Copyright © 2014 Korean Neurological Association 55
Print ISSN 1738-6586 / On-line ISSN 2005-5013 http://dx.doi.org/10.3988/jcn.2014.10.1.55 CASE REPORT
J Clin Neurol 2014;10:55-58
Introduction
Brain abscesses classically result from extension of nearby infection in the head, penetrating head injury, neurosurgery, or hematogenous spread from a remote infectious source through right-to-left shunting.1 However, up to 30% of brain abscesses have no such associations and thus are deemed cryp- togenic.3
Examples of right-to-left shunting are cyanotic heart dis- ease and pulmonary arteriovenous malformations (PAVMs),1,4 which form the basis of current recommendations for pro- phylactic antibiotics in patients with such conditions and for prophylactic closure of PAVMs.5 We report an unusual case of a right-to-left shunt found in the setting of a cryptogenic brain abscess.
Case Report
A 47-year-old woman presented with worsening headache and
neck pain over 4 days associated with nausea and vomiting.
She denied subjective fevers or chills. She reported traveling to the Dominican Republic 1 month prior to presentation. She had no other medical history and was not on any medications.
She denied any recent illnesses or dental procedures.
Her temperature was 38.0ºC, heart rate was 70 beats/min, re- spiratory rate was 18/min, and blood pressures were 140/72 mm Hg. The patient had no evident toxicity and was alert and oriented to person and time but not to place. An oral exami- nation showed good dentition with no notable abscess, pain, or gingival disease. A cardiovascular examination revealed no abnormalities, including murmurs. There was no evidence of skin infections or lesions. She had mild expressive aphasia with clear, unpressured speech. Reception and comprehension were intact. Her cranial nerves and the results of motor and sensory examinations were normal. However, she did have a shuffling gait with loss of balance to the right and clonus at the right ankle.
The laboratory parameters of the patient at admission were remarkable for leukocytosis with a left shift (17.8×109 WBCs per liter and 90% neutrophils). The results of electrocardio- gram and chest X-ray examinations were normal. Computed tomography (CT) of the brain without contrast agent demon- strated a left thalamic mass with a hypodense center and hy-
Novel Partial Anomalous Pulmonary Venous Connection Associated with Brain Abscess
Anish Koka,a Amit Sachdev,b Moussa F Yazbeck,b Rodney D Bell,b Christopher Farrellc
aDepartments of Cardiology, bNeurology, and cNeurosurgery, Thomas Jefferson University, Philadelphia, PA, USA
Received March 29, 2012 Revised June 22, 2012 Accepted June 22, 2012 Correspondence Anish Koka, MD
Department of Cardiology, Thomas Jefferson University, Suite 105, 829 Spruce St., Philadelphia, PA 19107, USA Tel +1-215-829-3530 Fax +1-215-829-3090
E-mail [email protected]
BackgroundzzRight-to-left vascular shunts are associated with brain abscess.
Case ReportzzWe present a 47-year-old female with a cryptogenic left thalamic abscess on which Streptococcus mitis grew upon aspiration. Computed tomography of the chest with con- trast agent revealed an anomalous connection between the left superior pulmonary and brachio- cephalic veins. A right-to-left shunt was confirmed in a transthoracic echocardiogram study in which bubbles were injected into the left arm; this shunt had not previously been noted upon right-arm injection.
ConclusionszzWe recommend aggressive evaluation for right-to-left shunts in patients who present with cryptogenic brain abscesses. In addition to imaging, this should include a bubble- based study with left-arm saline injection. J Clin Neurol 2014;10:55-58 Key Wordszz cryptogenic, brain abscess, pulmonary shunt.
Open Access
cc This is an Open Access article distributed under the terms of the Cre- ative Commons Attribution Non-Commercial License (http://creative- commons.org/licenses/by-nc/3.0) which permits unrestricted non-com- mercial use, distribution, and reproduction in any medium, provided the ori- ginal work is properly cited.
