http://dx.doi.org/10.16956/kaes.2016.16.3.57
Endocrine Surgery
소포변이 갑상선유두암 진단에서 초음파검사와 수술 중 동결절편 검사의 역할
충북대학교병원 외과1, 병리학과2, 충북대학교 의과대학 병리학교실3, 외과학교실4
공병호
1ㆍ김동주
1ㆍ이옥준
2,3ㆍ박진우
1,4Supplementary Role of Ultrasonography and
Intraoperative Frozen Section Analysis in Diagnosis of Follicular Variant of Papillary Thyroid Carcinomas
Purpose: The follicular variant of papillary thyroid carcinoma (FVPTC) is the most common variant of papillary thyroid carcinoma (PTC). Preoperative diagnosis of FVPTC is often confused with cPTC, follicular neoplasm (FN), and benign follicular lesion because of the paucity of nuclear changes of PTC and overlapping features with benign and other neoplastic follicular lesions. The aim of this study is to elucidate whether ultrasonography and/or intraoperative frozen section analysis (FSA) have a supplementary role in the diagnosis of FVPTC.
Methods: Fifty-five patients diagnosed with histologically confirmed FVPTC from January 2007 to December 2013 were identified. All patients had undergone either lobectomy with/without completion thyroidectomy or total thyroidectomy. Medical records, final histological reports and sonographic (US) findings were reviewed. All sonographic images, 53 fine needle aspiration cytology (FNAC) slides, and FSA slides for 24 cases were available for reexamination.
Results: Three histologic types of FVPTC were identified: encapsulated (n=39); infiltrative (n=15); and diffuse (n=1). There were two distinct sonographic patterns: FN-type (n=28) and PTC-type (n=27). The encapsulated type is more common in the FN-like pattern, compared to the PTC-like one (85.7% vs. 55.6%, P=0.009). Among the 24 cases in which sonographic images and FNAC and FSA slides were available for review, six cases (25%) were diagnosed as either FN in FNAC and suspicious PTC(R/O PTC)/PTC in FSA or R/O PTC/PTC in FNAC and FN in FSA. Among those 24 cases described above, 13 cases (54.2%) were diagnosed as either FN-type in US and R/O PTC/PTC in FNAC/FSA or PTC-type in US and FN in FNAC/FSA.
Conclusion: It is difficult to make a correct diagnosis of FVPTC before definitive treatment even with US, FNAC and FSA. However the possibility of FVPTC must be considered, especially when diagnoses in US, FNAC and FSA are different and include R/O PTC/PTC and FN in the same case.
Key Words: Papillary thyroid carcinoma, Follicular variant, Follicular neoplasm, Fine needle aspiration cytology, Ultrasonography, Frozen section analysis 중심 단어: 갑상선유두암, 소포변이, 소포종양, 세침흡인세포검사, 초음파검사, 동결절편검사
Byeong-Ho Ghong1,
Dong-Ju Kim1, Ok-Jun Lee2,3, Jin-Woo Park1,4
Departments of 1Surgery, 2Pathology, Chungbuk National University Hospital, Departments of 3Pathology,
4Surgery, Chungbuk National University, College of Medicine, Cheongju, Korea
This work was supported by the intramural research grant of Chungbuk National University in 2015.
Received June 1, 2016, Revised July 20, 2016, Accepted August 2, 2016 Correspondence: Jin-Woo Park
Department of Surgery, Chungbuk National Univsersity Hospital, 776, 1 sunhwan-ro, Seowon-gu, Cheongju 28644, Korea Tel: +82-43-269-6033
Fax: +82-43-266-6037
E-mail: [email protected]
Copyright © 2016 Korean Association of Thyroid and Endocrine Surgeons; KATES. All Rights Reserved.
cc This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
이 있다.(2,3) 소포변이 갑상선유두암은 전형적인 갑상선유두암 에서 보이는 핵의 변화를 가지면서 갑상선소포암에서 볼 수 있는 미세소포 구조(microfollicular structure)를 동시에 가질 때 진단 할 수 있다. 그러나, 핵의 변화가 종양의 일부에서만 관찰될 수 있 어 소포종양, 갑상선종 등의 다른 진단과 감별이 어려울 수 있다.
