저작자표시-비영리-변경금지 2.0 대한민국 이용자는 아래의 조건을 따르는 경우에 한하여 자유롭게 l 이 저작물을 복제, 배포, 전송, 전시, 공연 및 방송할 수 있습니다. 다음과 같은 조건을 따라야 합니다: l 귀하는, 이 저작물의 재이용이나 배포의 경우, 이 저작물에 적용된 이용허락조건 을 명확하게 나타내어야 합니다. l 저작권자로부터 별도의 허가를 받으면 이러한 조건들은 적용되지 않습니다. 저작권법에 따른 이용자의 권리는 위의 내용에 의하여 영향을 받지 않습니다. 이것은 이용허락규약(Legal Code)을 이해하기 쉽게 요약한 것입니다. Disclaimer 저작자표시. 귀하는 원저작자를 표시하여야 합니다. 비영리. 귀하는 이 저작물을 영리 목적으로 이용할 수 없습니다. 변경금지. 귀하는 이 저작물을 개작, 변형 또는 가공할 수 없습니다.
Radiologic,
Histologic and Functional Analysis
afterTransplantation of Autologous Cultured
Chondrocytesinto Trachea and Vocal Fold
by
Jin Seok Lee
Major in Medicine
Department of Medical Sciences
The Graduate School, Ajou University
Radiologic,
Histologic and Functional Analysis
afterTransplantation of Autologous Cultured
Chondrocytesinto Trachea and Vocal Fold
by
Jin Seok Lee
A Dissertation Submitted to The Graduate School of
Ajou University in Partial Fulfillment of the
Requirements for the Degree of Doctor of Medicine
Supervised by
Chul-Ho Kim, M.D. Ph.D.
Major in Medicine
Department of Medical sciences
The Graduate School, Ajou University
This certifies that the dissertation
ofJin Seok Lee is approved.
SUPERVISORY COMMITTEE
Keehyun Park
Yun-HoonChoung
Hyun Jun Kim
Yoon Woo Koh
Chul-Ho Kim
The Graduate School, Ajou University
June, 22nd, 2012
감사의 글
박사 학위를 시작하고 많은 시간이 지났지만 여러 은사님들의 관심과 지도로 학위를 잘 마무리 하게 되었습니다.먼저, 박사학위를 계획하고 지도해 주신 김철호 교수님께 감사드립니다. 그리고, 박사학위 지도 및 심사에 도움을 주신 박기현, 정연훈, 김현준, 고윤우 교수님께도 심심한 감사 말씀 올립니다. 학위 실험이 동물실험이었던 만큼 여러 분들에게 많은 도움을 받게 되었습니다. 이번 연구의 기본 틀을 제시해 주신 정형외과학교실의 민병헌 교수님, 항상 바쁘시지만 검체의 조직 검사를 도와주신 병리학교실의 김장희 교수님, 토끼의 CT 촬영을 허락해 주시고 도와주신 영상의학과 교수님과 기사님들, 수년간 벤치와 동물 실험실에서 고생하신 연구원 선생님들, 동물 실험 때 마다 바쁜 일정 중에서 도움을 준 전공의 선생님들께도 감사 드립니다. 그 동안 뒷바라지 하신 것도 모자라 아직도 항상 아들 걱정 하시는 부모님과 항상 옆에서 지켜봐 주며 도와주는 집사람에게 항상 죄송하고 감사한 마음 입니다. 이번 박사 학위뿐만이 아니라 지금까지 살면서 학생에서 수련의, 전공의, 전문의로의 과정을 거쳐 현재에 이르게 되었지만 주변의 도움 없이는 무엇 하나 할 수 없었을 것 입니다.무언가 한 가지 일을 마무리 지으면서 갖게 되는 기쁨과 보람보다는 주변에 감사한 마음이 더 커지게 되는 것을 보면 이제서야 철이 들고 있다는 생각이 듭니다. 앞으로 연구하고 실험할 기회가 많지는 않겠지만 이번 박사 학위를 좋은 경험으로 삼고, 은사님들 선배, 후배들과 환자들에게 도움을 주는 사람이 되도록 노력하겠습니다. 2012 년 6 월 이진석i
-ABSTRACT–
Radiologic, Histologic and Functional Analysis after Transplantation
of Autologous Cultured Chondrocytes into Trachea and Vocal Fold
Reconstruction of tracheal defects is one of the most difficult procedures in head and neck surgery. To date, various reconstructing techniques have been used with no consensus on the best approach. This study investigated the feasibility of using a fibrin/hyaluronic acid (HA) composite gel with autologous chondrocytes for tracheal reconstruction. Chondrocytes from autologous rabbit auricular cartilages were expanded and seeded into a culture dish at high density to form stable tracheal cartilages mechanically using a fibrin/HA composite gel. A 1-cm long by 0.5-cm wide defect was created by a scalpel on the cervical tracheae of six rabbits. Tissue-engineered cartilages using fibrin/HA composite were trimmed and fixed to the defect boundaries with tissuecol®. Postoperatively, the site was evaluated endoscopically, histologically, radiologically, and functionally.None of the six rabbits showed signs of respiratory distress. Postoperatively, in all cases, rigid telescopic examination showed that the implanted scaffolds were completely covered with regenerated mucosa without granulation or stenosis. Histologically, the grafts showed no signs of inflammatory reaction and were covered with ciliated epithelium. Even when grafts were broken andmigrated from their original insertion site, implanted cartilages were well preserved. However, the grafts did show signs of mechanical failure at the implantation site.The beat frequency of ciliated epithelium on implants was very similar to that of normal respiratory mucosa. In conclusions,implants with autologous chondrocytes cultured with fibrin/HA showed good tracheal luminal contour, functional epithelial regeneration, and preservation of neocartilage without inflammation, but lacked adequate mechanical stability.
Injection laryngoplasty is an option for treatment of glottic insufficiency followingvocal fold paralysis, vocal fold atrophy or scarring. We intended to evaluate theplausibility of autologous chondrocytes cultured with fibrin/hyaluronic acid (HA) forpermanent vocal fold augmentation. Chondrocytes from rabbit auricular cartilagewere expanded and cultured with fibrin/HA composite gel. 0.1 ml dosages offibrin/HA gel with autologous chondrocytes were
ii
injected into the left vocal folds ofsix rabbits. Four months postoperatively, the site was evaluated endoscopically,histologically, and radiologically. None of the six rabbits showed signs of respiratorydistress. Computed tomography images and endoscopic evaluation revealedsufficient augmentation volume of the injected vocal fold. Histologic data showed thatthe injected material did not migrate from their original insertion site. Even though thenumber of chondrocyte that settled down and survived in the injected site wasvarying in rabbits, chondrocytes successfully formed neo-cartilage at four monthspostoperatively in all cases. Histologically, the grafts showed no signs ofinflammatory reaction and were covered with ciliated epithelium. The chondrocytescultured with fibrin/HA could be a plausible injection material for vocal foldaugmentation.
Key Words: tracheal reconstruction,injection laryngoplasty, vocal cord paralysis,tissue engineering, autologous chondrocyte,
iii
TABLE OF CONTENTS
ABSTRACT ··· i
TABLE OF CONTENTS ··· iii
LIST OF FIGURES ··· iv
PART ONE ··· 1
I. INTRODUCTION ··· 1
II. MATERIALS AND METHODS ··· 3
A. Isolation of Chondrocytes ··· 3
B. Preparation of Fibrin/HA Composite Gel ··· 4
C. Animals and Surgical Procedures ··· 6
D. Endoscopic and Radiological Assessment··· 7
E. Histology and Scanning Electron Microscope (SEM) ··· 8
F. Measurement of Tracheal Ciliary Beat Frequency ··· 8
G. Statistical Analysis ··· 9
III. RESULTS ··· 10
A. Assessment of in vitro culture of autologous chondrocytes with Fibrin/HA Composite ··· 10
B. Assessment of in vivo implants using autologous chondrocytes cultured with Fibrin/HA ··· 10
IV. DISCUSSION··· 16
V. CONCLUSION ··· 19
PART TWO I. INTRODUCTION ··· 20
II. MATERIALS AND METHODS ··· 22
A. Isolation of Chondrocytes and Preparation of Fibrin/HA Composite Gel ··· 22
B. Animals and Surgical Procedures ··· 23
C. Endoscopic and Radiological Assessment ···24
D. Histologic Assessment··· 25
iv
A. Assessment of in vitro Culture of Chondrocytes with Fibrin/HA Composite Gel ···
··· 26
B. Assessment of in vivo Autologous Injection Material ··· 26
C. Histologic Assessment of Injection Material ··· 27
IV. DISCUSSION ··· 30
V. CONCLUSION ··· 33
REFERENCES ··· 34
v
-LIST OF FIGURES -
PART ONE
Fig 1. Isolation and culture of chondrocytes. ··· 4 Fig. 2. Morphological findings of tissue-engineered cartilage using a fibrin/hyaluronate
composite gel as observed at different time points. ··· 5 Fig. 3. Histology and SEM images of tissue-engineered cartilages using a fibrin/hyaluronate
composite gel as seen at 4 weeks. ··· 6
Fig. 4. Implantation of tissue-engineered cartilages using a fibrin/hyaluronate composite gel. ··· 7 Fig. 5. Findings of endoscopy of the rabbit trachea. ··· 12 Fig. 6. Findings of computed tomography of the rabbit trachea. ··· 12 Fig. 7. Histological evaluation of tissue-engineered tracheal construction 6 months after
surgery. ··· 13 Fig. 8. Scanning electron microscopic images of implanted trachea 6 months after surgery. ··· 14 Fig. 9. Measurement of trachea ciliary beat frequency (CBF). ··· 15 PART TWO
vi
Fig. 2. Endoscopic findings of the vocal folds of one representative rabbit. ···24 Fig. 3. Findings of computed tomography (CT) four months after surgery. ···26 Fig. 4. Histological evaluation of injected material four months after surgery in rabbit #1. ·
···27 Fig. 5. Histological evaluation of injected material four months after surgery in rabbit #2. ·
1
<PART ONE>
I.
