doi: 10.1253/circj.CJ-18-1303
comes from the Harmonizing Optimal Strategy for Treat-ment of Coronary Artery Stenosis–Safety & Effectiveness of Drug-Eluting Stents & Anti-platelet Regimen (HOST– ASSURE) randomized controlled trial (RCT), in which the PtCr-EES (Promus Element, Boston Scientific, Natick,
T
he platinum chromium (PtCr) alloy has greater radial strength, radio-opacity, and flexibility com-pared with the cobalt chromium (CoCr) alloy, which may result in potential advantages when developed into coronary stents. We previously reported the 1-yearout-Received January 9, 2019; revised manuscript received March 22, 2019; accepted April 9, 2019; J-STAGE Advance Publication released online May 31, 2019 Time for primary review: 18 days
VHS Medical Center, Seoul (C.H.K.); Seoul National University Hospital, Seoul (K.W.P., J.K., H.-S.K.); Dankook University Hospital, Cheonan (B.-E.P.); Busan National University Hospital, Busan (K.S.C.); Presbyterian Medical Center, Jeonju (J.Y.R.); Uijeongbu St. Mary’s Hospital, Uijeongbu (H.-K.J.); Ulsan Hospital, Ulsan (E.-S.S.); Samsung Changwon Hospital, Changwon (J.H.O.); Chonnam National University Hospital, Gwangju (M.-H.J.); Boramae Medical Center, Seoul (S.K.); Chungbuk National University Hospital, Cheongju (K.-K.H.); Wonju Christian Hospital, Wonju (J.-H.Y.); Inje University Ilsan Paik Hospital, Goyang (S.Y.L.); Dong-A Medical Center, Busan (T.-H.P.); St. Vincent’s Hospital, Suwon (K.W.M.); Gangnam Severance Hospital, Seoul (H.-M.K.); Keimyung University Dongsan Medical Center, Daegu (S.-H.H.); Daegu Catholic University Medical Center, Daegu (J.-K.R.); Daegu Fatima Hospital, Daegu (B.-R.L.); Gyeongsang National University Hospital, Jinju (Y.W.P.); and Seoul National University Bundang Hospital, Seongnam (I.-H.C.), Republic of Korea
(Footnote continued the next page.)
Long-Term Comparison of Platinum Chromium
Everolimus-Eluting Stent vs. Cobalt Chromium
Zotarolimus-Eluting Stent
― 3-Year Outcomes From the HOST–ASSURE
Randomized Clinical Trial ―
Chee Hae Kim, MD; Kyung Woo Park, MD, PhD; Jeehoon Kang, MD; Byoung-Eun Park, MD, PhD; Kwang Soo Cha, MD, PhD; Jay Young Rhew, MD, PhD; Hui-Kyung Jeon, MD, PhD;
Eun-Seok Shin, MD, PhD; Ju Hyeon Oh, MD, PhD; Myung-Ho Jeong, MD, PhD; Sanghyun Kim, MD, PhD; Kyung-Kuk Hwang, MD, PhD; Jung-Han Yoon, MD, PhD;
Sung Yun Lee, MD, PhD; Tae-Ho Park, MD, PhD; Keon Woong Moon, MD, PhD; Hyuck-Moon Kwon, MD, PhD; Seung-Ho Hur, MD, PhD; Jae-Kean Ryu, MD, PhD;
Bong-Ryul Lee, MD, PhD; Yong Whi Park, MD, PhD; In-Ho Chae, MD, PhD; Hyo-Soo Kim, MD, PhD on behalf of the HOST–ASSURE Investigators
Background: There are limited data on the long-term outcome of platinum chromium-based everolimus-eluting stents (PtCr-EES) vs. cobalt chromium-based zotarolimus-eluting stents (CoCr-ZES).
Methods and Results: A total of 3,755 patients undergoing percutaneous coronary intervention (PCI) were randomized 2:1 to PtCr-EES or CoCr-ZES, and 96.0% of patients completed the 3-year clinical follow-up. The primary outcome was target lesion failure (TLF), defined as a composite of cardiac death, target vessel-related myocardial infarction (MI), and clinically-driven target lesion revascular-ization (TLR). At 3 years, TLF occurred in 5.3% and in 5.4% of the PtCr-EES and CoCr-ZES groups, respectively (hazard ratio 0.978; 95% confidence interval 0.730–1.310, P=0.919). There were no significant differences in the individual components of TLF. Routine angiographic follow-up was performed in 38.9% of the total patients. In a landmark analysis of the subgroup that had follow-up angiography, the clinically-driven TLR rate of CoCr-ZES was significantly higher than PtCr-EES group during the angiography follow-up period (P=0.009). Overall definite and probable stent thrombosis rates were very low in both groups (0.5% vs. 0.6%, P=0.677). Conclusions: PtCr-EES and CoCr-ZES had similar and excellent long-term outcomes in both efficacy and safety after PCI in an all-comer population.
Key Words: Clinical outcome; Cobalt chromium-based zotarolimus-eluting stent; Drug-eluting stent; Percutaneous coronary intervention; Platinum chromium-based everolimus-eluting stent
1490 KIM CH et al. Angiography
Quantitative analysis of angiographic images was per-formed at a central core laboratory, the Seoul National University Hospital by specialized technicians who were unaware of the purpose of this study and used validated software (CAAS 5.7., Pie Medical Imaging, Maastricht, The Netherlands). A longitudinal stent deformity (LSD) was defined as any inconsistency in the radiodensity pat-tern along the length of the stent, or other gross irregulari-ties or deformiirregulari-ties.
