관내 피세포성장인자 주입술을 초기 치료로 시행하고, 이후 경과 관찰을 시행하면서 질병의 활동성이 재발하는 경우 주사 치료를 추가로 시행하는 방법을 통해 대부분의 환자에서 황반 두께의 정상화와 함께 시력의 호전 혹은 유지를 기대 할 수 있었다.
REFERENCES
1) Yannuzzi LA, Negrão S, Iida T, et al. Retinal angiomatous pro- liferation in age-related macular degeneration. Retina 2001;21:
416-34.
2) Massacesi AL, Sacchi L, Bergamini F, Bottoni F. The prevalence of retinal angiomatous proliferation in age-related macular degener- ation with occult choroidal neovascularization. Graefes Arch Clin Exp Ophthalmol 2008;246:89-92.
3) Maruko I, Iida T, Saito M, et al. Clinical characteristics of exuda- tive age-related macular degeneration in Japanese patients. Am J Ophthalmol 2007;144:15-22.e2.
4) Liu Y, Wen F, Huang S, et al. Subtype lesions of neovascular age-related macular degeneration in Chinese patients. Graefe's Arch Clin Exp Ophthalmol 2007;245:1441-5.
5) Gross NE, Aizman A, Brucker A, et al. Nature and risk of neo- vascularization in the fellow eye of patients with unilateral retinal angiomatous proliferation. Retina 2005;25:713-8.
6) Bottoni F, Massacesi A, Cigada M, et al. Treatment of retinal an- giomatous proliferation in age-related macular degeneration: a ser- ies of 104 cases of retinal angiomatous proliferation. Arch Ophthalmol 2005;123:1644-50.
7) Rosenfeld PJ, Brown DM, Heier JS, et al. Ranibizumab for neo- vascular age-related macular degeneration. N Engl J Med 2006;
355:1419-31.
8) Brown DM, Kaiser PK, Michels M, et al. Ranibizumab versus ver- teporfin for neovascular age-related macular degeneration. N Engl J Med 2006;355:1432-44.
9) Spaide RF, Laud K, Fine HF, et al. Intravitreal bevacizumab treat- ment of choroidal neovascularization secondary to age-related macular degeneration. Retina 2006;26:383-90.
10) Cohen SY, Dubois L, Tadayoni R, et al. Results of one-year's treat- ment with ranibizumab for exudative age-related macular degener- ation in a clinical setting. Am J Ophthalmol 2009;148:409-13.e1.
11) Kang S, Cho WK, Roh YJ. The efficacy of ranibizumab for choroi- dal neovascularization in age-related macular degeneration. J Korean Ophthalmol Soc 2009;50:725-30.
12) Kim YH, Kim ES, Yu SY, Kwak HW. Long-term effect of intra- vitreal bevacizumab for CNV secondary to age-related macular degeneration. J Korean Ophthalmol Soc 2008;49:1935-40.
13) Parodi MB, Iacono P, Menchini F, et al. Intravitreal bevacizumab versus ranibizumab for the treatment of retinal angiomatous proliferation. Acta Ophthalmol 2013;91:267-73.
14) Ghazi NG, Knape RM, Kirk TQ, et al. Intravitreal bevacizumab (Avastin) treatment of retinal angiomatous proliferation. Retina 2008;28:689-95.
15) Konstantinidis L, Mameletzi E, Mantel I, et al. Intravitreal ranibi- zumab (Lucentis®) in the treatment of retinal angiomatous pro- liferation (RAP). Graefes Arch Clin Exp Ophthalmol 2009;247:
1165-71.
16) Costagliola C, Romano MR, dell'Omo R, et al. Intravitreal bev- acizumab for the treatment of retinal angiomatous proliferation.
Am J Ophthalmol 2007;144:449-51.
17) Hufendiek K, Hufendiek K, Panagakis G, et al. Visual and morpho- logical outcomes of bevacizumab (Avastin®) versus ranibizumab (Lucentis®) treatment for retinal angiomatous proliferation. Int Ophthalmol 2012;32:259-68.
18) Kang JH, Park KA, Chung SE, Kang SW. Retinal angiomatous proliferation and intravitreal bevacizumab injection. Korean J Ophthalmol 2007;21:213-5.
19) Lee MY, Kim KS, Lee WK. Combination therapy of ranibizumab and photodynamic therapy for retinal angiomatous proliferation with serous pigment epithelial detachment in Korean patients:
twelve-month results. Retina 2011;31:65-73.
20) Lee PY, Lee WK. Treatments of stage 1 retinal angiomatous proliferation. J Korean Ophthalmol Soc 2008;49:442-9.
