이용자는 아래의 조건을 따르는 경우에 한하여 자유롭게 l 이 저작물을 복제, 배포, 전송, 전시, 공연 및 방송할 수 있습니다. 다음과 같은 조건을 따라야 합니다: l 귀하는, 이 저작물의 재이용이나 배포의 경우, 이 저작물에 적용된 이용허락조건 을 명확하게 나타내어야 합니다. l 저작권자로부터 별도의 허가를 받으면 이러한 조건들은 적용되지 않습니다. 저작권법에 따른 이용자의 권리는 위의 내용에 의하여 영향을 받지 않습니다. 이것은 이용허락규약(Legal Code)을 이해하기 쉽게 요약한 것입니다. Disclaimer 저작자표시. 귀하는 원저작자를 표시하여야 합니다. 비영리. 귀하는 이 저작물을 영리 목적으로 이용할 수 없습니다. 변경금지. 귀하는 이 저작물을 개작, 변형 또는 가공할 수 없습니다.
Doctoral Thesis in Medicine
Relation between preoperative
electromyographic activity of the deltoid
and trapezius and clinical results after
reverse shoulder arthroplasty
by
LI HONGRI
Ajou University Graduate School
Major in Medicine
Relation between preoperative
electromyographic activity of the deltoid
and trapezius and clinical results after
reverse shoulder arthroplasty
Doohyung Lee,
M.D., Ph.D.
Advisor
I submit this thesis as the
Doctoral thesis in Medicine
February 2020
Ajou University Graduate School
Major in Medicine
Department of Medical Sciences
LI HONGRI
The Doctoral thesis of LI HONGRI in Medicine
is hereby approved.
Thesis Defense Committee President
11111111111111111111
Seung-hyun Yoon
Member1111111wook hwan kim
Bong-gun Lee
Member1S ng uk han
Jae-Ho Cho
Member111111111111111111111
Nam-Su Chung
Member111111111111111111111
Doohyung Lee
Ajou University Graduate School
December 23, 2019
i
ABSTRACT
Background: If patients susceptible to poor clinical outcomes could be predicted
before reverse shoulder arthroplasty (RSA), it would help to set reasonable post-surgical patient expectations in the preoperative setting. Our hypothesis is that the preoperative electromyographic (EMG) activity of the deltoid and upper trapezius muscles is correlated with clinical outcomes of patients undergoing RSA.
Methods: EMG activity in the deltoid and upper trapezius muscles was measured in
25 patients scheduled to undergo RSA during three motions: shrugging, forward flexion, and abduction. Their postoperative clinical results were assessed prospectively during regular outpatient visits, including strength, active range of motion, pain, and functional scores. The correlations between the preoperative EMG activities and clinical results were analyzed.
Results: Postoperative shoulder strength after RSA was increased in patients with
greater preoperative EMG activity in the middle deltoid and upper trapezius. Preoperative EMG activity of the anterior or middle deltoid muscle was associated with active ROM of flexion or abduction, while EMG activity of the posterior deltoid was associated with the active ROM of external rotation.
Conclusions: Shoulder strength after RSA was positively correlated with
preoperative EMG activity in the deltoid and upper trapezius. Active ROM after RSA was positively correlated with preoperative EMG activity in the deltoid. Therefore, preoperative EMG measurements of the deltoid and upper trapezius may predict clinical outcomes after RSA.