Statistical Analysis
Continuous variables are presented as mean ± SD and com-pared using Student’s t-test. Categorical variables are pre-sented as counts with percentages and compared using chi-square or Fisher’s exact test, as appropriate. Hazard ratios (HR) with 95% confidence intervals (CI) were esti-mated using the Cox proportional-hazards method. Cumu-lative event rates were estimated using the Kaplan-Meier method. Time-to-event curves were compared using log-rank tests. In patients undergoing routine angiography follow-up, landmark analyses (3 periods: before, during and after routine angiography follow-up period) were per-formed to determine whether there was a difference in out-comes according to the allocated stent during the routine angiography follow-up period. All analyses were performed using SPSS version 22.0 (IBM Co., Armonk, NY, USA).
Results
Baseline Characteristics and Procedures
A total of 3,755 patients were enrolled at 40 centers in South Korea from June 2010 to November 2011. These patients were randomly allocated to PtCr-EES (2,503 patients) or CoCr-ZES (1,252 patients). A flowchart of the study is provided in Figure 1; 96.0% (3,606/3,755 patients, PtCr-EES group: 96.0% and CoCr-ZES group: 96.2%) of the enrolled patients completed the 3-year follow-up. The baseline patient characteristics are shown in Table 1. There was no difference in demographic characteristics except for the frequency of males and current smokers, who were more frequent in the PtCr-EES group. Table 2 shows the baseline lesional and procedural characteristics. The detailed angiographic parameters were noted in our previ-ous report and there were no significant differences between the 2 groups.3
The regimen of antiplatelet therapy during follow-up is summarized in Supplementary Table 1. Patients received, in addition to aspirin, either double-dose clopidogrel or single dose clopidogrel+cilostazol for the first month post-PCI and then were recommended to receive conventional DAPT up to 1 year. The 2 groups showed similar rates of DAPT at both 1 year and 3 years (% of patients on DAPT: 91.6% and 49.2% at 1-year and 3-year follow-up, respectively). Clinical Outcomes at 3 Years
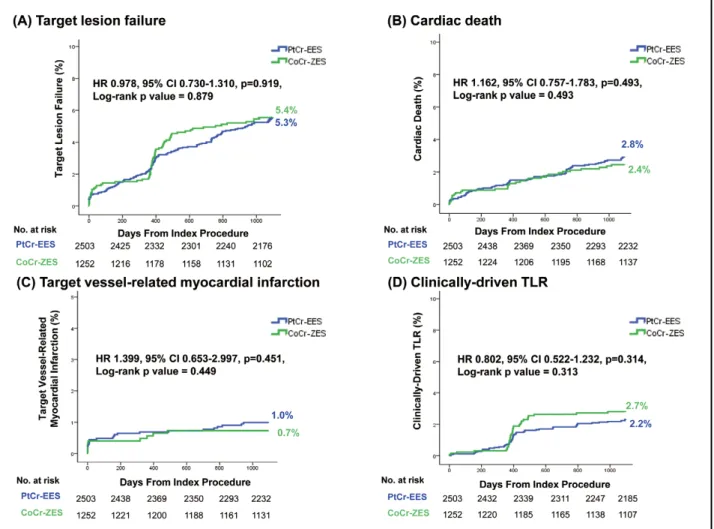
At 3 years, TLF had occurred in 5.3% and 5.4% of the population in the PtCr-EES and CoCr-ZES groups, respec-tively (HR 0.978, 95% CI 0.730–1.310, P=0.919) (Table 3; Figure 2A). There were no significant differences in the indi-MA, USA) was non-inferior to the CoCr-EES in terms of
target lesion failure (TLF) with very low rates of stent thrombosis (ST) in patients undergoing percutaneous cor-onary intervention (PCI).1–3 This study reports the long-term 3-year outcomes of PtCr-EES vs. CoCr-ZES in all-comers undergoing PCI. Additionally, this was the first long-term comparison of these stents in an Asian population.
Methods
Study Design
The HOST–ASSURE was a prospective, randomized, single-blind, blinded endpoint evaluation, multicenter trial conducted at 40 sites in South Korea. The study was an all-comers study, with a 2×2 design of the type of drug-eluting stent (DES) and the type of 1-month intensified antiplatelet therapy followed by conventional dual anti-platelet therapy (DAPT).1 Major exclusion criteria were severe left ventricular systolic dysfunction, cardiogenic shock, symptomatic heart failure, and an increased risk of bleeding. Participants were randomized 2:1 to PtCr-EES or CoCr-ZES and 1:1 to triple antiplatelet therapy or double-dose DAPT. The study was approved by the ethics com-mittees at the participating centers and was performed in accordance with the Declaration of Helsinki. Written informed consent was given by all participants.