최근 개정된 미국갑상선학회의 권고안에서는 크기가 4 cm 미만인 소포기원 분화 갑상선암에서 다른 위험 요인이 없는 경우 엽절제를 적용할 수 있다고 권고하고 있다.(4) 그 동안 소포변이 갑상선유두암에서 갑상선 절제의 범위는 기본적으로 전형적인 갑상선유두암과 동일하게 적용되어 왔으나, 최근의 보고에 의하 면 소포변이 갑상선유두암의 1/2∼2/3에서 예후가 매우 우수하 고 림프절 전이가 비교적 드문 피막형인 경우가 차지하고 있어, 엽절제술의 적응이 될 수 있는 경우가 많고, 림프절 절제의 경우 에는 전형적인 갑상선유두암과 달리 예방적 중앙경부림프절절제 의 효과가 불명확하다.(4) 심지어 최근에는 비침습형 소포변이 유 두암을 암종으로 분류하지 않고 소포종양에서와 마찬가지로 암 의 잠재력을 갖는 종양의 상태로 규정하자는 움직임도 있다.(5)
이렇게 소포변이 갑상선유두암에서 전형적인 갑상선유두암 에 비해 다른 치료를 권고하고 있어 수술 전 진단이 중요함에도 불구하고 대부분의 경우에 수술 후 조직검사에서 진단되는 경우 가 많다. 이는 소포종양에서와 같이 수술 전 세침흡인세포검사 를 통해 소포종양이나 갑상선종 등과 감별하는데 어려움이 있으 며, 특징적인 핵의 변화로 전형적인 갑상선유두암으로 오인되기 도 하기 때문이다.
이에 저자들은 후향적 조사를 통하여 초음파 검사와 세침흡인 세포검사, 그리고 수술 중 시행한 동결절편검사가 소포변이 갑상 선유두암의 진단 가능성을 높일 수 있는지를 알아보고자 하였다.
방 법
2007년 1월부터 2013년 12월까지 충북대학교병원에서 갑 상선암으로 일차 수술을 받은 환자는 모두 1,322명이었고, 소포 변이 갑상선유두암으로 최종 진단된 경우는 55명(4.2%)이었다.
이들 소포변이 갑상선유두암 환자를 대상으로 의무기록과 영상 검사 결과, 병리 조직학적 소견을 후향적으로 분석하였다. 대상 환자 중 53명에서 수술 전 세침흡인세포검사 슬라이드를, 24명
하였는데, 3 범주로 분류할 때는 ‘양성과 의미를 정하기 어려운 비정형성(AUS) 또는 소포병변(FLUS)’을 하나의 범주로 하고,
‘소포종양’과, ‘유두암의심 또는 유두암’을 각각 하나의 범주로 하였다. 동결절편검사의 결과도 유사하게 ‘양성’, ‘소포종양 의 심’, ‘갑상선유두암 의심 또는 갑상선암’의 3 범주로 나누었다.
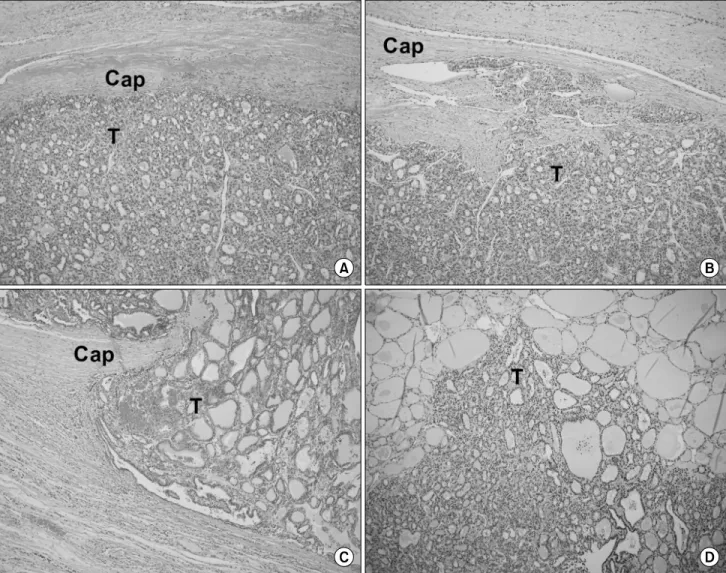
최종 조직진단은 피막형(encapsulated), 침윤형(infiltrative), 미만형(diffuse)으로 구분하였다. 피막형은 종양의 피막이 완전 하거나 불완전하더라도 주위와 경계가 분명하면서 피막외 침범 이 없는 경우로 하였다. 침윤형의 경우에는 최소침윤 소포암과 같이 피막 또는 혈관 침윤이 있는 경우를 최소(minimal) 침윤형 으로 하였고, 종양의 경계를 확인할 수 있으나 최소 침윤의 범위 를 넘어서는 침윤이 있는 경우를 광범위(wide) 침윤형으로 하였 다. 미만형의 경우는 피막 형성이 없고 종양의 경계가 불명확하 게 주위 조직으로 침윤하는 경우로 하였다(Fig. 1).