Venous Connection Associated with Brain Abscess
56 J Clin Neurol 2014;10:55-58
A
C
E
B
D
Fig. 1. A: Computed tomography an- giogram of the chest. Arrow indicates an anomalous pulmonary venous con- nection. B: 3-D false-color reconstruc- tion of panel A. Arrow indicates an anomalous pulmonary venous connec- tion. C: Postcontrast T1-weighted trans- verse MRI scan with rim-enhanced left- side lesion. D: Postcontrast T1-weighted sagittal MRI scan with rim-enhanced left-side lesion. E: 2-D echocardiogram obtained during left-side injection of agitated normal saline.
perdense periphery. A mass effect was noted on the left later- al and third ventricles. Well-aerated paranasal sinuses and mastoid cells were noted. Magnetic resonance imaging of the brain with and without contrast agent revealed a 2.4×2.2×
1.9-cm lesion with mild surrounding hyperintense T2- weighted and fluid-attenuated-inversion-recovery (FLAIR) signals compatible with edema (Fig. 1). The enhanced rim demonstrated a hypointense T2-weighted signal. The internal contents of the lesion were hyperintense on T2-weighted and FLAIR signals with corresponding restricted diffusion. These
imaging findings were highly suggestive of a brain abscess.
Stereotactically guided drainage was applied immediately to the patient. Five milliliters of foul-smelling, purulent fluid was aspirated. The patient was initially started on vancomycin, ceftriaxone, and metronidazole after cultures were obtained.
Streptococcus mitis grew in these cultures, and so the antibiot- ic coverage was appropriately narrowed.
The patient subsequently underwent transthoracic echocar- diography (TTE) and transesophageal echocardiography with agitated-saline contrast agent injected into the right arm; the
Koka A et al.
www.thejcn.com 57 results were unrevealing. A CT scan of the chest was per-
formed with contrast agent on postoperative day 13 due to a transient episode of hypoxia, which revealed an incidental finding of an anomalous connection between the left brachio- cephalic vein and the left superior pulmonary vein. No PAVMs were noted.
Diagnostic cardiac catheterization via the left basilic vein confirmed the anomalous venous connection and the presence of a predominantly left-to-right shunt based on measurement of the oxygen saturation. TTE with agitated saline injected into the left arm this time demonstrated the passage of a large amount of bubbles into the left side of the heart. The patient recovered well after abscess drainage and was discharged to a rehabilitation facility with plans for close follow-up, and eventual percutaneous closure of the anomalous connection.
Discussion
Bacteremia secondary to gingival or other dental disease may lead to brain abscess due to seeding of bacteria via valveless emissary veins that allow direct flow into the venous drainage system of the brain.1,6 Similarly, bacteremia from more-dis- tant infections may bypass typical pulmonary filtration via anomalies that allow right-to-left shunting [e.g., cyanotic con- genital heart disease, PAVMs, patent foramen ovale (PFO), and persistent venous connections to the arterial system];
thereby gaining access to the arterial structures of the brain.1,4 The idea that a right-to-left shunt may predispose to cere- bral abscesses has long been presumed in patients with cya- notic congenital heart disease. Cyanotic heart disease has ac- counted for 12.8–69.4% of all cases of brain abscesses in several series,7 and the incidence of brain abscess in patients with cyanotic heart disease has been reported to range be- tween 5% and 18.7%.8
Similarly, PAVMs have been noted to be associated with
both cerebral infarcts and abscesses. In one large series, the prevalence rates of cerebral abscess were 8% and 16% in pa- tients with a single and multiple PAVMs, respectively.9 The standard recommended care regimen at high-volume centers is closure of PAVMs prophylactically in order to reduce their cerebral complications.5
While the latter two groups of patients appear to implicate persistent right-to-left shunts in the pathogenesis of brain ab- scesses, it has only recently been appreciated that intermit- tent right-to left-shunts may also predispose patients to ab- scesses. Kawamata et al.1 were the first to report two patients with cryptogenic brain abscesses that had PFOs, and suggest- ed that brain abscesses can arise from paradoxical emboli across a PFO. Several case reports have since noted the pres- ence of PFOs associated with cryptogenic brain abscesses.1,4,10 Most compellingly, Mahadevan et al.11 reported on a series of 68 consecutive patients with cerebral abscesses. Of their eight cryptogenic abscesses, seven had evidence of right-to-left shunting: five PFOs, one PAVM, and one persistent shunt from the superior vena cava (SVC) to the left atrium.