Procedures and Endpoints
Participants were randomly assigned to the PtCr-EES or CoCr-ZES group by a web-based online randomization system after diagnostic angiography. After the first month of intensified antiplatelet therapy, maintenance of DAPT was left to the discretion of individual physicians with a general recommendation of at least 1 year. PCI was per-formed according to standard techniques using standard devices by physician’s decision. The primary endpoint was TLF, a composite of cardiac death, target vessel-related myocardial infarction (TV-MI), and clinically-driven target lesion revascularization (TLR). Clinically-driven TLR was defined as a revascularization procedure with at least one of the following: (1) recurrence of chest pain; (2) positive non-invasive test; and (3) angiographically significant stenosis with diameter >70%, for which PCI was deemed necessary. Secondary endpoints included all of the indi-vidual components of the primary endpoint as well as ST, patient-oriented clinical outcome (POCO), and all compo-nents of POCO (all-cause death, all-cause MI, and any repeat revascularization). All deaths were considered cardiac unless a definite non-cardiac cause could be estab-lished. ST was defined as definite or probable according to the Academic Research Consortium (ARC) classification.4 An independent clinical event adjudication committee, whose members were unaware of the study group assign-ments, assessed all of the clinical endpoints. The primary analysis was on an intention-to-treat basis. Routine angio-graphic follow-up was not mandated, but if performed, was recommended to be done at 12–15 months after the index procedure according to the individual treating physi-cians’ judgment.
Clinical Trial Registration Information: HOST–ASSURE trial (https://clinicaltrials.gov/ct2/show/NCT01267734, NCT01267734) Mailing address: Professor Kyung Woo Park, MD, PhD, Department of Internal Medicine, Cardiovascular Center, Seoul National
University Hospital, 101 Daehak-ro, Jongro-gu, Seoul 110-744, Republic of Korea. E-mail: [email protected] ISSN-1346-9843 All rights are reserved to the Japanese Circulation Society. For permissions, please e-mail: [email protected]
Figure 1. Study flowchart. CoCr-ZES, cobalt chromium-based zotarolimus-eluting stent; PtCr-EES, platinum chromium-based everolimus-eluting stent.
Table 1. Baseline Demographic Characteristics
PtCr-EES (n=2,503) CoCr-ZES (n=1,252) P value Age, years 63.1±10.8 60.78±9.68 0.312 Male 1,746 (69.8) 820 (65.6) 0.010 BMI, kg/m2 24.6±3.2 24.7±3.2 0.189 Hypertension 1,706 (68.2) 852 (68.1) 0.862 Diabetes 795 (31.8) 401 (32.0) 0.862 Dyslipidemia 1,601 (64.0) 822 (65.7) 0.335 Current smoker 823 (32.9) 369 (29.5) 0.040 Chronic renal failure 59 (2.4) 36 (2.9) 0.283 Peripheral artery disease 41 (1.6) 27 (2.2) 0.263 Cerebrovascular disease 172 (6.9) 79 (6.3) 0.486 Previous PCI 247 (9.9) 120 (9.6) 0.691 Previous CABG surgery 16 (0.6) 10 (0.8) 0.580 Previous MI 116 (4.6) 49 (3.9) 0.338 Congestive heart failure 41 (1.6) 13 (1.0) 0.123 Clinical diagnosis 0.708 Silent ischemia 119 (4.8) 63 (5.0) Stable angina 746 (29.8) 367 (29.3) Unstable angina 903 (36.1) 476 (38.0) NSTEMI 452 (18.1) 209 (16.7) STEMI 283 (11.3) 137 (10.9)
Acute coronary syndrome 1,645 (65.4) 828 (65.7) 0.827 Values are given as mean ± standard deviation or n (%). BMI, body mass index; CABG, coronary artery bypass graft; CoCr-ZES, cobalt chromium-based zotarolimus-eluting stent; PCI, percutaneous coronary intervention; PtCr-EES, platinum chromium-based everolimus-eluting stent; NSTEMI, non-ST-segment elevation myocardial infarction; STEMI, ST-segment elevation myocardial infarction.
1492 KIM CH et al.
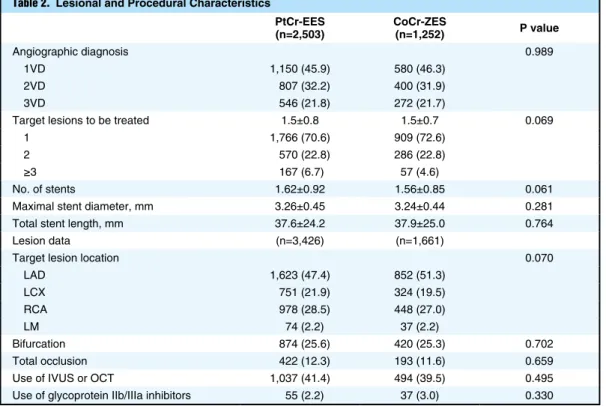
Table 2. Lesional and Procedural Characteristics
PtCr-EES (n=2,503) CoCr-ZES (n=1,252) P value Angiographic diagnosis 0.989 1VD 1,150 (45.9) 580 (46.3) 2VD 807 (32.2) 400 (31.9) 3VD 546 (21.8) 272 (21.7)
Target lesions to be treated 1.5±0.8 1.5±0.7 0.069 1 1,766 (70.6) 909 (72.6)
2 570 (22.8) 286 (22.8) ≥3 167 (6.7) 57 (4.6)
No. of stents 1.62±0.92 1.56±0.85 0.061 Maximal stent diameter, mm 3.26±0.45 3.24±0.44 0.281 Total stent length, mm 37.6±24.2 37.9±25.0 0.764 Lesion data (n=3,426) (n=1,661)
Target lesion location 0.070 LAD 1,623 (47.4) 852 (51.3) LCX 751 (21.9) 324 (19.5) RCA 978 (28.5) 448 (27.0) LM 74 (2.2) 37 (2.2) Bifurcation 874 (25.6) 420 (25.3) 0.702 Total occlusion 422 (12.3) 193 (11.6) 0.659 Use of IVUS or OCT 1,037 (41.4) 494 (39.5) 0.495 Use of glycoprotein IIb/IIIa inhibitors 55 (2.2) 37 (3.0) 0.330 Values are given as mean ± standard deviation or n (%). CoCr-ZES, cobalt chromium-based zotarolimus-eluting stent; IVUS, intravascular ultrasound; LAD, left anterior descending artery; LCX, left circumflex artery; LM, left main artery; OCT, optical coherence tomography; PtCr-EES, platinum chromium-based everolimus-eluting stent; RCA, right coro-nary artery.