초음파 검사의 결과는 2명의 외과의에 의해 이루어졌으며, 소 포종양에서와 같은 둥글고 경계가 좋고 내부 에코가 비교적 균질 한 경우를 소포종양형, 갑상선유두암에서와 같이 경계가 불규칙 적이거나 분엽의 형태를 보이고, 현저한 저에코, 키가 큰 결절, 미세석회화를 동반하는 경우를 유두암형으로 나누었다(Fig. 2).
통계적 검증은 SPSS 12.0KO for windows를 사용하여 Pearson 카이제곱 검정을 통해 확인하였고, P<0.05 인 경우 유 의한 차이라고 판단하였다.
결 과
1. 소포변이 갑상선유두암의 초음파 소견 및 조직학적 특성 소포변이 갑상선유두암은 병리학적으로 피막형(encap- sulated), 침윤형(infiltrative), 미만형(diffuse)으로 구분하였는 데 각각 39예(70.9%), 15예(27.3%), 1예(1.8%)로 피막형이 가 장 흔한 유형이었다.
초음파 소견을 크게 소포종양형과 유두암형으로 나누었을 때 각각 28예(50.9%), 27예(49.1%)를 차지하였다. 소포종양형일 때 피막형의 빈도가 더 높았다(85.7% vs. 55.6%, P=0.009) (Table 1). 반대로 유두암형의 경우에는 침윤형의 비중이 높았다.
Fig. 1. Histologic types of follicular variant of papillary thyroid carcinomas. (A) Encapsulated, (B) minimally infiltrative, (C) widely infiltrative, and (D) diffuse type. Cap = capsule; T = tumor (H&E, ×100).
Fig. 2. Sonographic patterns of follicular variant of papillary thyroid carcinomas. (A) A papillary thyroid carcinoma-like ultrasound (US) image shows an irregular hypoechoic nodule with microcalcifications in the left thyroid gland. (B) A follicular neoplasm-like US image shows a well-defined oval isoechoic nodule in the right thyroid gland.
FNAC
Frozen
Benign FN >R/O PTC Total
Benign/AUS, FLUS 2 (8.3%) 2 (8.3%) 2 (8.3%) 6 (25.0%)
FN 3 (12.5%) 1 (4.2%) 2 (8.3%) 6 (25.0%)
>R/O PTC 3 (12.5%) 4 (16.7%) 5 (20.8%) 12 (50.0%)
Total 8 (33.3%) 7 (29.2%) 9 (37.5%) 24 (100%)
FNAC = fine needle aspiration cytology; AUS = atypia of undetermined significance; FLUS = follicular lesion of undetermined significance; FN = follicular neoplasm; >R/O PTC = definitive or suspicious papillary thyroid carcinoma.
Table 2. Comparison between results of fine needle aspiration cytology and frozen section analysis in follicular variant of papillary thyroid carcinomas
Histologic types| Sonographic pattern USFN-type USPTC-type Total Encapsulated 24 (43.6%)* 15 (27.3%) 39 (70.9%)
Full 7 5 12
Partial 17 10 27
Infiltrative 4 (7.3%) 11 (20.0%) 15 (27.3%)
Minimal 2 6 8
Wide 2 5 7
Diffuse 1 (1.8%) 1 (1.8%)
Total 28 (50.9%) 27 (49.1%) 55 (100%) USFN-type = follicular neoplasm-like sonographic pattern;
USPTC-type = papillary thyroid carcinoma-like sonographic pattern.