INTRODUCTION
Tracheal defects, such as tracheal stricture and tracheomalacia, are related to human morbidity. Every year in the United States, approximately 150,000 patients experience complications associated with endotracheal intubation and mechanical ventilation, particularly patients with brain or spinal cord injuries requiring long-term intubation and ventilatory support.(Wijkstra et al., 2003) Chronic airway strictures show high mortality rates of 11% to 24%, and pose significant clinical challenges. Other tracheal lesions such as tumors or trauma may also require tracheal resection with primary reconstruction.(Grillo, 2002) Although the total resectable length is restricted to 30% of the trachea in children or to 6 cm in adults, replacement of longer sections will be practical with the development of reliable, functional tracheal replacements.Various approaches for tracheal replacement have been described, including the use of autologous tissues,(Cavadas, 1998)autografts,(Nakanishi et al., 1993) allografts,(Yokomise et al., 1994) prosthetic materials,(Okumura et al., 1991) or a combination of these approaches.(Osada et al., 1994) However, all of these approaches and techniques carry risks and complications, such as immune rejection, poor graft integration, graft ischemia, or rejection, resulting in limited clinical use.(Grillo, 2002)Recently, regenerative medicine has been considered as a useful clinical discipline that ensures and enhances the quality of life in patients undergoing organ reconstruction. Tissue bioengineering has already provided functional human organ replacements in various other fields.(Atala et al., 2006) However, possible impediments should be resolved to make tracheal tissue engineering successful. Factors contributing to unsatisfactory outcomes include 1) lack of ciliated epithelium, which contribute to auto-purification; 2) infection or foreign body reaction; 3) immunological complications; 4) material failure; and 5) repeated surgical interventions, including tracheostomy. The tissue engineering technique requires three fundamental components: cells, scaffolds, and growth-regulation factors. Among these components, scaffolds on which cells are proliferated and differentiated are particularly important for regeneration of structured tissues and organs. Along with the synthetic scaffolds, many naturally derived scaffolds have been developed
2
and examined, both in vitro and/or in vivo, including hyaluronate (HA),(Grigolo et al., 2001; Dausse et al., 2003) fibrin,(Stern et al., 2000) collagen,(Chaipinyo et al., 2004)alginate,(Chia et al., 2004) and chitosan scaffolds.(Suh and Matthew, 2000) Recently, a combination of two or more biomaterials is commonly used to increase the benefits of each biomaterial. In a previous study, we examined the potential of fibrin/HA gel as a promising composite biomaterial to build a hyaline-like cartilage construction(Park et al., 2005) and we demonstrated the replacement of the resected rabbit trachea with an allograft implant using a fibrin/hyaluronan composite gel.(Kim et al., 2010) One of the main limitations ofthis approach was absorption of implanted cartilages.(Kim et al., 2010)We hypothesized that autologous tissue-engineered implants have better biocompatibility and structure, supporting
in vivo cartilage formation with specialized shapes.In this preliminary studyto develop
autologous tissue-engineered circumferential tracheal segments, we performed endoscopic, radiological, and histological characterizations of autologous tissue-engineered implants for tracheal defect repair in animal experiments using auricular chondrocytes cultured with fibrin/HA. We also studied the ciliary beat frequency (CBF) of the ciliated epithelium regenerated on the implants as functional evaluation of the reconstructed airway.
3
II.
MATERIALS AND METHODS
A. Isolation of Chondrocytes
Chondrocytes were isolated from the rabbit auricular cartilages (Fig. 1-A, B). In brief, female rabbits, weighing about 3 kg ± 0.1, were anesthetized with tiletamine (4.0mg/kg; Virbac, Ltd., France) and zolazepam (4.0mg/kg; Virbac, Ltd., France) and some of the auricular cartilages were obtained from each rabbit by sterile dissection. Pieces of the cartilages were finely minced and washed with phosphate buffered saline (PBS). They were then digested in 0.2% (w/v) collagenase (Worthington Biochemical, Lakewood, NY) in PBS for 5 h at 37 °C. Using a cell strainer (70 ㎛ Nylon, Falcon, Franklin Lake, NJ), the cells were filtered, pooled, and centrifuged at 1200 rpm for 10 min. After washing twice with PBS, the cell pellet was re-suspended in Dulbecco’s modified Eagles medium (DMEM: Gibco BRL, Grand Island, NY) supplemented with 10% fetal bovine serum (FBS, Gibco BRL), 100 U/mL penicillin G (Gibco BRL), and 100 µg/mL streptomycin (Gibco BRL). The cells were then plated at a density of 1.5 x 105 cells/cm2 and placed at 37°C in a 5% CO2 incubator. The culture medium was changed every other day. The primary chondrocytes were passaged twice before starting the experiments (Fig. 1-C, D). This study was approved by the Committee for Ethics in Animal Experiments of Ajou University School of Medicine.
4
Fig. 1.Isolation and culture of chondrocytes.Autologous chondrocytes were isolated from
rabbit auricular cartilages (A, B). Pieces of cartilages were finely minced and the cells were then plated at a density of 1.5x105 cells/cm2 as a monolayer culture and placed in a 5% CO2
incubator at 37 (C)℃ . The primary chondrocyteswere passaged twice before experiments (D).
B. Preparation of Fibrin/HA Composite Gel
To prepare fibrin/HA composite gel, chondrocytes were pelleted by centrifugation and then re-suspended in a solution containing both fibrinogen (9–18 mg/mL, Mokam Research Center, Suwon, Korea) and HA (molecular size of 3000 kDa; 10 mg/mL, LGCI, Daejeon, Korea). Chondrocyte suspension of 5 x 106 cells/mL was then mixed homogeneously with aprotinin (Mokam Research Center), 60 U/mL thrombin (1000 U/mg protein: Sigma, St. Louis, MO), the fibrin stabilizing Factor XIII, and 50 mM CaCl2. Then, 250 µl of the fibrin/HA mixture was dropped into an empty Petri dish to form a gel. Each drop was then transferred to a six-well culture plate and cultured in DMEM supplemented with 10% FBS and antibiotics. Specimens were stored for up to four weeks in the medium prior to in vitro examination and implantation (Fig. 2. and Fig. 3.).
5
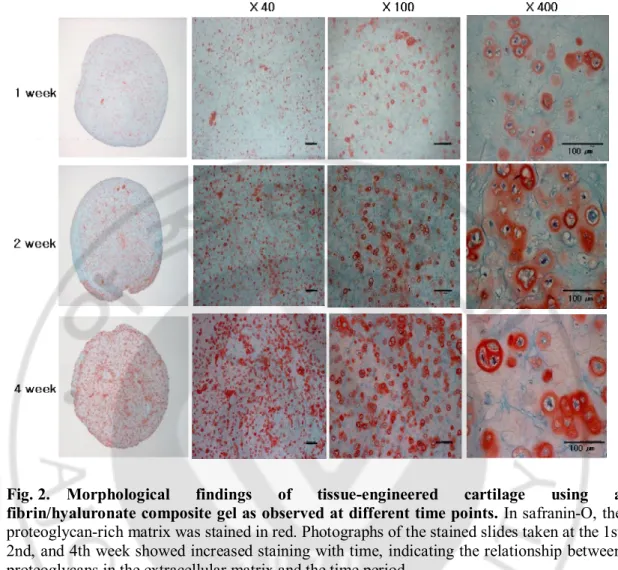
Fig. 2. Morphological findings of tissue-engineered cartilage using a fibrin/hyaluronate composite gel as observed at different time points. In safranin-O, the
proteoglycan-rich matrix was stained in red. Photographs of the stained slides taken at the 1st, 2nd, and 4th week showed increased staining with time, indicating the relationship between proteoglycans in the extracellular matrix and the time period.