Table 3. Cumulative Incidence of Clinical Events Up to 3 Years PtCr-EES
(n=2,503) CoCr-ZES (n=1,252) (95% CI)HR P value
TLF 132 (5.3) 68 (5.4) 0.978 (0.730–1.310) 0.919 Patient-oriented clinical outcome 316 (12.6) 163 (13.0) 0.975 (0.807–1.178) 0.797 All-cause death 121 (4.8) 42 (3.4) 1.456 (1.025–2.069) 0.036 Cardiac 69 (2.8) 30 (2.4) 1.162 (0.757–1.783) 0.493 Non-cardiac 52 (2.1) 12 (1.0) 2.193 (1.170–4.107) 0.014 All-cause MI 43 (1.7) 20 (1.6) 1.085 (0.638–1.845) 0.762 Target vessel-related MI 24 (1.0) 9 (0.7) 1.343 (0.624–2.889) 0.451 Repeat revascularization 190 (7.6) 114 (9.1) 0.837 (0.663–1.056) 0.133 TLR 95 (3.8) 52 (4.2) 0.925 (0.660–1.297) 0.652 Clinically-driven repeat revascularization 97 (3.9) 64 (5.1) 0.763 (0.556–1.046) 0.093 Clinically-driven TLR 54 (2.2) 34 (2.7) 0.802 (0.522–1.232) 0.314 Definite or probable ST 13 (0.5) 7 (0.6) 0.839 (0.367–1.917) 0.677 Cerebrovascular accident 32 (1.3) 14 (1.1) 1.084 (0.575–2.045) 0.803 Ischemic 27 (1.1) 9 (0.7) 1.462 (0.685–3.120) 0.326 Hemorrhagic 5 (0.2) 2 (0.2) 1.012 (0.185–5.527) 0.989 All PLATO bleeding 63 (2.5) 27 (2.2) 1.220 (0.773–1.927) 0.394 Major bleeding 25 (1.0) 13 (1.0) 1.048 (0.527–2.087) 0.893 Major, life-threatening 3 (0.1) 4 (0.3) 0.507 (0.102–2.512) 0.405 Values are n (%). Target lesion failure (TLF) was a composite of cardiac death, target vessel-related myocardial infarction (TV-MI), and clinically-driven TLR; patient-oriented clinical outcome was a composite of all-cause death, all-cause MI, and any repeat revascularization. CoCr-ZES, cobalt chromium-based zotarolimus-eluting stent; PtCr-EES, platinum chromium-based everolimus-eluting stent; PLATO, PLATelet inhibition and patient Outcomes; ST, stent thrombosis; TLR, target lesion revascularization.
continued DAPT until 1 year after PCI, and were on aspirin monotherapy at the time of the event. Details of the indi-vidual cases of ST are described in Supplementary Table 4. Landmark Analyses of 1–3-Year Clinical Outcomes
Landmark analyses were performed from 1 year to 3 years. TLF occurred in 3.1% and 3.6% of the population in the PtCr-EES and CoCr-ZES groups, respectively (HR 0.881, 95% CI 0.605–1.281, P=0.506). There were no significant differences in the individual components of TLF from 1 year to 3 years (cardiac death, 1.4% vs. 1.0%, P=0.731; TV-MI, 0.1% vs. 0.2%, P=0.472; clinically-driven TLR, 0.9% vs. 1.5%, P=0.122).