*Encapsulated type is more common in USFN-type, compared to USPTC-Type (85.7% vs. 55.6%, P=0.009).
Table 1. Histologic types and sonographic patterns in folli- cular variant of papillary thyroid carcinomas
NF<50% NF≥50%
FNAC Non-PTC 8 57.1% 14 36.9%
>R/O PTC 7 42.9% 24 63.1%
Total 15 100.0% 38 100.0%
P=0.357.
Non-PTC = cytologic diagnoses but papillary thyroid carcinoma;
>R/O PTC = definitive or suspicious papillary thyroid carcinoma.
Table 3. Cytologic diagnosis by FNAC according to propor- tion of cells with nuclear features of classic papillary thyroid carcinoma (NF) in follicular variant of papillary thyroid carcinomas
다. 유두암 진단을 기대할 수 있는 경우는 31예로 전체의 58.5%
로 가장 많았다.
세포검사와 동결절편검사의 결과가 모두 확인 가능한 경우는 24예였다(Table 2). 이들 중 수술 전 세포검사에서 갑상선유두 암을 의심하는 소견을 보인 경우가 전체의 50%로 가장 많았다.
수술 중 동결절편 검사의 경우에도 갑상선유두암을 의심하는 소 견을 보인 경우가 37.5%로 가장 많았으나, 양성 또는 소포종양 을 의심하는 경우와 큰 차이를 보이지는 않았다. 두 가지 검사에 서 모두 갑상선 유두암을 의심한 경우는 5예(20.8%) 였고, 한 쪽 검 사에서는 갑상선유두암이 의심되고 다른 한쪽 검사에서는 소포종 양을 의심하였던 경우는 모두 6예(25.0%) 였다. 11예(45.8%)에서 동결절편검사를 활용하여 수술 중에 전형적인 갑상선유두암 또
암의 핵 변화를 보이는 세포 분율이 50% 이상인 경우에서 세포검 사 결과 갑상선유두암을 의심할 수 있는 경우가 더 빈번하였으나 통계적 유의성은 없었다: 63.1% vs. 42.9%, P=0.357 (Table 3).
3. 소포변이 갑상선유두암의 진단에서 초음파패턴, 세포진단, 동결절편검사의 조합
수술 전 시행한 초음파 검사 결과와 세포검사 결과, 그리고 수 술 중 시행한 동결절편 검사 결과가 모두 확인 가능한 24예를 대 상으로 이들 검사의 조합이 수술 중 소포변이 갑상선유두암의 진 단에 도움을 주는 지를 알아보았다. 먼저 초음파 소견을 바탕으 로 소포종양형(USFN-type)과 유두암형(USPTC-type)으로 나 누고, 각 군에서 세포검사와 동결절편검사의 결과를 비교하였다 (Table 4). 두 가지 검사에서 모두 갑상선 유두암을 의심한 경우 는 소포종양형에서 1예(8.3%) 였는데 병리학적 유형은 피막형 이었고, 유두암형에서는 4예(33.3%)가 있었는데, 피막형 1예와 침윤형 2예, 그리고 미만형 1예였다. 수술 전 세포검사와 수술 중
USFN-type (n=12) USPTC-type (n=12) Frozen section analysis
Benign FN >R/O PTC Benign FN >R/O PTC
FNAC Benign/AUS/FLUS 2 (16.7%) 1 (8.3%) 1 (8.3%) 2 (16.7%)
FN 1 (8.3%) 1 (8.3%) 2 (16.7%) 2 (16.7%)
>R/O PTC 3 (25.0%) 3 (25.0%) 1 (8.3%) 1 (8.3%) 4 (33.3%)
FNAC = fine needle aspiration cytology; AUS = atypia of undetermined significance; FLUS = follicular lesion of undetermined significance; FN = follicular neoplasm; >R/O PTC = definitive or suspicious papillary thyroid carcinoma; USFN-type = follicular neoplasm-like sonographic pattern; USPTC-type = papillary thyroid carcinoma-like sonographic pattern.