Level of evidence: Level II, prognosis study
Keyword: electromyography, trapezius, deltoid, muscle strength, reverse shoulder
ii
LIST OF CONTENTS
ABSTRACT ... i
LIST OF CONTENTS ... ii
LIST OF FIGURES ... iii
LIST OF TABLES ... iv
I. INTRODUCTION ... 1
II. MATERIALS AND METHODS ... 4
III. RESULTS ... 12
IV. DISCUSSIONS ... 18
V. CONCLUSIONS ... 22
iii
LIST OF FIGURES
Figure 1. Photographs showing the bipolar surface electrodes placement for four muscles (1: anterior deltoid, 2: middle deltoid, 3: posterior deltoid, 4: upper trapezius). A BTS FREEEMG 300 system (gray cuboidal shape) used to collect EMG signals was connected with the paired surface electrodes. ... 9 Figure 2. Three motions and reference posture for EMG measurement. A. Standing
without shoulder motion as reference posture B. Shrugging, C. Active flexion D. Active abduction. ... 10
iv
LIST OF TABLES
Table 1. Placement of electrodes for deltoid and upper trapezius ... 8 Table 2. Clinical data before surgery and at final follow up ... 14 Table 3. Preoperative EMG amplitudes (%RVC) of deltoid and upper trapezius
muscles during three motions such as shrugging, abduction and forward flexion ... 15 Table 4. Correlation between preoperative EMG amplitude during three motions and
postoperative clinical results such as shoulder strength (in abduction), active range of motion and functional scores. ... 16
1
2
Reverse shoulder arthroplasty (RSA) is an effective treatment for cuff tear arthropathy (CTA) or severely degenerative osteoarthritis (OA) with large cuff tears in elderly patients.19 Although RSA has good outcomes, particularly in reducing pain,
shoulder strength after RSA is often unpredictable. After RSA, some patients complain of insufficient improvement in strength, which may result from complex muscular problems of joint function in flexion and rotation and the high variability of anatomical modifications with glenoid bone loss and atrophy of the associated muscles.7,21 Based on the mechanics of massive tears and the compensatory role of the deltoid, patients show cranial migration of the humeral head and secondary degenerative OA. 27,28 Biomechanically, RSA increases the moment arm by medializing the center of rotation, thereby increasing the strength of the deltoid muscle.2,22 Excessive tension or degeneration of the deltoid can cause shoulder
weakness after RSA.12,32 Moreover, excessive tension can sometimes result in complications such as stress fractures of the acromium.3 Therefore, deltoid muscle function is an important factor in patients with RSA.30,31 It is thought that the stronger
the deltoid is, the better the prognosis after RSA. The upper trapezius muscle is activated in abduction and external rotation of the scapula for healthy individuals.5,6,9,17 The upper trapezius shows increased electromyographic (EMG)
activity during abduction in patients with rotator cuff tears.13 Therefore, this study
examined whether the preoperative activity of the deltoid or upper trapezius muscles is correlated with shoulder strength or range of motion (ROM) after RSA.
A conventional method of evaluating the activity of the deltoid or upper trapezius muscle is to use manual muscle tests or a handheld device. However, in patients with CTA, it is difficult to evaluate the strength of the deltoid and upper trapezius muscles independently of the effects of the injured rotator cuff.4,10,25,33
Magnetic resonance imaging (MRI) and Computed Tomography (CT) can be used to evaluate the condition of the deltoid muscle but has limited ability to evaluate
3
dynamic muscle motion.12,18,35 Therefore, we used dynamic EMG measurements to
evaluate the activity of the deltoid and upper trapezius muscles. We hypothesized that patients with greater EMG activity in the deltoid or upper trapezius preoperatively would have greater shoulder strength or active ROM after RSA.
4
5
This was a prospective study. All experimental procedures were approved by the Institutional Review Board. Informed consent was obtained from all patients. From November 2015 to October 2017, we recruited 32 patients scheduled to undergo RSA after no response to conservative treatment for at least 6 months. Patients were included if they consented to dynamic EMG measurement of the shoulder muscles before surgery and underwent primary RSA with a diagnosis of CTA or severe degenerative OA with a large rotator cuff tear using a reverse type prosthesis (Exactech, Gainesville, FL, USA). The exclusion criteria were any neurological deficit, such as axillary nerve palsy, cervical radiculopathy, or myelopathy; previous infection around the shoulder; a systemic disorder such as diabetes mellitus, rheumatoid arthritis, or thyroid dysfunction; and revision arthroplasty. Ultimately, 21 patients with CTA and 4 patients with OA with large rotator cuff tears were included. There were 20 women (80%). The mean age of the participants was 73 ± 6 years, their mean height was 153.8 ± 12.1 cm, and their mean weight was 55.6 ± 8.4 kg. The average follow-up period was 14 ± 3 months.