Routine Angiography Follow-up
Although routine follow-up coronary angiography was not mandated, it was performed in 38.9% of the patients (median time from index PCI: 402 days, interquartile range: 41 days), and in 38 (95.0%) of the 40 centers. The decision to perform routine coronary angiography was up to each individual physician’s discretion. The proportion of patients having routine angiographic follow-up was similar between the 2 stent groups (38.2% vs. 40.4% in PtCr-EES vs. CoCr-ZES, P=0.190). In this group of vidual components of TLF (cardiac death, 2.8% vs. 2.4%,
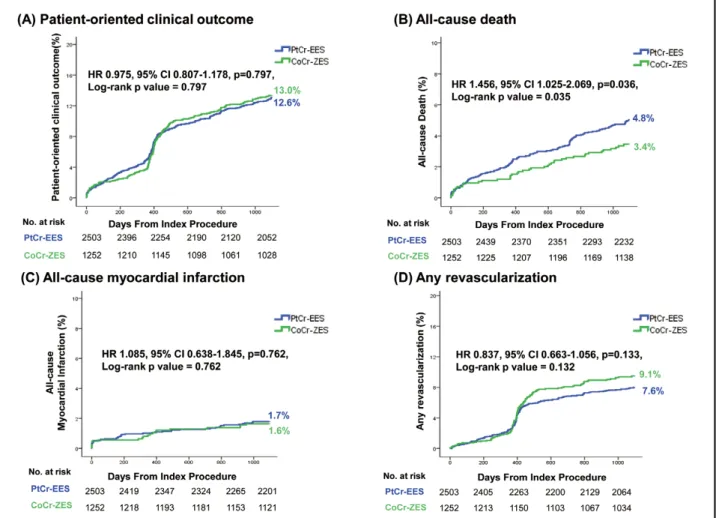
P=0.493; TV-MI, 1.0% vs. 0.7%, P=0.451; clinically-driven TLR, 2.2% vs. 2.7%, P=0.314; Figure 2B–D). POCO was also comparable between the 2 groups, and occurred in 12.6% and 13.0% of the PtCr-EES and CoCr-ZES groups, respectively (HR 0.975, 95% CI 0.807–1.178, P=0.797; Figure 3A). Among the individual components of POCO, rates of all-cause MI (1.7% vs. 1.6%, P=0.762) and any revas-cularization (7.6% vs. 9.1%, P=0.133) were similar between the groups (Figure 3C,D). However, the rate of all-cause death was higher in the PtCr-EES group (4.8% vs. 3.4%; HR 1.456, 95% CI 1.025–2.069, P=0.036; Figure 3B). This was because of a significant difference in the occurrence of non-cardiac death (2.1% vs 1.0%, P=0.014). The specific causes of non-cardiac deaths are summarized in Supplementary Table 2. Subgroup analyses of TLF showed consistent findings with no significant interaction between the different subgroups and the allocated stent (Supplementary Table 3). ARC-defined definite and probable ST rates were very low, and occurred in 0.5% and 0.6% in the PtCr-EES and CoCr-ZES groups, respectively (P=0.677, Supplementary Figure). There were 3 cases of very late definite ST in the PtCr-EES group, occurring on days 701, 787, and 932 from the index proce-dure, but not in the CoCr-ZES group. All these patients
Figure 2. Kaplan-Meier curves of target lesion failure (TLF) and individual components of TLF. (A) TLF, (B) cardiac death, (C) target vessel-related myocardial infarction, (D) clinically-driven target lesion revascularization (TLR). CoCr-ZES, cobalt chromium-based zotarolimus-eluting stent; PtCr-EES, platinum chromium-chromium-based everolimus-eluting stent.
1494 KIM CH et al.
Figure 4. Landmark analyses of TLF and driven TLR in patients with routine angiography follow-up. (A) TLF, (B) clinically-driven TLR. Abbreviations as in Figure 2.
Figure 3. Kaplan-Meier curves of patient-oriented clinical outcome (POCO) and its individual components. (A) POCO, (B) all-cause death, (C) all-all-cause myocardial infarction, (D) any revascularization. CoCr-ZES, cobalt chromium-based zotarolimus-eluting stent; PtCr-EES, platinum chromium-based everolimus-eluting stent.
TLF.3 Also, the 2-year results of the DUTCH PEERS study showed similar results, with low event rates for both PtCr-EES and CoCr-ZES.20 Our 3-year follow-up results are in line with these previous studies. Although the PtCr alloy itself has a greater radial strength and radiopacity than the CoCr alloy, it does not lead to a benefit in clinical outcome, which suggests that the general evolution in anti-proliferative drugs, polymers, use of DAPT, and proce-dural techniques, as well as in stent alloys, has contributed to the overall improvement in the outcomes of PCI.
In the current study, we found similar rates of TLF and POCO at 3 years. One finding that was not previously reported was that the repeat revascularization rates in those having routine angiographic follow-up was slightly but statistically significantly higher in the CoCr-ZES group. This phenomenon was not observed in the subgroup with-out rwith-outine angiographic follow-up. Because follow-up angiography is susceptible to the oculostenotic reflex, there is a tendency to perform repeat revascularization more frequently because of a perceived degree of angiographic stenosis, especially in stents that have slightly greater late loss. We believe that the permissive nature of the study protocol regarding angiographic follow-up and repeat revascularization may have resulted in oculostenotic PCI rather than ischemia-driven revascularization. However, our results also suggested that the CoCr-ZES may have slightly greater angiographic late luminal loss and in-stent restenosis rates than the PtCr-EES, although quantitative coronary angiographic analysis was not performed in the follow-up cases. In the literature, the reported late luminal loss of CoCr-ZES is 0.27 µm,15 which is greater than that reported for PtCr-EES (0.15 µm).21 Regarding the risk of very late definite or probable ST, the overall rates were extremely low for both stents (0.0% vs. 0.1% for CoCr-ZES vs. PtCr-EES, P=0.220), confirming the long-term safety of both stent platforms. Furthermore, it was a relief to observe no additional adverse clinical events in the 7 cases of overt LSD at baseline.
Overall, the device-oriented event rates and patient-ori-ented event rates of the current study were lower than those reported in previous trials. There may be several reasons for this. First, DAPT was maintained for a long period of time in this study (56.5% at 2 years and 49.2% at 3 years). Considering that 65% of the patients had acute coronary syndrome as the clinical presentation, and the average stent length was 28 mm per lesion and 38 mm per patient, it is not surprising that a significant proportion of the treating physicians decided to maintain DAPT for longer. Second, the patients in the present study received intensified antiplatelet therapy during the first month post-PCI. Therefore, the 1-year outcomes also showed low rates of clinical events (1-year TLF 2.9%). There may have been possible “legacy effects” of the intensified antiplatelet regi-mens beyond the first months of therapy. Third, the per-centage of patients receiving “image-guided” or at least “image-supported” PCI was 40.8%, which is significantly higher than the real-world use rate.22 It is well known from previous studies that in patients undergoing long stenting and complex PCI, imaging support can improve clinical outcomes.23 Fourth, post-procedural cardiac enzyme mea-surement was not mandated in the study, and thus post-procedural MI may not have been fully captured, which could not be confirmed, and may also have lowered the rate of TLF even further. Finally, the study was conducted in an East Asian population. It is known that East Asians patients, clinically-driven TLR occurred more frequently
in the CoCr-ZES group (P=0.009, Figure 4), while the rates were similar in those that did not have routine follow-up angiography (P=0.156). No significant interaction in the clinically-driven TLR group between routine angiography follow-up and stent type was observed (P=0.911). There was no significant difference in TLF or TLR before or after the routine angiographic follow-up period.