6
Fig. 3. Histology and SEM images of tissue-engineered cartilages using a fibrin/hyaluronate composite gel as seen at 4 weeks.A three dimentional culture of
chondrocytes embedded in the fibrin/hyaluronate composite matrix(A). H&E staining showed that engineered tissues consisted of evenly spaced lacunae cells embedded in a basophilic matrix (bar scale: 100 μm) (B). The extracellular region was strongly stained by the characteristic red of safranin O (C). Alcian blue staining confirmed the observations of H&E staining (D). SEM images of implants reflected the surface characteristics of the fibrin/hyaluronate composite with chondrocytes (E, F).
C. Animals and Surgical Procedures
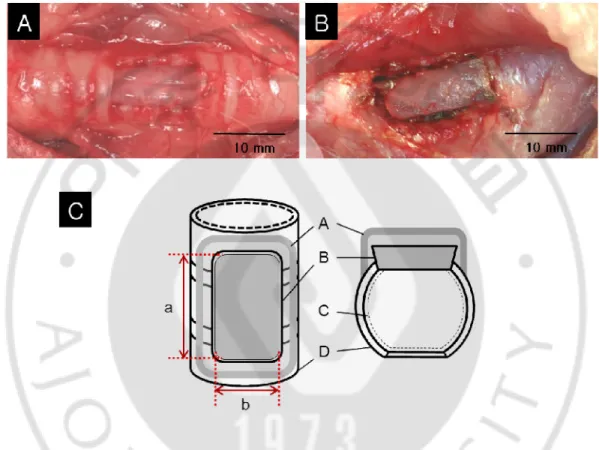
Under anesthesia by tiletamine (4.0mg/kg; Virbac, Ltd., France) and zolazepam (4.0mg/kg; Virbac, Ltd., France), the cervical trachea was exposed through a vertical skin incision and splitting of the sternohyoid and sternothyroid muscles along the median line. Tracheal defects, approximately 5 mm wide by 10 mm long, were made using a scalpel (Fig. 4-A). The autologous cartilage with a fibrin/HA scaffold was trimmed and inserted into the resected site (Fig. 4-B, C). Finally, it was fixed and sealed to the defected boundaries with tissuecol® (fibrinogen 110mg+ thrombin 500IU+ aprotinin 3000KIU, DaLim Co., Seoul, Korea). Both sides of the split sternohyoid and sternothyroid muscles were then replaced over the graft and sutured. Finally, the incised skin was sutured.Animal care, housing, and experimental procedures were conducted according to the Guidelines for Animal Experiments of Ajou University. Tardomyocel ® comp (Benzathine penicillin G (100,000IU),
7
Procaine penicillin G (25,000IU), and streptomycin (125.000IU); Bayer, Ltd., Korea) were administered (0.1ml/kg; subcutaneous injection) for 5 days to prevent postoperative infections.
Fig. 4. Implantation of tissue-engineered cartilages using a fibrin/hyaluronate composite gel. Under anesthesia, the cervical tracheae were exposed through a vertical skin
incision and splitting of the sternohyoid and sternothyroid muscles along the median line. Tracheal defects, approximately 5 mm wide by 10 mm long, were formed by a scalpel (A). An allograft cartilage with a fibrin/HA scaffold was trimmed and inserted edge to edge to the resected site instead of overlaying. It was fixed and sealed to the defected boundaries with tissuecol® (B). A schematic of the technique described in this study (C). A: tissuecol, B:
implant, C: mucosa, D: cartilage, a: length of implant, b: width of implant.
D. Endoscopic and Radiological Assessment
To monitor the progress of tracheal regeneration, endoscopic examinations were carried out periodically with an endoscopy systemconsisting of a rigid endoscope (0 degree,
8
diameter 4mm, Karl Storz, Tuttlingen, Germany) and a camera (Coolpix 3500, Nikon Co., Tokyo, Japan) with a light source (Head-light unit, Head-light, Karl Storz, Tuttlingen, Germany). Anesthesia was induced with tiletamine (4.0mg/kg; Virbac, Ltd., France) and zolazepam (4.0mg/kg; Virbac, Ltd., France) to facilitate these examinations. A three dimensional image of the rabbit’s trachea was obtained using computed tomography (CT) performed on the operation site using a CT scanner system (Brilliance 64, Philips, Eindhoven, Netherlands) 1, 3, and 6 months postoperatively.
E. Histology and Scanning Electron Microscope (SEM)
Histological assessments including light microscopy and scanning electron microscopy were also performed to evaluate the regenerative status of the operated site at three and six months postoperatively. After fixing with 10% formalin for 24 h, the implanted samples were embedded in paraffin and sectioned at 5 ㎛ thickness. The sections were stained with hematoxylin and eosin (H&E) for cell morphology. Both safranin O/fast green and alcian blue were used to locate the glycosaminoglycan (GAG) deposits in the specimens. The surface morphology of the implant was examined using a scanning electron microscope (Hitachi S-800, Tokyo, Japan). Before SEM observation, the samples were fixed with 0.4% glutaraldehyde for 24 hours and then coated with gold/palladium for 20 min.
F. Measurement of Tracheal Ciliary Beat Frequency
Tracheal ring explants (1-2 mm thick) were prepared from the trachea, and the trachea was washed with DMEM/F12 medium (DMEM/F12: Dulbecco’s Modified Eagle’s Medium/ Ham’s F-12; Gibco, Gand Island, NY) containing 10000 Units/㎖ penicillin- 10000 ㎍/㎖ streptomycin (Gibco, Gand Island, NY) and kept in the medium. Briefly, actively beating ciliated cells were maintained at 24 ± 0.5°C by a thermostatically controlled heated stage and were digitally analyzed using an inverted microscope (Axiovert 40CLF, Carl Zeiss, Inc., Thornwood, NY) and a high speed digital camera (Moticam 2000, Motic Ltd., Causeway Bay, Hong Kong). Whole-field analysis was performed using a software (Ammons Engineering, Mt. Morris, MI) that automatically analyzed the entire captured image of all ciliated cells in a given field. Amplitudes and frequencies of all cilia were collated, mapped
9
to the screen image, and statistically analyzed to determine the average frequency and standard deviation (SD) of ciliary beat on the entire image. Predominant frequencies of all motile cilia were sampled in at least six separate fields. Thus, all frequencies were expressed as mean ± SD from six separate fields.
G. Statistical analysis
Parameters of the data from at least six independent experiments were expressed as mean ± SD. Comparisons of the means of different groups were made using one-way analysis of variance (ANOVA). Statistical significance was set at P < 0.05.
10
III.
RESULTS
A. Assessment of in vitro culture of autologous chondrocytes with fibrin/HAcomposite
As shown in Fig. 2, chondrocytes kept their round shape and preserved their attachment on the fibrin/HA matrix. Among the whole cell population in vitro, more than 90% were viable cells in the fibrin/HA composite at week 1. The cells were homogeneously distributed in the matrix and exhibited round morphology along lacunae. The extracellular region was strongly stained in safranin O (red), indicating the presence of the proteoglycan-rich matrix (Fig. 2). At week 4, the accumulated GAG at the core region of the fibrin/HA composite in vitro was more significant than that at week 1.At 4 weeks, histological features of the tracheal implant H&E staining revealed a nearly normal hyaline cartilage (Fig. 3-A, B). Similar to that of a native trachea, the staining showed the presence of a mature cartilage surrounded by connective tissues. With safranin O staining, the tissue-engineered cartilage was organized into lobules with round, angular lacunae, each containing a single chondrocyte (Fig. 3-C). In addition, alcian blue showed intense staining of the entire matrix at 4 weeks, confirming the abovementioned observations (Fig. 3-D).In SEM, a large amount of the extracellular matrix produced by the engineered cartilage was observed. The HA fibers were found embedded in and distributed through the entire matrix (Fig. 3-E, F). In most areas, morphology and structure of the engineered cartilage were similar to those of the native cartilage.