A single surgeon performed all RSAs. The glenohumeral joint was approached through the deltopectoral plane. The glenoid component was fixed with superior inclination of 10° and 0° retroversion and the humeral stem was fixed with 20° retroversion.24 All surgeries were done without repairing the subscapularis, while the
infraspinatus tear was repaired when possible.
All patients underwent the following tests before and after surgery as outpatients. Patients were asked to rate the intensity of their worst pain on a visual analogue scale from 0 (none) to 10 (maximal).15 Active ROM was measured using a
goniometer with a long arm, including forward flexion, abduction, and external rotation. Active internal rotation was measured as the highest spine level that the patient could reach. Strength was measured at 90° of abduction using a handheld di
6
gital dynamometer (JTECH Commander, UT, USA). However, in patients with active forward flexion ROM < 90° due to pseudoparalysis (n =13), muscle strength was measured at the maximum abduction angle. The Constant score and American Shoulder and Elbow Surgeons (ASES) Standardized Shoulder Assessment Form were used for functional evaluations.1,16
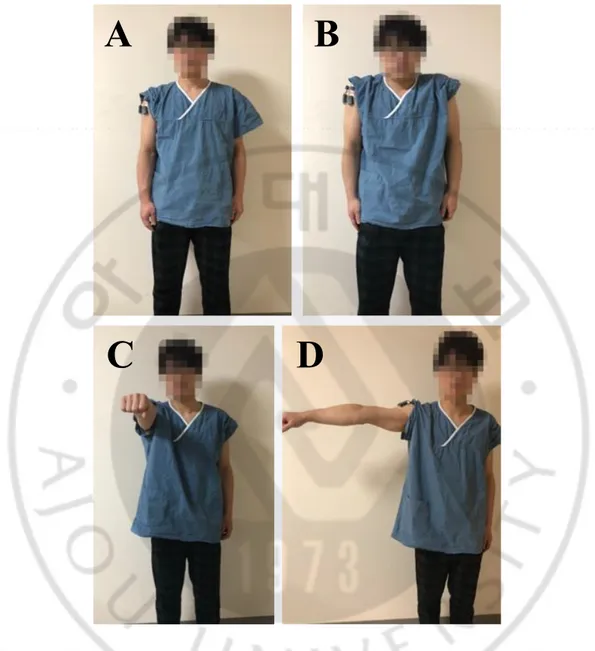
The day before surgery, dynamic EMG measurements of the deltoid and upper trapezius muscles were made during three motions: shrugging, forward flexion, and abduction. First, anodic surface electrodes were attached at a specific area for each muscle: the anterior, middle, and posterior deltoid and upper trapezius (Table 1). A disposable, self-adhesive, pre-gelled bipolar Ag/AgCl electrode was used with an interelectrode distance of 20 mm. Before attaching the electrodes, the skin covering the muscles was cleaned with alcohol to minimize impedance. EMG signals from the four muscles were collected using a BTS FREE EMG 300 system (BTS Bioengineering, MA, USA) (Fig. 1). Before EMG measurements, the three motions to be performed were explained. After each motion, the patient was allowed to recover for at least 2 min to avoid local muscle fatigue (Fig. 2). Shrugging was performed for 10 s and it was a relatively painless motion that was tolerated by the patients with CTA or severe OA. To measure the EMG signals during shoulder flexion, the arm was raised to 90° of forward flexion for 10 s. When it was difficult to maintain the arm at 90° of abduction due to pseudoparalysis (n=13), the patients were tested at the maximum degree of forward flexion that they could achieve. Finally, to measure the EMG signals during shoulder abduction, the arm was abduct