Long-Term Outcome of Cases With Initial Longitudinal Stent Deformation
Previously, we reported 7 cases of angiographically overt LSD at baseline, which occurred exclusively in the PtCr-EES group (2 occurred in the left main coronary artery, 4 in the left anterior descending artery (LAD), and 1 in the right coronary artery (RCA)). Of these patients, only 1 required additional stent implantation at baseline proce-dure (LAD); 3 of the patients stopped DAPT at 1 year post-PCI and 4 continued DAPT for 3 years. Of those who discontinued DAPT after 1 year, 1 patient continued aspi-rin and 2 patients continued clopidogrel as single antiplate-let treatment. At 3 years of follow-up, none of the overt LSD cases were associated with further adverse events.
Discussion
The PtCr-EES and CoCr-ZES are 2 of the most commonly implanted 2nd-generation DES. The current study reports the 3-year long-term outcomes from the HOST–ASSURE RCT, which compared these 2 stent platforms head to head for the first time in an all-comer East Asian popula-tion. The major findings of the present analysis are as fol-lows: (1) at 3 years, PtCr-EES and CoCr-ZES had similar rates of TLF, a composite of cardiac death, TV-MI, and clinically-driven TLR, and the individual components of TLF were similar between the 2 stents; (2) the rate of repeat revascularization with the CoCr-ZES was slightly higher than with the PtCr-EES but only in those undergo-ing routine angiographic follow-up, suggestundergo-ing an oculo-stenotic reflex; and (3) very late ST occurred in 3 patients in the PtCr-EES group and in none of the CoCr-ZES group. Both stents showed excellent safety with overall definite or probable ST rates below 1%.
Currently, 2nd-generation DES are the mainstay of treatment of patients with significant coronary artery dis-ease. Innovations in stent design and alloy have allowed manufacturers to reduce the strut thickness, resulting in better deliverability and conformability. Further, the incor-poration of more biocompatible polymers has resulted in less inflammatory response and vascular toxicity. This has resulted in improved clinical outcomes in both randomized studies and meta-analyses compared with bare metal stents or 1st-generation DES.5–14 Compared with the CoCr alloy, PtCr has greater radial strength, less recoil, and greater radiopacity, which may offer potential advantages in visu-alization and long-term outcomes.
In the Resolute All-Comers trial, similar results for CoCr-ZES compared with CoCr-EES were shown at 1-, 2-, 4-, and final 5-year follow-up.15–18 In the PLATINUM study, the non-inferiority of PtCr-EES to CoCr-EES in terms of safety and efficacy was shown up to 12 months post-PCI.19 However, before our study, there were no direct comparisons of CoCr-ZES and PtCr-EES. As we reported in the 1-year follow-up results of the HOST–ASSURE RCT, PtCr-EES was non-inferior to CoCr-ZES in terms of
1496 KIM CH et al. 2007; 115: 2344 – 2351.
5. Sabate M, Cequier A, Iñiguez A, Serra A, Hernandez-Antolin R, Mainar V, et al. Everolimus-eluting stent versus bare-metal stent in ST-segment elevation myocardial infarction (EXAMINATION): 1 year results of a randomised controlled trial. Lancet 2012; 380: 1482 – 1490.
6. Sabaté M, Brugaletta S, Cequier A, Iñiguez A, Serra A, Hernádez-Antolín R, et al. The EXAMINATION trial (everolimus-eluting stents versus bare-metal stents in ST-segment elevation myocar-dial infarction): 2-year results from a multicenter randomized controlled trial. JACC Cardiovasc Interv 2014; 7: 64 – 71. 7. Sabaté M, Brugaletta S, Cequier A, Iñiguez A, Serra A,
Jiménez-Quevedo P, et al. Clinical outcomes in patients with ST-segment elevation myocardial infarction treated with everolimus-eluting stents versus bare-metal stents (EXAMINATION): 5-year results of a randomised trial. Lancet 2016; 387: 357 – 366. 8. Serruys PW, Ong A, Piek JJ, Neumann FJ, van der Giessen WJ,
Wiemer M, et al. A randomized comparison of a durable poly-mer Everolimus-eluting stent with a bare metal coronary stent: The SPIRIT first trial. EuroIntervention 2005; 1: 58 – 65. 9. Serruys PW, Ruygrok P, Neuzner J, Piek JJ, Seth A, Schofer JJ,
et al. A randomised comparison of an everolimus-eluting coro-nary stent with a paclitaxel-eluting corocoro-nary stent: The SPIRIT II trial. EuroIntervention 2006; 2: 286 – 294.