B. Assessment of in vivo implants using autologous chondrocytes cultured with Fibrin/HA
In total, six rabbits underwent the process of tracheal reconstruction with tissue-engineered cartilages. During recovery or postoperative period, none of the rabbits showed any signs of stridor or difficulty in breathing. All animals survived through the operation and no wound infection or signs of inflammation at the surgical sites were noted.Telescopic findings under anesthesia showed that all six rabbits resulted in complete recovery with no
11
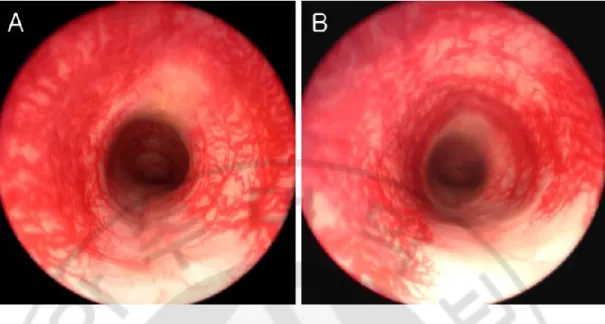
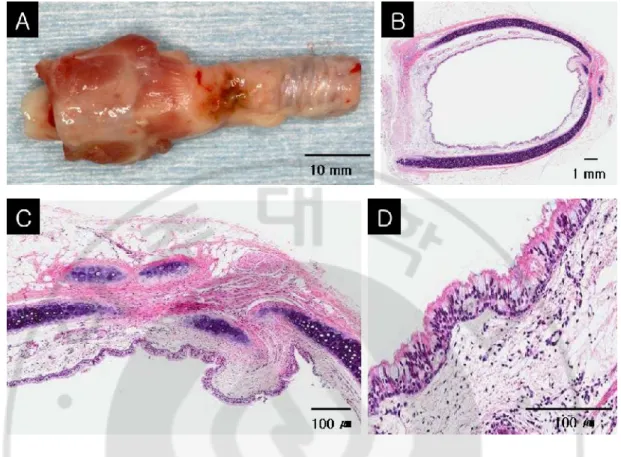
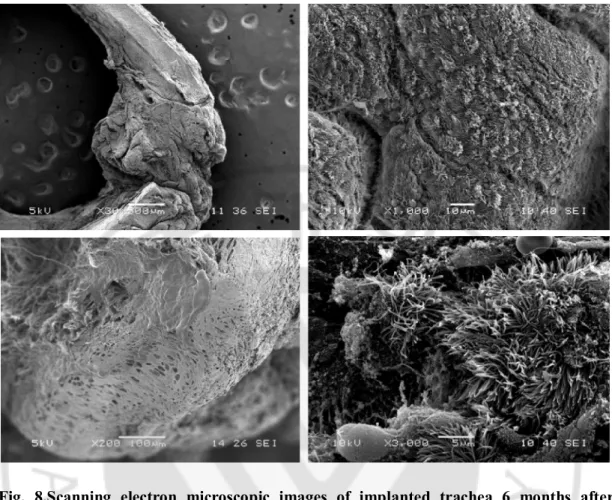
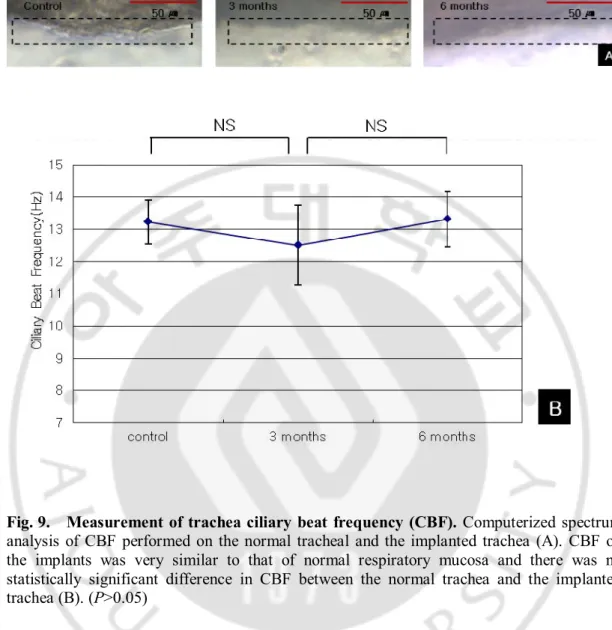
stenosis or granulation in the regenerated trachea (Fig. 5A, B). Figure 5 shows the telescopic images of the rabbits with typical luminal portrayal of their successfully reconstructed trachea 1 month and 6 months after the operation.No obvious tracheal stenosis was observed on the CT images at two different observational periods. Six months after surgery, axial CT images at the operated sites revealed a fine luminal portrayal of the reconstructed trachea (Fig. 6-A) and definite cartilage signal was detected in the three-dimensional images reconstructed from fine axial images (Fig. 6-B).Gross assessments showed that all implants appeared to be healthy and integrated, and the luminal shape was comparable in size with that of a native rabbit trachea (Fig. 7-A, B). However, all grafts underwent partial breaking and migration from their original insertion site into the tracheal defect (Fig. 7-B, C). Histological assessments indicated that the cartilages closely resembled native tracheal cartilages with similar overall morphology (Fig. 7-C, D). H&E staining revealed the presence of mature chondrocytes and matrix surrounded by connective tissues as expected in native trachea. Three months after surgery, the epithelial lining was already complete at the operated site and the concentration of cilia was nearly normal (Fig. 7-C, D).SEM images showed completely regenerated cilia on the external surface and lacunae cells, matrix, and fibrous tissues on the cross sectional view (Fig. 8).When normal tracheal mucosa was compared to the regenerated mucosa, the CBF of the regenerated ciliated epithelium was similar to the normal control data with no statistically significant difference of CBF between a normal trachea and a implanted trachea (Fig. 9-A, B). (P = 0.239 by one-way ANOVA: control versus implanted trachea at postoperative 3 months: P = 0.169; control versus implanted trachea at postoperative 6 months: P = 0.868; postoperative 3 months (of implanted trachea) versus postoperative 6 months: P = 0.127).
12
Fig. 5.Findings of endoscopy of the rabbit trachea. The implant was a good fit on the
tracheal defect in the rabbit. In images taken 1 month (A) and 6 months (B) after the operation, the implant was completely covered with regenerated mucosa without any granulation or displacement.
Fig. 6. Findings of computed tomography of the rabbit trachea. Six months after
surgery, axial CT images at the operated sites revealed a fine luminal portrayal of the reconstructed trachea (A) and cartilage signal was clearly detected in the three-dimensional images reconstructed from fine axial images (B).
13
Fig. 7.Histological evaluation of tissue-engineered tracheal construction 6 months after surgery.Gross specimen of the implanted trachea (A).Hematoxylin-eosin staining shows
viable engineered cartilage within the reconstructed larynogotrachea along with partial inflammatory cells in submucosa (B). However, due to the compressive force of the laryngotracheal complex, all grafts underwent partial buckling, breaking, and migration from their original insertion site into the laryngofissure. The luminal surface layered with connective tissues is completely covered with epithelial cells and pseudostratified ciliated columnar epithelium (i.e. normal respiratory mucosa) is clearly observed (C, D).
14
Fig. 8.Scanning electron microscopic images of implanted trachea 6 months after surgery.Gross images of the implanted trachea and the adjacent normal trachea (A). The
cross-section image of lacunae cells and fibrous tissues (B) and the scanning electron microscopic images shows completely regenerated cilia on the external surface (C, D).
15
Fig. 9. Measurement of trachea ciliary beat frequency (CBF). Computerized spectrum
analysis of CBF performed on the normal tracheal and the implanted trachea (A). CBF on the implants was very similar to that of normal respiratory mucosa and there was no statistically significant difference in CBF between the normal trachea and the implanted trachea (B). (P>0.05)
16
IV.