21) Byeon SH, Hong JP, Lee H, et al. Photodynamic therapy results of retinal angiomatous proliferation with pigmented epithelial detach- ment in age-related macular degeneration. J Korean Ophthalmol Soc 2006;47:1410-6.
22) Cho YJ, Park SP. Intravitreal ranibizumab therapy for neovascular age-related macular degeneration with a predominantly hemor- rhagic lesion. J Korean Ophthalmol Soc 2011;52:838-45.
23) Chang MA, Do DV, Bressler SB, et al. Prospective one-year study of ranibizumab for predominantly hemorrhagic choroidal neo- vascular lesions in age-related macular degeneration. Retina 2010;
30:1171-6.
24) Shienbaum G, Garcia Filho CA, Flynn HW Jr, et al. Management of submacular hemorrhage secondary to neovascular age-related macular degeneration with anti–vascular endothelial growth factor monotherapy. Am J Ophthalmol 2013;155:1009-13.
25) Avery RL, Fekrat S, Hawkins BS, Bressler NM. Natural history of
subfoveal subretinal hemorrhage in agerelated macular degeneration.
Retina 1996;16:183-9.
26) Bennett SR, Folk JC, Blodi CF, Klugman M. Factors prognostic of visual outcome in patients with subretinal hemorrhage. Am J Ophthalmol 1990;109:33-7.
27) Riusala AM, Immonen IJ. Predictors of structural findings in old disciform lesions. Am J Ophthalmol 2004;138:245-53.
28) Holladay JT. Visual acuity measurements. J Cataract Refract Surg 2004;30:287-90.
29) Arias L, Armada F, Donate J, et al. Delay in treating age-related macular degeneration in Spain is associated with progressive vi- sion loss. Eye (Lond) 2009;23:326-33.
30) Oliver-Fernandez A, Bakal J, Segal S, et al. Progression of visual loss and time between initial assessment and treatment of wet age-related macular degeneration. Can J Ophthalmol 2005;40:313-9.
31) Rauch R, Weingessel B, Maca SM, Vecsei-Marlovits PV. Time to first treatment: the significance of early treatment of exudative age-related macular degeneration. Retina 2012;32:1260-4.
=ABSTRACT=
Twelve-Month Outcomes of Intravitreal Anti-Vascular Endothelial Growth Factor Therapy for Retinal Angiomatous Proliferation
Deok Bae Kim, MD1, Jae Hui Kim, MD2, Seong Hun Jeong, MD2, Tae Gon Lee, MD2, Jong Woo Kim, MD2, Chul Gu Kim, MD2, Sung Won Cho, MD2, Dong Won Lee, MD2, Jung Il Han, MD2
Happyeye21 Hospital1, Gwangju, Korea
Department of Ophthalmology, Kim’s Eye Hospital, Konyang University College of Medicine2, Seoul, Korea
Purpose: To evaluate the 12-month outcomes of anti-vascular endothelial growth factor (VEGF) treatment for patients with retinal angiomatous proliferation (RAP).
Methods: Retrospective review of medical records was performed for 33 patients (33 eyes) who were diagnosed with RAP.
All patients were initially treated with three consecutive intravitreal anti-VEGF injections after diagnosis. Additional treat- ment was performed when the recurrence of exudation was noted. The best-corrected visual acuity (BCVA) was measured before the first injection and at 3, 6, and 12 months after the first injection. The value measured before the treatment was compared with those measured after treatment.
Results: The patients received an average of 4.2 ± 1.7 intravitreal anti-VEGF injections during the 12-month follow-up period. The logarithm of minimal angle of resolution (log MAR) values of BCVA before the first injection and at 3, 6, and 12 months after the first injections were 0.76 ± 0.49, 0.55 ± 0.35, 0.67 ± 0.41, and 0.70 ± 0.50, respectively. BCVA was sig- nificantly improved at 3 and 6 months (p < 0.001 and p = 0.037) compared to that measured before the first injection.
However, there was no significant difference between BCVA before the first injection and 12 months after the first injection (p = 0.590). At 12 months of follow-up, 29 eyes (87.9%) showed stable (<2 log MAR lines of change) or improved (≥2 log MAR lines of improvement) BCVA.
Conclusions: Anti-VEGF therapy was found to be beneficial in both normalizing macular thickness and in improving or maintaining visual acuity in the majority of patients with RAP.
J Korean Ophthalmol Soc 2013;54(11):1700-1707
Key Words: Anti-vascular endothelial growth factor, Clinical outcomes, Retinal angiomatous proliferation, Visual acuity
Address reprint requests to Jae Hui Kim, MD Kim’s Eye Hospital
#136 Yeongsin-ro, Yeongdeungpo-gu, Seoul 150-034, Korea
Tel: 82-2-2671-7665, Fax: 82-2-2671-6359, E-mail: [email protected]