10. Stone GW, Rizvi A, Sudhir K, Newman W, Applegate RJ, Cannon LA, et al. Randomized comparison of everolimus-and paclitaxel-eluting stents: 2-year follow-up from the SPIRIT (Clinical Evaluation of the XIENCE V Everolimus Eluting Cor-onary Stent System) IV trial. J Am Coll Cardiol 2011; 58: 19 – 25. 11. Gada H, Kirtane AJ, Newman W, Sanz M, Hermiller JB,
Mahaffey KW, et al. 5-year results of a randomized comparison of XIENCE V everolimus-eluting and TAXUS paclitaxel-eluting stents: Final results from the SPIRIT III trial (clinical evaluation of the XIENCE V everolimus eluting coronary stent system in the treatment of patients with de novo native coronary artery lesions). JACC Cardiovasc Interv 2013; 6: 1263 – 1266.
12. Dangas GD, Serruys PW, Kereiakes DJ, Hermiller J, Rizvi A, Newman W, et al. Meta-analysis of everolimus-eluting versus paclitaxel-eluting stents in coronary artery disease: Final 3-year results of the SPIRIT clinical trials program (Clinical Evaluation of the Xience V Everolimus Eluting Coronary Stent System in the Treatment of Patients With De Novo Native Coronary Artery Lesions). JACC Cardiovasc Interv 2013; 6: 914 – 922. 13. Park KW, Kang SH, Velders MA, Shin DH, Hahn S, Lim WH,
et al. Safety and efficacy of everolimus-versus sirolimus-eluting stents: A systematic review and meta-analysis of 11 randomized trials. Am Heart J 2013; 165: 241 – 250.e4.
14. Kang SH, Park KW, Kang DY, Lim WH, Park KT, Han JK, et al. Biodegradable-polymer drug-eluting stents vs. bare metal stents vs. durable-polymer drug-eluting stents: A systematic review and Bayesian approach network meta-analysis. Eur Heart J 2014; 35: 1147 – 1158.
15. Serruys PW, Silber S, Garg S, van Geuns RJ, Richardt G, Buszman PE, et al. Comparison of zotarolimus-eluting and evero-limus-eluting coronary stents. N Engl J Med 2010; 363: 136 – 146. 16. Silber S, Windecker S, Vranckx P, Serruys PW, RESOLUTE All Comers investigators. Unrestricted randomised use of two new generation drug-eluting coronary stents: 2-year patient-related versus stent-related outcomes from the RESOLUTE All Comers trial. Lancet 2011; 377: 1241 – 1247.
17. Taniwaki M, Stefanini GG, Silber S, Richardt G, Vranckx P, Serruys PW, et al. 4-year clinical outcomes and predictors of repeat revascularization in patients treated with new-generation drug-eluting stents: A report from the RESOLUTE All-Comers trial (A Randomized Comparison of a Zotarolimus-Eluting Stent With an Everolimus-Eluting Stent for Percutaneous Coro-nary Intervention). J Am Coll Cardiol 2014; 63: 1617 – 1625. 18. Iqbal J, Serruys PW, Silber S, Kelbaek H, Richardt G, Morel
MA, et al. Comparison of zotarolimus- and everolimus-eluting coronary stents: Final 5-year report of the RESOLUTE all-comers trial. Circ Cardiovasc Interv 2015; 8: e002230.
19. Stone GW, Teirstein PS, Meredith IT, Farah B, Dubois CL, Feldman RL, et al. A prospective, randomized evaluation of a novel everolimus-eluting coronary stent: The PLATINUM (a Prospective, Randomized, Multicenter Trial to Assess an Evero-limus-Eluting Coronary Stent System [PROMUS Element] for the Treatment of Up to Two de Novo Coronary Artery Lesions) trial. J Am Coll Cardiol 2011; 57: 1700 – 1708.
20. Sen H, Lam MK, Löwik MM, Danse PW, Jessurun GA, van Houwelingen KG, et al. Clinical events and patient-reported
can have lower rates of ischemic events after PCI, the so-called “East Asian paradox”.24,25 It has been shown in multiple trials from Korea, Japan, and China that the TLF rates are relatively low in similar clinical groups.26–30 Even though the mechanism of lower ischemic event rates in East Asians is currently unknown, differing levels of thrombogenicity such as lower baseline inflammatory sta-tus, response to antiplatelet therapy, and hypercoagulabil-ity according to ethnichypercoagulabil-ity are hypothesized to contribute to this phenomenon.31
Study Limitations
First, the 3-year TLF rates were lower than in other stud-ies. However, we performed periodic monitoring and data audits throughout this trial. Also, a meticulous search of all patients who were lost to follow-up was performed and thus we had a high 3-year follow-up rate, and the occur-rence of death was confirmed using a national verification system. Therefore, we believe that the possibility of event underreporting is very low. Rather, the reasons just men-tioned may better explain our findings. Another limitation was the permissive nature of the study protocol regarding angiographic follow-up and repeat revascularization, which resulted in an artificially high percentage of routine angiographic follow-up. Furthermore, this may have resulted in oculostenotic PCI rather than ischemia-driven revascularization. Therefore, there may be limitations in comparing the natural clinical course of PCI using 2 differ-ent stdiffer-ents.
Conclusions
The PtCr-EES and CoCr-ZES had similar and excellent long-term outcomes in both efficacy and safety after PCI in an all-comer East Asian population.
Acknowledgments
This study was supported by an unrestricted grant from Boston Scientific Korea. The funding source had no role in the study design, data collection, monitoring, analysis, interpretation or writing of the manuscript.
Disclosures The authors declare no conflict of interest.