Table 4. Comparison between results of fine needle aspiration cytology and frozen section analysis according to sonographic patterns in follicular variant of papillary thyroid carcinomas
동결절편 검사에서 각각 갑상선유두암 의심과 소포종양 의심으 로 서로 다르게 진단된 경우는 소포종양형-과 유두암형-초음파 소견에서 각각 3예(25.0%)로 일부에서만 관찰되었다. 반면 초 음파 검사 소견을 중심으로, 소포종양의 초음파 소견을 보이면 서 세침흡인세포검사나 동결절편검사에서 갑상선유두암이 의 심되는 경우는 12예 중 7예(58.3%), 갑상선유두암의 초음파 소 견을 보이면서 세침흡인세포검사나 동결절편검사에서 소포종 양이 의심되는 경우는 12예 중 6예(50.0%)로 전체 24예 중 13예 (54.2%)에서 초음파 검사의 결과와 세침흡인세포검사 또는 동 결절편검사의 결과가 서로 다르고 각각 갑상선유두암과 소포종 양의 특성을 모두 보여주었다.
고 찰
갑상선유두암은 가장 흔한 내분비암의 하나로 전형적인 경우 외에도 여러 가지 변이가 보고되고 있는데, 소포변이가 9∼
22.5%를 차지해 가장 흔하다.(1) 소포변이 갑상선유두암은 전 형적인 갑상선유두암에 비해 림프절 전이와 갑상선 피막외 침범 의 빈도가 낮다는 특징이 있으며,(2) 장기 생존율은 서로 비슷한 것으로 보고된다.(3) 소포변이 갑상선유두암의 수술적 치료는 전형적인 갑상선유두암이나, 소포암의 경우와 다를 수 있으므로 수술 전 진단이 중요함에도 불구하고 대부분의 경우에 수술 후 조직검사에서 진단되는 경우가 많다. 소포변이 갑상선유두암은 갑상선유두암의 핵형을 갖는 종양 세포가 관찰되지만, 잘 형성 된 유두 모양 구조가 보이지 않고 미세소포구조를 보일 때 진단 할 수 있다. 그러나 수술 전 진단은 쉽지 않은데, 특징적인 핵형의 변화가 균일하게 분포하지 않을 수 있고, 다른 양성 병변이나 소 포종양과의 감별이 어렵기 때문이다. Manimaran 등(6)은 세침 흡인세포검사 검체에서 미세소포 구조를 보이면서 동시에 핵형 의 변화가 있을 경우에 좀 더 세심하게 유두암의 전형적인 핵형 의 변화인 고랑(nuclear groove) 또는 가성함입체(nuclear pseudoinclusion) 등을 살펴보는 것이 중요하다고 보고하였으
나, Ustun 등(7)은 실제로 소포변이 갑상선유두암의 수술 전 세 포 진단이 매우 어려워서, 암으로 진단하는 경우가 전체의 27%
에 불과하며, 암을 의심하는 경우까지 포함하여도 38% 정도였 고, BRAF 돌연변이 양성인 경우가 전체의 18%에 불과하여 진단 에 추가의 도움을 주지 못한다고 보고하였다.
본 연구에서는 이런 한계를 극복하기 위해, 수술 전 시행한 초 음파 검사 소견과 세침흡인세포검사 결과에 추가로 조직 진단의 일환으로 시행한 수술 중 동결절편검사를 합하여 수술 중 소포변 이 갑상선유두암의 진단 가능성을 높일 수 있는지를 알아보았다.