ed to 90° for 10 s. If it was difficult to maintain the arm at 90° of abduction, the measurement was performed in the same manner as the measurement of shoulder flexion. To reduce interference during the initiation or termination of each motion, the EMG signal for 3–6 s was analyzed. The signal was amplified with a gain of 500, noise < 1 μV, and a common mode rejection ratio of 100. The EMG signals were
7
sampled at 1500 Hz and filtered at a bandwidth of 10,500 Hz. All signals were collected by a laptop computer equipped with a 16-bit analog-to-digital converter. The EMG signals acquired for each motion were converted by full-wave rectification and filtered through a second-order Butterworth filter with a cutoff frequency of 3 Hz.14,34 Although maximal voluntary contraction (MVC) is the most common
method for normalizing EMG amplitudes, we used the controlled reference voluntary contraction (RVC) method because of the massive rotator cuff tears. As a reference posture, the EMG amplitude was measured for 10 s while standing with both arms at the sides.26 %RVC was calculated as the normalized EMG amplitude
8
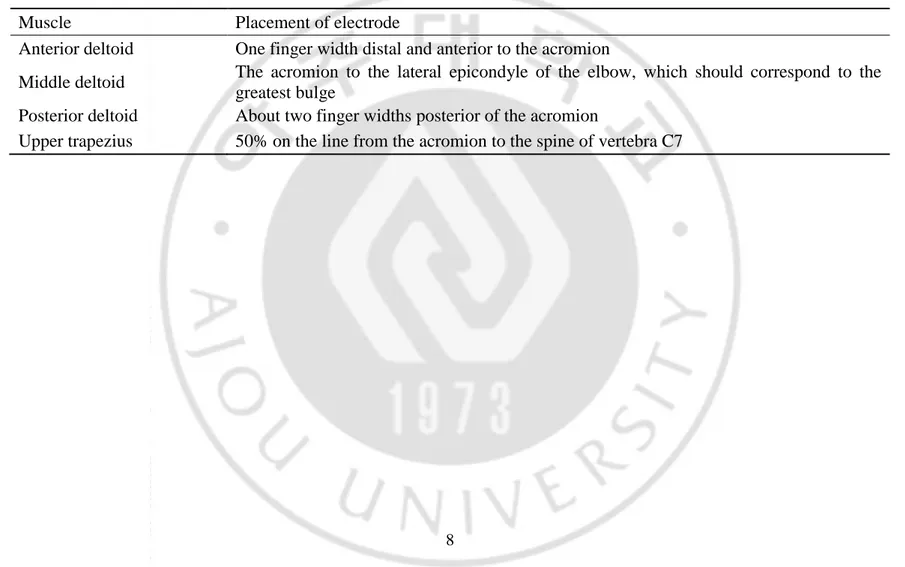
Table 1. Placement of electrodes for deltoid and upper trapezius Muscle Placement of electrode
Anterior deltoid One finger width distal and anterior to the acromion
Middle deltoid The acromion to the lateral epicondyle of the elbow, which should correspond to the greatest bulge
Posterior deltoid About two finger widths posterior of the acromion
9
Figure 1. Photographs showing the bipolar surface electrodes placement for four muscles (1: anterior deltoid, 2: middle deltoid, 3: posterior deltoid, 4: upper trapezius). A BTS FREEEMG 300 system (gray cuboidal shape) used to collect EMG signals was connected with the paired surface electrodes.
10
A
B
C
D
Figure 2. Three motions and reference posture for EMG measurement. A. Standing without shoulder motion as reference posture B. Shrugging, C. Active flexion D. Active abduction.
11
For statistical analyses, partial correlations with confounding variables such as age and sex were used to evaluate the associations between preoperative EMG amplitudes of the deltoid and upper trapezius muscles and postoperative shoulder strength and active ROM; the results are presented as correlation coefficients (R). Clinical data were compared between the preoperative assessment and final follow-up using the Wilcoxon signed-rank test. A P-value < 0.05 was considered to indicate statistical significance. Statistical analyses were performed using SPSS ver. 12.0.1 (SPSS, Chicago, IL, USA).