Another conduit for intermittent right-to-left shunting in- volves anomalous systemic venous connections. The most common anomaly of the superior caval circulation is persis- tence of the left SVC (Table 1).12 Most (92%) of the left SVCs drain into the right atrium via the coronary sinus, which ap- pears echocardiographically as a dilated coronary sinus. The remaining 8% drain directly into the left atrium, creating a right-to-left shunt that has been reported to be associated with cerebral abscess.10
We have reported a novel anomalous venous connection as- sociated with a cerebral abscess. Connection of the pulmonary veins to the systemic venous circulation is rare, and repre- sents a type of partial anomalous pulmonary venous connec- tion. The four most-common conduits in order of decreasing frequency are 1) pulmonary veins from the right upper and/
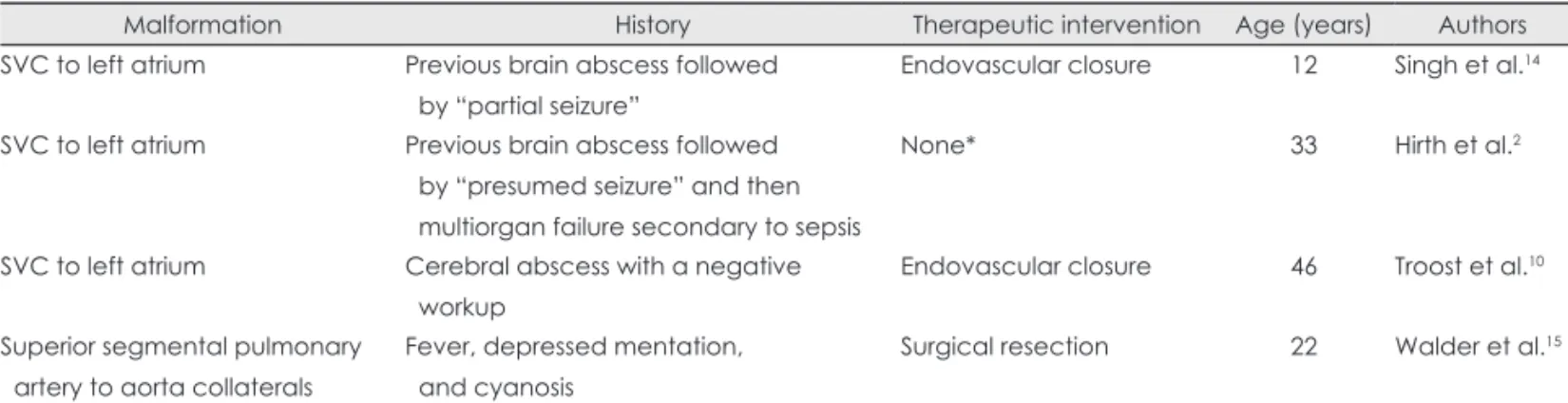
Table 1. Previously reported vascular malformations
Malformation History Therapeutic intervention Age (years) Authors
SVC to left atrium Previous brain abscess followed by “partial seizure”
Endovascular closure 12 Singh et al.14
SVC to left atrium Previous brain abscess followed by “presumed seizure” and then multiorgan failure secondary to sepsis
None* 33 Hirth et al.2
SVC to left atrium Cerebral abscess with a negative workup
Endovascular closure 46 Troost et al.10
Superior segmental pulmonary artery to aorta collaterals
Fever, depressed mentation, and cyanosis
Surgical resection 22 Walder et al.15 Previously reported cardiopulmonary vascular malformations associated with brain abscess excluding HHT, hepatopulmonary syn- drome, structural heart disease, and congenital pulmonary artery-vein complexes. In total, 186 articles dating back to 1893 were re- viewed.