References
1. Park KW, Park BE, Kang SH, Park JJ, Lee SP, Cha KS, et al. The Harmonizing Optimal Strategy for Treatment of coronary artery stenosis-sAfety & effectiveneSS of drug-elUting stents & antiplatelet REgimen (HOST-ASSURE) trial: Study protocol for a randomized controlled trial. Trials 2012; 13: 29.
2. Park KW, Kang SH, Park JJ, Yang HM, Kang HJ, Koo BK, et al. Adjunctive cilostazol versus double-dose clopidogrel after drug-eluting stent implantation: The HOST-ASSURE Random-ized Trial (Harmonizing Optimal Strategy for Treatment of Coronary Artery Stenosis–Safety & Effectiveness of Drug-Elut-ing Stents & Anti-platelet Regimen). JACC Cardiovasc Interv 2013; 6: 932 – 942.
3. Park KW, Kang SH, Kang HJ, Koo BK, Park BE, Cha KS, et al. A Randomized comparison of platinum chromium-based everolimus-eluting stents versus cobalt chromium-based zotaro-limus-eluting stents in all-comers receiving percutaneous coro-nary intervention: HOST-ASSURE (Harmonizing Optimal Strategy for Treatment of Coronary Artery Stenosis–Safety & Effectiveness of Drug-Eluting Stents & Anti-platelet Regimen), a randomized, controlled, noninferiority trial. J Am Coll Cardiol 2014; 63: 2805 – 2816.
4. Cutlip DE, Windecker S, Mehran R, Boam A, Cohen DJ, van Es GA, et al. Clinical end points in coronary stent trials. Circulation
(Efficacy of Xience/Promus Versus Cypher to Reduce Late Loss After Stenting) randomized trial. J Am Coll Cardiol 2011; 58: 1844 – 1854.
27. Kim BK, Hong MK, Shin DH, Nam CM, Kim JS, Ko YG, et al. A new strategy for discontinuation of dual antiplatelet therapy: The RESET Trial (REal Safety and Efficacy of 3-month dual antiplatelet Therapy following Endeavor zotarolimus-eluting stent implantation). J Am Coll Cardiol 2012; 60: 1340 – 1348. 28. Song L, Li J, Guan C, Jing Q, Lu S, Yang L, et al. Randomized
comparison of novel biodegradable polymer and durable poly-mer-coated cobalt-chromium sirolimus-eluting stents: Three-year outcomes of the I-LOVE-IT 2 Trial. Catheter Cardiovasc Interv 2018; 91: 608 – 616.
29. Nakamura M, Iijima R, Ako J, Shinke T, Okada H, Ito Y, et al. Dual antiplatelet therapy for 6 versus 18 months after biodegrad-able polymer drug-eluting stent implantation. JACC Cardiovasc Interv 2017; 10: 1189 – 1198.
30. Natsuaki M, Kozuma K, Morimoto T, Kadota K, Muramatsu T, Nakagawa Y, et al. Biodegradable polymer biolimus-eluting stent versus durable polymer everolimus-eluting stent: A ran-domized, controlled, noninferiority trial. J Am Coll Cardiol 2013; 62: 181 – 190.
31. Jeong YH. “East Asian paradox”: Challenge for the current antiplatelet strategy of “one-guideline-fits-all races” in acute coronary syndrome. Curr Cardiol Rep 2014; 16: 485.
Supplementary Files Please find supplementary file(s);
http://dx.doi.org/10.1253/circj.CJ-18-1303 chest pain in all-comers treated with Resolute Integrity and
Pro-mus Element stents: 2-year follow-up of the DUTCH PEERS (DUrable Polymer-Based STent CHallenge of Promus ElemEnt Versus ReSolute Integrity) randomized trial (TWENTE II). JACC Cardiovasc Interv 2015; 8: 889 – 899.
21. Meredith IT, Verheye S, Dubois CL, Dens J, Fajadet J, Carrié D, et al. Primary endpoint results of the EVOLVE trial: A ran-domized evaluation of a novel bioabsorbable polymer-coated, everolimus-eluting coronary stent. J Am Coll Cardiol 2012; 59: 1362 – 1370.
22. Dattilo PB, Prasad A, Honeycutt E, Wang TY, Messenger JC. Contemporary patterns of fractional flow reserve and intravas-cular ultrasound use among patients undergoing percutaneous coronary intervention in the United States: Insights from the National Cardiovascular Data Registry. J Am Coll Cardiol 2012; 60: 2337 – 2339.
23. Jang JS, Song YJ, Kang W, Jin HY, Seo JS, Yang TH, et al. Intravascular ultrasound-guided implantation of drug-eluting stents to improve outcome: A meta-analysis. JACC Cardiovasc Interv 2014; 7: 233 – 243.
24. Levine GN, Jeong YH, Goto S, Anderson JL, Huo Y, Mega JL, et al. Expert consensus document: World Heart Federation expert consensus statement on antiplatelet therapy in East Asian patients with ACS or undergoing PCI. Nat Rev Cardiol 2014; 11: 597.
25. Kang J, Kim HS. The evolving concept of dual antiplatelet therapy after percutaneous coronary intervention: Focus on unique feature of East Asian and “Asian paradox”. Korean Circ J 2018; 48: 537 – 551.
26. Park KW, Chae IH, Lim DS, Han KR, Yang HM, Lee HY, et al. Everolimus-eluting versus sirolimus-eluting stents in patients undergoing percutaneous coronary intervention: The EXCELLENT