DISCUSSION
A variety of materials have been used in tracheal prostheses, such as various inert materials alone(Neville, 1982; Okumura et al., 1991) or in combination with autologous tissues,(Osada et al., 1994; Banis et al., 1996) but none of them has been effective. There is, however, a general agreement that autologous tissues are the first choice in reconstructive surgery, particularly in tracheal surgery. Several reports have described experimental tracheal reconstruction with autotransplants, but none of them has proven to be satisfactory for human use. However, this procedure is complicated by the need for a long-term immunosuppressant therapy and a lack of sufficient donor tissue. Therefore, reconstruction of cartilage tissues used by tissue engineering these days has become one of the most popular and prospective research themes due to the fact that chondrocytes rely on the permeation of tissue fluid for nutrition supply, thus exempting cartilage tissues from revascularization. Due to their low antigenic characteristics, allogeneic chondrocytes can be used to repair cartilage tissue defects.(Langer and Vacanti, 1993; Weinand et al., 2006)In our previous allogeneic study, we were unable to find any evidence of graft rejection or severe inflammation.(Park et al., 2005; Kim et al., 2010) However, the limitation of our previous study was graft resorption.(Kim et al., 2010) Therefore, methods to decrease the absorption of implanted cartilages should be developed. In this study, we hypothesized that autologous tissue-engineered implants have better biocompatibility and structure supporting in vivo cartilage formation. Compared with our previous study, the use of autologous tissue-engineered cartilage implants for reconstruction of the trachea can be advantageous over the allogeneic approach in terms of preservation of implanted cartilages. However, our preliminary study has some limitations in terms of reconstruction of partial tracheal resection because small defects in which at least 50% of the native cartilagenous support for the trachea is preserved can be allowed to heal by second intention with little eventual loss of lumen and successful reepithelization. Therefore, this study was designed as a preliminary animal experiment for evaluation of tissue-engineered implants using a fibrin/HA composite gel and an intermediate step toward the ability to produce lengths of autologous tissue-engineered complete tracheal segments. Based on our previous study,(Park et al., 2005; Kim et al.,
17
2010)we used fibrin glue mixed with HA as a composite scaffold. Fibrin glue possesses several important features: (i) biocompatibility and biodegradability, (ii) fibronectin-rich, and (iii) high affinity for biological tissues. Fibronectin is an essential protein in the cartilage matrix for chondrocytes–extracellular matrix (ECM) interaction; however, the weak mechanical properties and early degradation of fibrin have been problematic.(Peretti et al., 2001) HA is considered as a key component in the cartilage ECM with high hydrophilicity and molecular weight. HA binds to aggrecan, an assembly of large aggregating proteoglycans, and to the chondrocyte surface receptor CD 44. It is believed that mutual interactions between chondrocytes, ECM molecules, and HA are critical in maintaining cartilage homeostasis.(Ishida et al., 1997) In our present work, the fibrin/HA composite provided a favorable environment for chondrocytes to maintain their characteristic phenotype and synthesize cartilage ECMs.In the present study, a rabbit model was designed to determine the suitability of using autologous engineered cartilages as grafts in tracheal reconstruction. The meaningful results from this study were that tissue-engineered cartilages in tracheal defects of all rabbits were preserved, although the tracheal regeneration were incomplete, and that functional epithelial regeneration was observed. It was also noted that in each rabbit, the airway was maintained even in cases where the grafts had shifted position or collapsed. The fact that the grafts were broken and occasionally become dislodged from their original insertion point demonstrates that the compressive biomechanical forces exerted on the grafts were not always counteracted by the mechanical properties of the grafts themselves and that surgical placement is extremely important for graft success. What is unclear is the cause of the displacement of some of the grafts. In some cases, the graft material itself appears to have collapsed, but in other instances, the graft material may have simply shifted its position during or soon after surgical implantation.In tracheal regeneration, functional epithelial regeneration is very important. Belsey summarized the requirements for tracheal replacement: a laterally rigid, but longitudinally flexible tube and a surface covered with ciliated respiratory epithelium.(Belsey, 1950) At the very beginning, many scientists were led to believe in the illusionary simplicity of tissue-engineered tracheal reconstruction and took it as no more than developing a tubular cartilage tissue. Later, animal examinations demonstrated the importance of an intact epithelial line to prevent the in-growth of granulomatous tissues and fatal airway obstruction. The cilia also help to expel the mucosal
18
fluid and the adhering microparticles. Therefore, the focus in tissue-engineered trachea studies has shifted currently towards substitution of reepithelialization.(Kamil et al., 2004; Kim et al., 2004)From this perspective, we ascertained the importance of functional assessment of cilia and measured the CBF of implanted mucosa. Comparable to our previous study, the CBF of the regenerated ciliated epithelium was similar to the control data with no statistically significant difference in CBF between a normal trachea and an implanted trachea (P > .05). However, to mention superiority of our approach (autologous chondrocytes cultured with fibrin/HA) in terms of functional reepithelialization, it needs to evaluate in long circumferential tracheal defect because most cases of tracheal reconstruction or secondary healing after partial resection demonstrated successful reepithelialization.
19
V.
CONCLUSION
This preliminary study shows that tracheal reconstruction after partial resection using implants with autologous chondrocytes cultured with fibrin/HA resulted in favorable epithelialization on the implants and preservation of neo-cartilage without graft rejection or inflammation, but lacked adequate mechanical stability. Further studies on the mechanical stability of cultured autologous cartilage implantation and the ability to produce autologous tissue-engineered circumferential tracheal segments are essential to advance our technique as a good substitute for conventional approaches.
20
<PART TWO>
I.
INTRODUCTION
Glottic insufficiency, which is caused by vocal fold paralysis, bowing, atrophy orscarring, occasionally leads to severe dysphonia and aspiration, eventually make thepatients encounter socio-economic disability.(Hillel et al., 1999) Unilateral vocal fold paralysis is mostcommonly caused by iatrogenic unilateral recurrent laryngeal or vagus nerve injuryduring several kinds of surgery such as head and neck surgery includingthyroidectomy, esophageal surgery, thoracic surgery, or skull base surgery.(Dimarakis and Protopapas, 2004; Myssiorek, 2004) Sulcusvocalis or vocal atrophy, which are common vocal fold findings of presbylaryngis, arereported to be observed in up to 25% of elderly people.(Takano et al., 2010; Davids et al., 2012) Surgical treatment forglottal insufficiency can be classified into two types according to the approachSurgical procedures which need an external approach like type I thyroplasty,arytenoid adduction or laryngeal re-innervation could be one option1 and injectionlaryngoplasty which uses autologous fat(Shindo et al., 1996; Havas and Priestley, 2003), collagen(Pearl et al., 2002), polymethylmethacrylate(PMMA)(Homicz and Watson, 2004) or calcium hydroxylapatite(Chhetri et al., 2004) could be another. These days, injectionlaryngoplasty, which is a relatively simple procedure that can be performed in theout-patient department and does not need an external incision, is the most frequentlyused option. However, injectable bio materials are not often permanent, and multipleinjections may be required. An external incision might be needed to harvest theinjectable autologous materials, while synthetic materials may trigger inflammatoryimmune reactions.(Kwon and Buckmire, 2004) Furthermore, the injection materials that are currently beingused have shown limited improvement in patients with sulcus vocalis or vocal foldatrophy.(Welham et al., 2011) Therefore, investigations for the development of the ideal permanentinjection material need to be continued.Meanwhile, autologous chondrocyte implantation (ACI) is now accepted as aneffective treatment for chondral defects in orthopedics.(Harris et al., 2010) Because chondrocytesmainly receive their nutrition by diffusion of substances and can endure a low oxygenenvironment, implanted chondrocytes easily survive in human bodies. Onceimplanted, chondrocytes are able to express their normal phenotype andsuccessfully
21
perform their original function, providing biomechanical properties bysynthesizing extracellular matrix (ECM) components. These ECM components mightbe able to maintain the augmented volume for treatment of glottal insufficiency.Therefore, strategy of using autologous chondrocyte might possibly be abiocompatible and durable new candidate for injection laryngoplasty.The fibrin/hyaluronic acid (HA) composite are known to provide a favorableenvironment for chondrocytes to maintain their characteristic phenotype andsynthesize cartilage extracellular matrix (ECM).(Ishida et al., 1997; Allison and Grande-Allen, 2006) We previously reported thesuccessful reconstruction of tracheal defect using fibrin/HA composite gel.(Kim et al., 2010) Thesecomplexes showed good biocompatibility without graft rejection or severeinflammation. With this precedent study, we hypothesized that these chondrocytescultured with fibrin/HA could be a plausible injection material for vocal foldaugmentation. In this study, we performed endoscopic, radiologic, and histologiccharacterizations in animal experiments using autologous chondrocytes cultured withfibrin/HA.
22
II.
MATERIALS AND METHODS
A. Isolation of Chondrocytes and Preparation of Fibrin/HA Composite Gel
Chondrocytes were isolated from rabbit auricular cartilage. Under anesthesia bytiletamine (4.0 mg/kg) (Virbac Ltd., Carros, France) and zolazepam (4.0 mg/kg)(Virbac), the auricular cartilage (Fig. 1A) was removed by sterile dissection. Pieces ofcartilage were finely minced and washed with phosphate buffered saline (PBS). Theywere then digested in 0.2% (w/v) collagenase (Worthington Biochemical, Lakewood,NY, USA) in PBS for 5 hours at 37°C. Using a 70 Km nylon cell strainer (Falcon,Franklin Lake, NJ, USA), the cells were filtered, pooled, and centrifuged at 1200 rpmfor 10 minutes. After washing twice with PBS, the cell pellet was resuspended inDulbecco’s modified Eagles medium (DMEM) (Gibco BRL, Grand Island, NY, USA)supplemented with 10% fetal bovine serum (FBS) (Gibco BRL), 100 U/mL penicillinG (Gibco BRL) and 100 μg/mL streptomycin (Gibco BRL). The cells were then platedat a density of 1.5 X105 cells/cm2 and placed at 37°C in a 5% CO2 incubator (Fig.1B). The culture medium was changed every other day. The primary chondrocyteswere passaged twice before the experiments.To prepare the fibrin/HA composite gel, the chondrocytes were pelleted bycentrifugation, and then resuspended in a solution containing both fibrinogen (9– 18mg/mL) (Mokam Research Center, Suwon, South Korea) and HA (molecular size of3,000 kDa; 10 mg/mL) (LGCI, Daejeon, South Korea). Chondrocyte suspension of 5X 106
cells/mL was then mixed homogeneously with 110KIU/ml aprotinin (MokamResearch Center), 60 U/mL thrombin (1,000 U/mg protein) (Sigma, St. Louis, MO,USA), 50U fibrin stabilizing factor XIII, and 50mM CaCl2 (Fig. 1C).