*No intervention secondary to death.
HHT: hereditary haemorrhagic teleangiectasia, SVC: superior vena cava.
Venous Connection Associated with Brain Abscess
58 J Clin Neurol 2014;10:55-58
or middle lobe to the SVC, usually with a sinus venosus atrial septal defect, 2) all of the right pulmonary veins to the right atrium, 3) all of the right pulmonary veins to the inferior vena cava, and 4) the left upper or both left pulmonary veins drain- ing via an anomalous vertical vein to the left brachiocephalic vein13 (as in our case).
The case reported herein is also notable for the negative re- sults obtained in a bubble-based study involving right-arm in- jection-the right-to-left shunt was only revealed after injecting agitated-saline contrast agent into the left arm. Since right-to- left shunts are strongly associated with cryptogenic brain ab- scesses, an aggressive evaluation that includes imaging and a bubble-based study with left-arm injection should be consid- ered in such cases. This approach could facilitate both defin- ing the pathogenesis and tailoring treatment for cryptogenic brain abscesses.
Conflicts of Interest
The authors have no financial conflicts of interest.
REFERENCES
1. Kawamata T, Takeshita M, Ishizuka N, Hori T. Patent foramen ovale as a possible risk factor for cryptogenic brain abscess: report of two cases. Neurosurgery 2001;49:204-206; discussion 206-207.
2. Hirth A, Disney P, Thorne S. Brain abscess associated with an unusu- al cause of right to left shunt. Heart 2007;93:34.
3. Mathisen GE, Johnson JP. Brain abscess. Clin Infect Dis 1997;25:
763-779; quiz 780-781.
4. Sung CW, Jung JH, Lee SH, Choi S, Cho JR, Lee N, et al. Brain ab- scess in an adult with atrial septal defect. Clin Cardiol 2010;33:E51- 5. Trerotola SO, Pyeritz RE. PAVM embolization: an update. AJR Am J E53.
Roentgenol 2010;195:837-845.
6. Whitfield P. The management of intracranial abscesses. Adv Clin Neurosci Rehabil 2005;5:12-15.
7. Aebi C, Kaufmann F, Schaad UB. Brain abscess in childhood--long- term experiences. Eur J Pediatr 1991;150:282-286.
8. Takeshita M, Kagawa M, Yonetani H, Izawa M, Yato S, Nakanishi T, et al. Risk factors for brain abscess in patients with congenital cya- notic heart disease. Neurol Med Chir (Tokyo) 1992;32:667-670.
9. Moussouttas M, Fayad P, Rosenblatt M, Hashimoto M, Pollak J, Henderson K, et al. Pulmonary arteriovenous malformations: cere- bral ischemia and neurologic manifestations. Neurology 2000;55:
959-964.
10. Troost E, Gewillig M, Budts W. Percutaneous closure of a persistent left superior vena cava connected to the left atrium. Int J Cardiol 2006;
106:365-366.
11. Mahadevan G, Thorne SA, Steeds RP. Echocardiography in crypto- genic cerebrospinal abscess. J Am Soc Echocardiogr 2008;21:401-403.
12. Kaiser LR, Kron IL, Spray TL. Mastery of Cardiothoracic Surgery.
2nd ed. Philadelphia: Lippincott Williams & Wilkins, 2006.
13. Walsh R, Fang J, Fuster V, O’Rourke R. Hurst’s the Heart. 13th ed.
New York: McGraw-Hill, 2011.
14. Singh S, Geelani MA, Modi P, Niwaria Y, Shahi S, Banerjee A. Anom- alous connection of superior vena cava to the left atrium masquerading as epilepsy: a case report with review of literature. Ann Card Anaesth 2008;11:42-45.
15. Walder LA, Anastasia LF, Spodick DH. Pulmonary arteriovenous mal- formations with brain abscess. Am Heart J 1994;127:227-232.