12
13
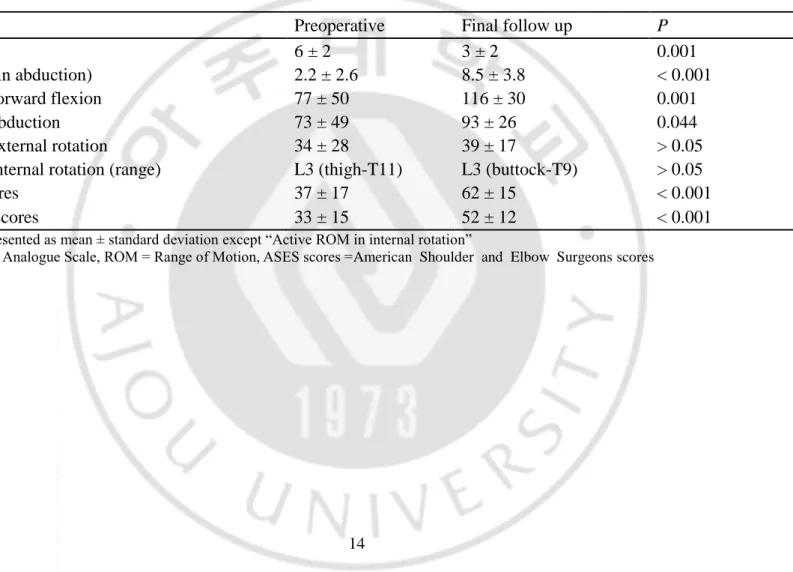
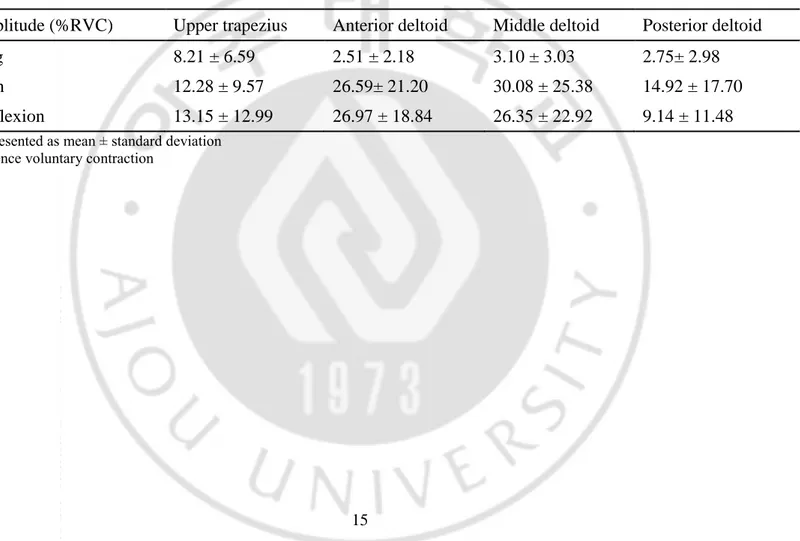
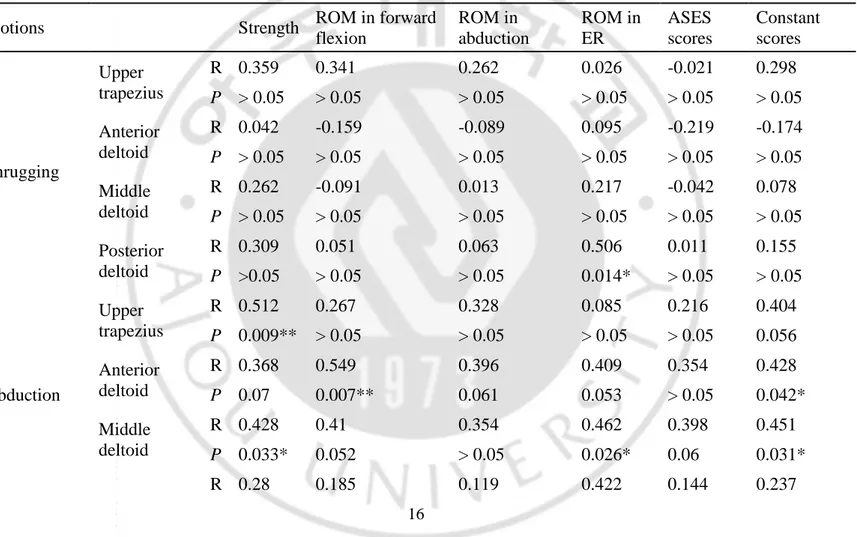
Table 2 compares the pre- and postoperative clinical findings. While VAS, strength, active ROM of forward flexion and abduction, ASES scores, and Constant scores were improved, active ROM in external and internal rotation did not. In terms of EMG amplitudes, preoperatively, shrugging motion activated mainly the upper trapezius at 8% RVC, while shoulder abduction and forward flexion activated the upper trapezius at 12–13% RVC and the deltoid except the posterior fibers at 26–30% RVC (Table 3). For the upper trapezius, the preoperative EMG amplitudes during abduction were positively correlated with shoulder strength (R = 0.512, P = 0.009) at the final follow-up. For the anterior deltoid, the preoperative EMG amplitudes during abduction were positively correlated with the active ROM in forward flexion (R = 0.549, P = 0.007) and Constant scores (R = 0.428, P = 0.042) at the final follow-up. The preoperative EMG amplitudes during forward flexion were positively correlated with the active ROM in forward flexion (R = 0.588, P = 0.003) and abduction (R = 0.461, P = 0.027) at the final follow-up. For the middle deltoid, the preoperative EMG amplitudes during abduction were positively correlated with shoulder strength (R = 0.428, P = 0.033) and active ROM in external rotation (R = 0.462, P = 0.026) and Constant scores (R = 0.451, P = 0.031) at the final follow-up. The preoperative EMG amplitudes during forward flexion were positively correlated with the active ROM in forward flexion (R = 