23
Fig.1. Isolation and culture of chondrocytes. (ACartilage tissue was harvested from rabbit
auricular cartilage and finely minced. (B)The cells were then plated at a density of 1.5 X105
cells/cm2 as a monolayerculture. (C) The chondrocytes were pelleted by centrifugation, and
then resuspendedin a solution containing both fibrinogen and hyaluronic acid. (D) The chondrocytesretained their shape and mixed with the fibrin/HA gel and homogeneously distributedin the fibrin/HA composite.
B. Animals and Surgical Procedure
Animal care, housing, and experimental procedures were conducted according to theGuidelines for Animal Experiments of Ajou University. Under anesthesia, 0.1 mldosages of fibrin/HA gel with autologous chondrocytes were injected with a 25-gaugeneedle into the left vocal folds of six New Zealand white rabbits under a 4-mmpediatric laryngoscope (8575AV, Karl Storz, Tuttlingen, Germany) (Fig. 2).Tardomyocel® compound (benzathine penicillin G [100,000 IU], procaine penicillin G[25,000 IU], streptomycin [125,000 IU])
24
(Bayer Korea Ltd., Seoul, South Korea) wasadministered (0.1 ml/kg; subcutaneous injection) for 5 days to prevent postoperativeinfections.
Fig.2. Endoscopic findings of the vocal folds of one representative rabbit. (A) Successful
augmentation of vocal fold with injected material immediate after the injection (black arrowheads). (B) Four months after the injection, augmentation (black arrowheads) was still sustained in the same rabbit.
C. Endoscopic and Radiologic Assessment
Endoscopic examinations to monitor the progress of regenerative status were carriedout four months postoperatively with an endoscopy system consisting of a rigidendoscope (diameter 4 mm) (Karl Storz, Tuttlingen, Germany) and a camera(Coolpix 3500; Nikon Co., Tokyo, Japan) with a light source (Head Light; Karl Storz).Anesthesia was inducted with tiletamine (4.0 mg/kg) and zolazepam (4.0 mg/kg) tofacilitate these examinations. Four months postoperatively, computed tomography(CT) performed on the larynx using a CT scanner system (Brilliance 64; Philips,Eindhoven, The Netherlands).
25
D. Histologic Assessment
Four months after the injection laryngoplasty was performed, the animals weresacrificed. Their larynges were resected and prepared for light microscopicexaminations. After fixing with 10% formalin for 24 hours, the implanted sampleswere embedded in paraffin and sectioned in 5 Km thickness. Glottic horizontalsections with a thickness of 5 Km were taken and the sections were mounted onglass slides. Samples were examined under the light microscope after being stainedwith hematoxylin–eosin (H&E) and safranin-O (S-O).
26
III.
RESULTS
A. Assessment of in vivo Cultureof Chondrocytes with Fibrin/HA Composite gel
Figure 1D shows that the chondrocytes retained their shape and mixed with thefibrin/HA gel. The viable cells counted for more than 90% of the whole cell populationin the fibrin/HA composite at day 5 in vitro (Fig. 1D). The cells were homogeneouslydistributed in the fibrin/HA composite.
B. Assessment of in vivo Autologous Injection Material
The postoperative condition of all rabbits was good. None of them showed any signsof infection and respiratory distress. Telescopic findings under anesthesiaimmediately after the injection showed that augmentation of the vocal fold with theinjected material was successful (Fig. 2A). Four months after the injection,augmentation was still sustained (Fig. 2B). Four months post-injection axial CT scanrevealed sufficient bulging of the injected vocal fold (Fig. 3).
27
Fig.3. Findings of computed tomography (CT) four months after surgery. (A), (B) Axial
CT images of the operated sites of two different rabbits reveal sufficient bulging of the injected vocal fold (black arrowheads).
C. Histologic Assessments of Injection Material
Post-injection 4 months histologic assessments revealed correct placement of theinjected materials within the paraglottic space of the larynx (Fig. 4, 5). On H&Estaining, the injected material formed tissue distinguishable from normal surroundingtissue (Fig. 4, red circles). The newly-formed tissue was not accompanied by anyinflammatory reaction such as infiltration of macrophages and integrated well withthe surrounding tissue (Fig. 4A-d, black arrowheads). Seen under high magnification(X100 or X400), the injected autologous chondrocytes were uniformly distributed inthe newly-formed area (Fig. 4A-e, black arrows).On S-O staining, the formation and accumulation of ECM components, proteoglycan,was identified under low magnification. Under higher magnification,
28
chondrocyteslocated in their lacunae were observed (Fig. 4B-2, black stars). ECM was formed inboth the interterritorial matrix adjacent to the lacunae and territorial matrix betweenthe lacunae.In another rabbit (Fig. 5), more cells than rabbit of the figure 4 resided in the newlyformed area and small amount of ECM formation was identified with S-O staining.However, lacunae formation was not detected.There was no evidence of tissue reaction or inflammatory response in all rabbits.
Fig.4. Histological evaluation of injected material four months after surgery in rabbit #1. (A) Hematoxylin and eosin staining. The injected material formed different tissue
distinguished from normal surrounding tissue (red circle). The newly-formed tissue did not accompany any inflammatory reaction such as infiltration of macrophage and integrated well with surrounding tissue (black arrowheads). The injected cells (black arrows) were uniformly distributed in the newly formed area. (B) Safranin-O staining. The formation and accumulation of ECM component proteoglycan was identified in low-magnification field. In high-magnification field, chondrocytes located in their lacunae were observed (black stars).
29
Fig.5. Histological evaluation of injected material four months after surgery in rabbit #2. (A) Hematoxylin and eosin staining. More cells than rabbit #1 resided in the newly
formed area (red circle). (B) Safranin-O staining. Small amount of extracellular matrix formation was identified. However, lacunae formation was not detected.
30
IV.