소포변이 갑상선유두암의 진단은 갑상선유두암의 특성과 소 포종양의 특성을 한 종양에서 동시에 확인할 때 가능하다. 전자 는 세침흡인세포검사 또는 동결절편 검사에서 핵의 변화를 통해 알아볼 수 있고, 특징적인 초음파 검사 소견을 통해서도 강력하 게 의심할 수 있다. 반면 후자의 경우에는 세침흡인세포검사 또 는 동결절편검사에서 미세소포구조를 가지고 양성 종양과 유사 한 초음파소견을 보일 때 의심할 수 있지만 감별해야 할 진단이 많다. 본 연구에서 세침흡인세포검사, 동결절편검사, 초음파 검 사의 결과를 모두 재검토할 수 있었던 경우는 전체 55예 중 24예 (43.6%)였다. 갑상선유두암의 특징적인 핵의 변화와 소포종양 의 특성인 미세소포구조를 확인하는 방법으로 세침흡인세포검 사 결과와 동결절편검사 결과를 이용하였을 때, 24예 중 6예 (25.0%)에서 두 가지 특성을 모두 보여주었다. 반면 초음파 검사 소견을 중심으로, 소포종양의 초음파 소견을 보이면서 세침흡인 세포검사나 동결절편검사에서 갑상선유두암이 의심되는 경우 와 갑상선유두암의 초음파 소견을 보이면서 세침흡인세포검사 나 동결절편검사에서 소포종양이 의심되는 경우를 살펴보면, 전 자의 경우 12예 중 7예(58.3%), 후자의 경우 12예 중 6예 (50.0%)에서 두 가지 특성을 모두 보여주었다. 본 연구의 대상 환 자 수가 매우 적고 소포변이 갑상선유두암의 수술 전 진단적 검 사 결과가 다양하게 나타났지만, 절반이상의 환자(24예 중 13 예, 54.2%)에서 초음파 검사의 결과와 세침흡인세포검사 또는 동결절편검사의 결과가 서로 다르고 각각 갑상선유두암과 소포
우선 소포변이 갑상선유두암이 조직학적으로도 이질적인 아형 의 조합이란 점이다. Liu 등은 조직 진단 된 78예의 소포변이 갑상 선유두암을 피막형(encapsulated, n=61), 비피막형(infiltrative/
diffuse, n=17)으로 나누어 살펴보았는데 전자는 소포종양과 유 사하고, 후자는 전형적인 갑상선유두암과 유사한 임상병리학적 소견을 보이는 것으로 보고하였다.(8,9) 반면 Gupta 등은 조직 진단된 45예를 피막형 (encapsulated, n=22), 비피막형(non- encapsulated, n=19), 미만형(diffuse, n=4)으로 나누었다. 본 연구에서는 피막형(encapsulated, n=39), 침윤형(infiltrative, n=15), 미만형(diffuse, n=1)으로 나누었는데, 다른 보고에서와 마찬가지로 피막형이 가장 흔했다. 조직학적 아형에 따라 다른 임상병리학적 특성을 보이는 것으로 보고되는데 피막형의 경우 가 가장 온건한 임상 경과를 보이며, 침윤형이나 미만형의 경우 전형적인 갑상선유두암과 유사한 공격적인 임상병리학적 특성 을 보여주며, BRAF 돌연변이의 빈도도 높다고 한다.(1,10) 한편 소포변이 갑상선유두암의 초음파 소견은 전형적인 유두암의 패 턴을 보이는 경우와 소포종양의 패턴을 보이는 경우로 대별할 수 있다.(11) 전자의 경우 너비보다 높이가 긴 모양(a taller-than- wide shape), 침윤성 경계, 심한 저에코, 미세석회화 등의 소견 을 보이고, 후자의 경우에는 계란형의 고형종괴로 유두암의 특 징적인 소견을 찾아 볼 수 없다. 본 연구의 경우 소포종양형- 과 유두암형-초음파 소견은 각각 각각 28예(50.9%), 27예(49.1%) 였고, 소포종양형-초음파 소견일 때 피막형의 빈도가 더 높았다 (85.7% vs. 55.6%, P=0.009). 한편 종괴 내에 유두암의 핵형을 가지는 세포가 어떻게 분포하는가도 소포변이 갑상선유두암의 진단에 영향을 미칠 수 있다. 본 연구에서 유두암의 핵형을 가지 는 세포 분율의 차이를 살펴보았는데, 그 분율이 50%를 넘는 경 우가 55예 중 39예(70.9%)로 대부분을 차지하였지만, 다양한 분 포를 보여 주었다. 통계적 유의성은 없었지만 이런 세포 분율이 50% 이상인 경우에서 세포검사 결과 갑상선유두암을 의심할 수 있는 경우가 더 빈번하여, 진단에 영향을 주었을 것으로 추정할 수 있었다.
본 연구가 대상 환자가 적고 후향적 연구라는 점과 특히 수술 전 또는 수술 중에 진단에 활용할 수 있는 초음파 검사, 세침흡인 세포검사, 동결절편검사의 결과를 모두 확인하고 재검토가 가능 했던 경우가 전체 55예 중 24예(43.6%)에 그쳤다는 점이 결과의
진단 가능성을 높일 수도 있겠다고 조심스럽게 말할 수 있겠다.