0.446, P = 0.033) at the final follow-up. For the posterior deltoid, the preoperative EMG amplitudes during shrugging were positively correlated with the active ROM in external rotation (R = 0.506, P = 0.014) (Table 4). The preoperative shoulder strength during abduction was not correlated with shoulder strength or active ROM (both P > 0.05) at the final follow-up.
14
Table 2. Clinical data before surgery and at final follow up
Preoperative Final follow up P
VAS 6 ± 2 3 ± 2 0.001
Strength (in abduction) 2.2 ± 2.6 8.5 ± 3.8 < 0.001 ROM in forward flexion 77 ± 50 116 ± 30 0.001 ROM in abduction 73 ± 49 93 ± 26 0.044 ROM in external rotation 34 ± 28 39 ± 17 > 0.05 ROM in internal rotation (range) L3 (thigh-T11) L3 (buttock-T9) > 0.05 ASES scores 37 ± 17 62 ± 15 < 0.001 Constant scores 33 ± 15 52 ± 12 < 0.001
Values are presented as mean ± standard deviation except “Active ROM in internal rotation”
15
Table 3. Preoperative EMG amplitudes (%RVC) of deltoid and upper trapezius muscles during three motions such as shrugging, abduction and forward flexion
EMG amplitude (%RVC) Upper trapezius Anterior deltoid Middle deltoid Posterior deltoid Shrugging 8.21 ± 6.59 2.51 ± 2.18 3.10 ± 3.03 2.75± 2.98 Abduction 12.28 ± 9.57 26.59± 21.20 30.08 ± 25.38 14.92 ± 17.70 Forward flexion 13.15 ± 12.99 26.97 ± 18.84 26.35 ± 22.92 9.14 ± 11.48
Values are presented as mean ± standard deviation RVC = reference voluntary contraction
16
Table 4. Correlation between preoperative EMG amplitude during three motions and postoperative clinical results such as shoulder strength (in abduction), active range of motion and functional scores.