DISCUSSION
Various materials have been developed and used for injection laryngoplasty to treatdeficiencies in glottal closure. However, no material has satisfied all areas until now.The ideal material for injection laryngoplasty would be biocompatible, durable, andeasily applied, resulting in a permanent medialization of the paralyzed vocal fold.Among currently used material, autologous material such as fat or fascia hasstrength in biocompatibility, but it is difficult to predict the remaining volume afterresorption and a large incision on the donor site is needed.(Havas and Priestley, 2003)Gelfoam or collagenfrom cadavers is known not to provoke any immune response, but is completelyresorbed and disappears in 4 – 6 weeks and thus only used for temporaryaugmentation of the vocal fold.8 PMMA and calcium hydroxylapatite, which arewidely used synthetic materials, have shown successful permanent glottisaugmentation. However, a biocompatibility problem still remains to be solved asseveral investigators have reported that foreign body granulomas may form afterinjection of these synthetic materials.(McClelland et al., 1997; Rudolph et al., 1999)In developing a biocompatible and permanent injection material for vocal foldaugmentation, we focused on autologous chondrocyte. We previously appliedautologous chondrocytes on the reconstruction of tracheal defects using a fibrin/HAcomposite gel.(Kim et al., 2010) Implanted chondrocytes are known to easily settle down in humanbodies and to be able to synthesize ECM components. The synthesized ECMcomponents exist and maintain the volume, even after the implanted chondrocytesdisappear. Therefore, we intend to investigate the plausibility of autologouschondrocytes cultured with fibrin/HA as an injection material for vocal foldaugmentation.In this study, the implanted material successfully maintained the shape of theaugmented vocal fold four months after the injection. The injected autologouschondrocytes successfully settled down and were uniformly distributed in the newlyformedarea. The implants and newly-formed tissue did not result in anyinflammatory reaction and integrated well with the surrounding tissue. Because, thevolume was mainly composed of proteoglycan, which was synthesized by theinjected chondrocytes, the augmentation might last a long period of time. However,the number of surviving chondrocytes in the newly formed area was varying inrabbits. One of the possible explanations is as follows. In rabbits with few survivingchondrocytes, injected chondrocytes
31
synthesized and accumulated ECMs in earlyperiods, after which the chondrocytes disappeared and cells from surroundingtissues immigrated into preformed, well-organized scaffolds, eventually maintainingthe augmented volume. The fact that cells in newly formed tissue resembled withcells in surrounding area supports this hypothesis.There have been several investigations about injecting autologous or allogeniccartilage harvested from the ear and minced into tiny chips.(Lee et al., 2004; Lee et al., 2011) According to thesestudies, injected auricular cartilage maintained its location and volume over 24months. However, these methods generally require a larger volume of cartilage,which eventually results in donor site morbidity. In addition, minced cartilage needs alarger injection needle than the present study, which could possibly be a limitation forfuture clinical application.The purpose of a scaffold is to act as a template to promote cellular interactions andsynthesis of the ECM which provides the structural framework for the newly formedtissue. It is important that the scaffold, a temporary structure, mimics the physiologicconditions of the ECM because this affects the differentiation potential of the cellsbeing seeded.(Chen et al., 2010) In this study, based on our previous study, we used fibrin glue,mixed with HA, as a composite scaffold. Fibrin glue, which is known to bebiocompatible, biodegradable and fibronectin rich, is one of the popular scaffold intissue engineering. It also has a high affinity to biological tissue. Fibronectin is anessential protein in the cartilage matrix for chondrocyte–ECM interaction.(Peretti et al., 2001) Inaddition, HA has been widely used as a scaffold for tissue engineering because of itsexcellent biocompatibility, viscoelastic properties, and ease of chain sizemanipulation. It also facilitates ECM remodeling via its interaction with cell surfacereceptors including CD44, which promotes the migration of cells.(Ishida et al., 1997; Allison and Grande-Allen, 2006) In the presentwork, the fibrin/HA composite provided a favorable environment for chondrocytes tomaintain their characteristic phenotype and to synthesize cartilage ECMs.Furthermore, research into the role of HA in laryngology indicates that it hasprofound effects on the structure and viscosity of vocal folds. In particular, it isresponsible for giving the vocal folds some of the viscoelasticity that is important inphonation and beneficial for the healing process.(Ward et al., 2002)Fibronectin also plays an pivotalrole in the phenotype of both normal vocal folds and in vocal fold disease.(Hirschi et al., 2002)Therefore, a fibrin/HA composite gel might be an appropriate scaffold for injectionlaryngoplasty,In terms of clinical application, there might also exist the difficulty in
32
obtaining anadequate number of chondrocytes, considering the slow rate of chondrocyteproliferation, and donor site morbidity.(Bentley et al., 2003; Hui et al., 2012) However, in a clinical setting, the usualvolume needed for the injection laryngoplasty is only 0.5 – 1.5 ml including thescaffold.(Kwon and Buckmire, 2004) This amount of chondrocytes is easily obtainable by the current culturesystem. A small amount of cartilage could be obtained from tragal cartilage withoutsignificant morbidity, and the procedure is very familiar to otolaryngologists becausethe tragal cartilage is frequently harvested for use in tympanoplasties orrhinoplasties.One of the challenges with using cell/scaffold-based therapies is to control accuracyand reproducibility. The augmented volume should be accurately predictable.Furthermore, the vocal fold is not merely a space occupying organ, but a complexorgan where the structure functionally generates the voice. Therefore, viscoelasticity,which is a key property of the vocal fold involving phonation, should be verified afteraugmentation. This preliminary study has some limitations. One of the weak points isthe absence of a control group, such as cartilage injection only or chondrocyte onlygroup. The relatively short follow-up period is also a weakness for evaluating thepermanent efficacy of the injection material. Although preliminary studies have beenpromising, the effectiveness of autologous chondrocyte injection using a fibrin/HAcomposite gel in the treatment of glottal insufficiency requires further long-termstudies.
33
V.
CONCLUSION
This study shows that injection laryngoplasty using composite gel with autologous chondrocytes cultured with fibrin/HA resulted in sufficient augmentation volume of the injected vocal cord and formation of neo-cartilage from 4 months postoperatively. The chondrocytes cultured with fibrin/HA might be could be a plausible injection material for vocal cord augmentation.
34
- REFERENCES –
1. Allison DD, Grande-Allen KJ: Review. Hyaluronan: a powerful tissue engineering tool. Tissue Eng 12: 2131-2140, 2006
2. Atala A, Bauer SB, Soker S, Yoo JJ, Retik AB: Tissue-engineered autologous bladders for patients needing cystoplasty. Lancet 367: 1241-1246, 2006
3. Banis JC, Jr., Churukian K, Kim M, Gu JM, Anderson GL, Kaneko S, Keelen T, Barker JH: Prefabricated jejunal free-tissue transfer for tracheal reconstruction: an experimental study. Plast Reconstr Surg 98: 1046-1051, 1996
4. Belsey R: Resection and reconstruction of the intrathoracic trachea. Br J Surg 38: 200-205, 1950
5. Bentley G, Biant LC, Carrington RW, Akmal M, Goldberg A, Williams AM, Skinner JA, Pringle J: A prospective, randomised comparison of autologous chondrocyte implantation versus mosaicplasty for osteochondral defects in the knee. J Bone Joint
Surg Br 85: 223-230, 2003
6. Cavadas PC: Tracheal reconstruction using a free jejunal flap with cartilage skeleton: experimental study. Plast Reconstr Surg 101: 937-942, 1998
7. Chaipinyo K, Oakes BW, Van Damme MP: The use of debrided human articular cartilage for autologous chondrocyte implantation: maintenance of chondrocyte differentiation and proliferation in type I collagen gels. J Orthop Res 22: 446-455, 2004
8. Chen W, Tabata Y, Tong YW: Fabricating tissue engineering scaffolds for simultaneous cell growth and drug delivery. Curr Pharm Des 16: 2388-2394, 2010 9. Chhetri DK, Jahan-Parwar B, Hart SD, Bhuta SM, Berke GS: Injection
laryngoplasty with calcium hydroxylapatite gel implant in an in vivo canine model.
Ann Otol Rhinol Laryngol 113: 259-264, 2004
10. Chia SH, Schumacher BL, Klein TJ, Thonar EJ, Masuda K, Sah RL, Watson D: Tissue-engineered human nasal septal cartilage using the alginate-recovered-chondrocyte method. Laryngoscope 114: 38-45, 2004
11. Dausse Y, Grossin L, Miralles G, Pelletier S, Mainard D, Hubert P, Baptiste D, Gillet P, Dellacherie E, Netter P, Payan E: Cartilage repair using new polysaccharidic
35
biomaterials: macroscopic, histological and biochemical approaches in a rat model of cartilage defect. Osteoarthritis Cartilage 11: 16-28, 2003
12. Davids T, Klein AM, Johns MM, 3rd: Current dysphonia trends in patients over the age of 65: is vocal atrophy becoming more prevalent? Laryngoscope 122: 332-335, 2012
13. Dimarakis I, Protopapas AD: Vocal cord palsy as a complication of adult cardiac surgery: surgical correlations and analysis. Eur J Cardiothorac Surg 26: 773-775, 2004
14. Grigolo B, Roseti L, Fiorini M, Fini M, Giavaresi G, Aldini NN, Giardino R, Facchini A: Transplantation of chondrocytes seeded on a hyaluronan derivative (hyaff-11) into cartilage defects in rabbits. Biomaterials 22: 2417-2424, 2001
15. Grillo HC: Tracheal replacement: a critical review. Ann Thorac Surg 73: 1995-2004, 2002
16. Harris JD, Siston RA, Pan X, Flanigan DC: Autologous chondrocyte implantation: a systematic review. J Bone Joint Surg Am 92: 2220-2233, 2010
17. Havas TE, Priestley KJ: Autologous fat injection laryngoplasty for unilateral vocal fold paralysis. ANZ J Surg 73: 938-943, 2003
18. Hillel AD, Benninger M, Blitzer A, Crumley R, Flint P, Kashima HK, Sanders I, Schaefer S: Evaluation and management of bilateral vocal cord immobility.