또한 소포변이 갑상선유두암의 세포수준과 조직 수준의 이질성 을 고려한다면 대부분의 환자에서 수술 전 또는 수술 중에 정확 한 진단을 하기는 어려울 것으로 생각하며, 진단적 갑상선절제 술과 그 이후의 완결갑상선 절제술의 필요성은 계속해서 존재할 것으로 생각한다.
결 론
본 연구에서 수술 전에 갑상선유두암의 소포변이를 진단하는 것은 매우 어려웠고, 수술 전 초음파검사와 수술 중 동결절편검 사를 모두 참조하더라도 많은 개선을 기대하기는 어려웠다. 이 는 소포변이 갑상선유두암이 세포와 조직 수준에서 매우 이질적 인 특성을 보여주기 때문으로 생각한다. 그러나 이상의 세가지 검사 중에 갑상선유두암과 소포종양을 의심할 수 있는 소견이 서 로 다른 검사에서 동시에 존재하는 경우에는 소포변이 갑상선유 두암의 가능성을 반드시 고려하는 것이 좋겠다.
REFERENCES
1. Gupta S, Ajise O, Dultz L, Wang B, Nonaka D, Ogilvie J, et al.
Follicular variant of papillary thyroid cancer: encapsulated, nonencapsulated, and diffuse: distinct biologic and clinical entities. Arch Otolaryngol Head Neck Surg 2012;138:227-33.
2. Yu XM, Schneider DF, Leverson G, Chen H, Sippel RS. Follicular variant of papillary thyroid carcinoma is a unique clinical entity:
a population-based study of 10, 740 cases. Thyroid 2013;23:
1263-8.
3. Lang BH, Lo CY, Chan WF, Lam AK, Wan KY. Classical and fol- licular variant of papillary thyroid carcinoma: a comparative study on clinicopathologic features and long-term outcome.
World J Surg 2006;30:752-8.
4. Haugen BR, Alexander EK, Bible KC, Doherty GM, Mandel SJ, Nikiforov YE, et al. 2015 American thyroid association manage- ment guidelines for adult patients with thyroid nodules and dif- ferentiated thyroid cancer: The American thyroid association guidelines task force on thyroid nodules and differentiated thy- roid cancer. Thyroid 2016;26:1-133.
5. Nikiforov YE, Seethala RR, Tallini G, Baloch ZW, Basolo F, Thompson LD, et al. Nomenclature revision for encapsulated follicular variant of papillary thyroid carcinoma: a paradigm
shift to reduce overtreatment of indolent tumors. JAMA Oncol 2016;2:1023-9.
6. Manimaran D, Karthinkeyan TM, Khan DM, Raman R T.
Follicular variant of papillary thyroid carcinoma: cytological in- dicators of diagnostic value. J Clin Diagn Res 2014;8:46-8.
7. Ustun B, Chhieng D, Prasad ML, Holt E, Hammers L, Carling T, et al. Follicular variant of papillary thyroid carcinoma: accuracy of FNA diagnosis and implications for patient management.
Endocr Pathol 2014;25:257-64.
8. Vivero M, Kraft S, Barletta JA. Risk stratification of follicular var- iant of papillary thyroid carcinoma. Thyroid 2013;23:273-9.
9. Liu J, Singh B, Tallini G, Carlson DL, Katabi N, Shaha A, et al.
Follicular variant of papillary thyroid carcinoma: a clin- icopathologic study of a problematic entity. Cancer 2006;107:
1255-64.
10. Finnerty BM, Kleiman DA, Scognamiglio T, Aronova A, Beninato T, Fahey TJ 3rd, et al. Navigating the management of follicular variant papillary thyroid carcinoma subtypes: a classic PTC comparison. Ann Surg Oncol 2015;22:1200-6.
11. Rhee SJ, Hahn SY, Ko ES, Ryu JW, Ko EY, Shin JH. Follicular var- iant of papillary thyroid carcinoma: distinct biologic behavior based on ultrasonographic features. Thyroid 2014;24:683-8.