Motions Strength ROM in forward flexion ROM in abduction ROM in ER ASES scores Constant scores Shrugging Upper trapezius R 0.359 0.341 0.262 0.026 -0.021 0.298 P > 0.05 > 0.05 > 0.05 > 0.05 > 0.05 > 0.05 Anterior deltoid R 0.042 -0.159 -0.089 0.095 -0.219 -0.174 P > 0.05 > 0.05 > 0.05 > 0.05 > 0.05 > 0.05 Middle deltoid R 0.262 -0.091 0.013 0.217 -0.042 0.078 P > 0.05 > 0.05 > 0.05 > 0.05 > 0.05 > 0.05 Posterior deltoid R 0.309 0.051 0.063 0.506 0.011 0.155 P >0.05 > 0.05 > 0.05 0.014* > 0.05 > 0.05 Abduction Upper trapezius R 0.512 0.267 0.328 0.085 0.216 0.404 P 0.009** > 0.05 > 0.05 > 0.05 > 0.05 0.056 Anterior deltoid R 0.368 0.549 0.396 0.409 0.354 0.428 P 0.07 0.007** 0.061 0.053 > 0.05 0.042* Middle deltoid R 0.428 0.41 0.354 0.462 0.398 0.451 P 0.033* 0.052 > 0.05 0.026* 0.06 0.031* R 0.28 0.185 0.119 0.422 0.144 0.237
17 Posterior deltoid P > 0.05 > 0.05 > 0.05 0.045* > 0.05 > 0.05 Forward flexion Upper trapezius R 0.311 0.16 0.214 -0.042 0.077 0.239 P > 0.05 > 0.05 > 0.05 > 0.05 > 0.05 > 0.05 Anterior deltoid R 0.33 0.588 0.461 0.243 0.347 0.402 P > 0.05 0.003** 0.027* > 0.05 > 0.05 0.057 Middle deltoid R 0.321 0.446 0.408 0.25 0.352 0.397 P > 0.05 0.033* 0.053 > 0.05 > 0.05 0.06 Posterior deltoid R 0.191 0.226 0.077 0.146 0.168 0.186 P > 0.05 > 0.05 > 0.05 > 0.05 > 0.05 > 0.05
EMG = electromyography, ROM = range of motion, ER = external rotation, ASES scores = American shoulder elbow society scores, R = correlation coefficient, ** P < 0.01, * P < 0.05
18
19
Higher EMG activity of the deltoid or upper trapezius muscles preoperatively predicted the recovery abduction force and active ROM in forward flexion, abduction, and external rotation. This is the first investigation of the preoperative factors related to the prognosis of RSA using dynamic EMG measurements.
Although RSA alters shoulder kinematics, the deltoid is the major muscle for forward flexion and abduction of the shoulder.3 A few studies have evaluated the
function of the deltoid using MRI or computed tomography and have found that the deltoid is related to postoperative outcomes after RSA. The greater the fatty degeneration in the deltoid seen on MRI, the lower the Constant scores.12 In a
previous study, the volume of a three-dimensional deltoid muscle model created from MRI using image-processing software was related to the prognosis of RSA.35
However, methods using static images cannot measure dynamic muscle activity. Therefore, we used EMG to evaluate the dynamic function of the deltoid and upper trapezius. It is still impossible to measure the force of the deltoid and upper trapezius muscles before RSA, while the EMG measurement of the deltoid and upper trapezius indicating secondary activation can predict the force that patients have postoperatively. While the strength of the deltoid can be measured directly using conventional manual tests, severe pain and marked superior migration of the humeral head in the dynamic condition can affect the results. We found that preoperative strength measured with a handheld dynamometer was not correlated with the postoperative strength or active ROM after RSA, while the preoperative EMG amplitude in the middle deltoid was correlated with postoperative strength. Patients with greater EMG activity in the middle and anterior deltoid had a more ROM in forward flexion. The EMG activity of the posterior deltoid was related to ROM in external rotation independent of infraspinatus tears. Latissimus dorsi muscle transfer enhances external rotation, at the cost of a potential loss of internal rotation.11 The
20
enhance the power of external rotation.23 Therefore, rehabilitation of the posterior
deltoid muscle may enhance the external rotation of the shoulder after RSA, although further studies are needed. Compared to the deltoid muscle, the function of the upper trapezius muscle in the shoulder with RSA has not been well studied. One study showed that after RSA, upper trapezius EMG activity during abduction was greater than in normal shoulders.29 In patients with rotator cuff tears, the increased EMG
activity in the upper trapezius plays a compensatory role during abduction between 60° and 120°.13 To the best of our knowledge, our study is the first to correlate the
activity of the upper trapezius with the postoperative results of RSA. EMG amplitudes in the upper trapezius were related to the recovery of strength in 90° of abduction; this can occur because after RSA the upper trapezius muscle works in the middle range of abduction, helping the middle deltoid muscle.