Otolaryngol Head Neck Surg 121: 760-765, 1999
19. Hirschi SD, Gray SD, Thibeault SL: Fibronectin: an interesting vocal fold protein. J
Voice 16: 310-316, 2002
20. Homicz MR, Watson D: Review of injectable materials for soft tissue augmentation.
Facial Plast Surg 20: 21-29, 2004
21. Hui JH, Buhary KS, Chowdhary A: Implantation of orthobiologic, biodegradable scaffolds in osteochondral repair. Orthop Clin North Am 43: 255-261, 2012
22. Ishida O, Tanaka Y, Morimoto I, Takigawa M, Eto S: Chondrocytes are regulated by cellular adhesion through CD44 and hyaluronic acid pathway. J Bone Miner Res 12: 1657-1663, 1997
23. Kamil SH, Eavey RD, Vacanti MP, Vacanti CA, Hartnick CJ: Tissue-engineered cartilage as a graft source for laryngotracheal reconstruction: a pig model. Arch
36
Otolaryngol Head Neck Surg 130: 1048-1051, 2004
24. Kim DY, Pyun J, Choi JW, Kim JH, Lee JS, Shin HA, Kim HJ, Lee HN, Min BH, Cha HE, Kim CH: Tissue-engineered allograft tracheal cartilage using fibrin/hyaluronan composite gel and its in vivo implantation. Laryngoscope 120: 30-38, 2010
25. Kim J, Suh SW, Shin JY, Kim JH, Choi YS, Kim H: Replacement of a tracheal defect with a tissue-engineered prosthesis: early results from animal experiments. J
Thorac Cardiovasc Surg 128: 124-129, 2004
26. Kwon TK, Buckmire R: Injection laryngoplasty for management of unilateral vocal fold paralysis. Curr Opin Otolaryngol Head Neck Surg 12: 538-542, 2004
27. Langer R, Vacanti JP: Tissue engineering. Science 260: 920-926, 1993
28. Lee BJ, Wang SG, Goh EK, Chon KM, Lee CH: Intracordal injection of autologous auricular cartilage in the paralyzed canine vocal fold. Otolaryngol Head Neck Surg 131: 34-43, 2004
29. Lee JC, Lee BJ, Wang SG, Lee CH, Shin DH: Intracordal Injections with Allogenic Cartilage in a Canine Paralyzed Vocal Fold Model: Long-Term Results. J Voice, 2011
30. McClelland M, Egbert B, Hanko V, Berg RA, DeLustro F: Evaluation of artecoll polymethylmethacrylate implant for soft-tissue augmentation: biocompatibility and chemical characterization. Plast Reconstr Surg 100: 1466-1474, 1997
31. Myssiorek D: Recurrent laryngeal nerve paralysis: anatomy and etiology.
Otolaryngol Clin North Am 37: 25-44, v, 2004
32. Nakanishi R, Shirakusa T, Mitsudomi T: Maximum length of tracheal autografts in dogs. J Thorac Cardiovasc Surg 106: 1081-1087, 1993
33. Neville WE: Reconstruction of the trachea and stem bronchi with Neville prosthesis.
Int Surg 67: 229-234, 1982
34. Okumura N, Nakamura T, Shimizu Y, Natsume T, Ikada Y: Experimental study of a new tracheal prosthesis made from collagen-grafted mesh. ASAIO Trans 37: M317-319, 1991
35. Osada H, Takeuchi S, Kojima K, Yamate N: The first step of experimental study on hybrid trachea: use of cultured fibroblasts with artificial matrix. J Cardiovasc Surg
37
(Torino) 35: 165-168, 1994
36. Park SH, Park SR, Chung SI, Pai KS, Min BH: Tissue-engineered cartilage using fibrin/hyaluronan composite gel and its in vivo implantation. Artif Organs 29: 838-845, 2005
37. Pearl AW, Woo P, Ostrowski R, Mojica J, Mandell DL, Costantino P: A preliminary report on micronized AlloDerm injection laryngoplasty. Laryngoscope 112: 990-996, 2002
38. Peretti GM, Randolph MA, Zaporojan V, Bonassar LJ, Xu JW, Fellers JC, Yaremchuk MJ: A biomechanical analysis of an engineered cell-scaffold implant for cartilage repair. Ann Plast Surg 46: 533-537, 2001
39. Rudolph CM, Soyer HP, Schuller-Petrovic S, Kerl H: Foreign body granulomas due to injectable aesthetic microimplants. Am J Surg Pathol 23: 113-117, 1999
40. Shindo ML, Zaretsky LS, Rice DH: Autologous fat injection for unilateral vocal fold paralysis. Ann Otol Rhinol Laryngol 105: 602-606, 1996
41. Stern S, Lindenhayn K, Schultz O, Perka C: Cultivation of porcine cells from the nucleus pulposus in a fibrin/hyaluronic acid matrix. Acta Orthop Scand 71: 496-502, 2000
42. Suh JK, Matthew HW: Application of chitosan-based polysaccharide biomaterials in cartilage tissue engineering: a review. Biomaterials 21: 2589-2598, 2000
43. Takano S, Kimura M, Nito T, Imagawa H, Sakakibara K, Tayama N: Clinical analysis of presbylarynx--vocal fold atrophy in elderly individuals. Auris Nasus
Larynx 37: 461-464, 2010
44. Ward PD, Thibeault SL, Gray SD: Hyaluronic acid: its role in voice. J Voice 16: 303-309, 2002
45. Weinand C, Peretti GM, Adams SB, Jr., Randolph MA, Savvidis E, Gill TJ: Healing potential of transplanted allogeneic chondrocytes of three different sources in lesions of the avascular zone of the meniscus: a pilot study. Arch Orthop Trauma Surg 126: 599-605, 2006
46. Welham NV, Choi SH, Dailey SH, Ford CN, Jiang JJ, Bless DM: Prospective multi-arm evaluation of surgical treatments for vocal fold scar and pathologic sulcus vocalis. Laryngoscope 121: 1252-1260, 2011
38
47. Wijkstra PJ, Avendano MA, Goldstein RS: Inpatient chronic assisted ventilatory care: a 15-year experience. Chest 124: 850-856, 2003
48. Yokomise H, Inui K, Wada H, Goh T, Yagi K, Hitomi S, Takahashi M: High-dose irradiation prevents rejection of canine tracheal allografts. J Thorac Cardiovasc Surg 107: 1391-1397, 1994
39 - 국문요약 -
자가 연골세포 배양물의 성대 및 기관 주입후
주입물의 유지와 조직학적 변화 및 기능적 변화 분석
아주대학교 대학원 의학과 이 진 석 (지도교수: 김철호) 기관 손상 재건은 두경부외과 영역에 있어서 가장 어려운 분야의 술기 중 하나로 알려져 있다. 최근까지도 여러 재건 방법들에 대한 연구가 진행되고 있으나 아직까지는 표준적으로 사용되는 방법이 정해지지 않고 있다. 성대주입술은성대마비, 성대구증등다양한질환으로인한애성및흡인을치료하는데갑상성형술과더불어중요한 술식으로알려져있다. 최근에는성대주입술이갑상성형술에비해비교적간단하고환자의부담을덜어줄수있는 술식으로널리시행되고있는실정이다. 그러나이러한기관재건물및성대주입물의경우에재건및주입후지속시간이짧아서추가 주입이필요하거나, 면역반응에인한염증으로합병증이발생할수있어새로운기관재건물이나성대주입물에 관한연구가지속되고있다.본 연구는 토끼에서 fibrin/hyaluronic acid(HA)합성겔을 이용하여 자가연골세포를 배양하고 이를 기관재건물 및 성대 주입물로사용하여 그 유용성을 알아보고자 하였다.여섯 마리의 토끼의 이개 연골에서 채취한 연골세포를 fibrin/HA 합성겔을 이용하여 배양 후 각각의 토끼의 기관에 인위적으로 만든 1.0cm x 0.5cm 손상부위에 삽입하였다. 삽입40 후 기관내시경, 조직학적 검사 및 전자현미경, 전산화 단층촬영, 섬모운동주파수 측정등을 이용하여 삽입물과삽입물을 덮고 있는 상피세포를 평가하였다. 같은 방법으로 제작한 성대주입물을토끼의성대주름에주입하고 4 개월후후두내시경및전산화단층촬영, 조직학적검사를시행하였다.기관내시경과 전산화 단층촬영상 삽입물 부위에 육아종 형성이나 기관협착 소견 없이 점막으로 덮인 소견이 관찰되었고, 수술 후 호흡곤란 소견을 보이는 토끼는 없었으며, 조직학적 검사 및 전자현미경상에는 염증반응 없이 섬모점막상피가 형성되어 있는 소견이 관찰되었다. 새로 형성된 섬모점막상피의 섬모 운동의 정도를 측정한 결과 기존 기관의 섬모 운동과 비슷한 정도의 섬모 운동이 관찰되었다. 성대 주입물의 경우 후두내시경및전산화단층촬영상주입한성대측에충분한부피의증대가관찰되었고, 주입 4 개월후시행한조직학적검사에서새로운연골세포의생성이관찰되었다.결론적으로 자가연골세포와 fibrin/HA 를 이용한 기관재건 삽입물은기관내경의 유지, 기능적인 섬모상피세포의 재생, 염증 반응 없는 새로운 연골세포의 유지 측면에서 유용할 것으로 판단된다. 또한 성대주입물은주입물의흡수및염증반응없이성대부피증대가가능한효과적인주입물의 특성을지니고있는것으로조사되었다.