The strengths of this study were its prospective design using the same technique and instrument, the preoperative measurements of the EMG activity of patients with CTA or OA with a large rotator cuff tear, and the inclusion of a relatively large number of patients in a dynamic EMG study. Confounding factors affecting the prognosis of RSA, such as age and sex, were controlled statistically. Nevertheless, this study had some limitations. First, dynamic EMG measurements can be affected by the patient’s experience of severe pain and willingness or volitional ability to forcefully contract muscles. To control for this, the EMG signals should be normalized using the MVC or RVC. Although the MVC method is commonly used for healthy subjects, the RVC method is good for patients who find it difficult to exert maximal or submaximal power because of severe joint pain.8,20 Given the
characteristics of our patients with CTA or OA with large cuff tears, it was impossible to perform MVC. Therefore, standing erect with both arms at the sides was adopted as the reference posture. Second, for 13 patients with pseudoparalysis, the EMG was not measured at 90° during forward flexion or abduction. Only one dynamic EMG
21
study of RSA patients has recorded the muscle activities during weighted abduction and flexion after RSA, using a 1.5 kg weight.29 However, we measured the EMG
before surgery, and in a preliminary study, found that the weighted abduction and flexion proved impossible; therefore, we measured the EMG activity during shrugging, forward flexion, and abduction without a weight. Although it was difficult for some preoperative patients to attain 90° of abduction or flexion, the EMG amplitudes measured in these patients were related to the clinical results.
22
23
Postoperative shoulder strength after RSA was increased in patients with greater preoperative EMG activity in the middle deltoid and upper trapezius. Preoperative EMG activity of the anterior or middle deltoid muscle was associated with active ROM of flexion or abduction, while EMG activity of the posterior deltoid was associated with the active ROM of external rotation. Therefore, preoperative EMG measurements of these muscles will help to predict the postoperative outcome of RSA and set reasonable post-surgical patient expectations in the preoperative setting.
24
REFERENCES
1. Angst F, Schwyzer HK, Aeschlimann A, Simmen BR, Goldhahn J. Measures of adult shoulder function: Disabilities of the Arm, Shoulder, and Hand Questionnaire (DASH) and its short version (QuickDASH), Shoulder Pain and Disability Index (SPADI), American Shoulder and Elbow Surgeons (ASES) Society standardized shoulder assessment form, Constant (Murley) Score (CS), Simple Shoulder Test (SST), Oxford Shoulder Score (OSS), Shoulder Disability Questionnaire (SDQ), and Western Ontario Shoulder Instability Index (WOSI). Arthritis care & research 2011;63 Suppl 11:S174-188. 10.1002/acr.20630 2. Boileau P, Watkinson D, Hatzidakis AM, Hovorka I. Neer Award 2005: The
Grammont reverse shoulder prosthesis: results in cuff tear arthritis, fracture sequelae, and revision arthroplasty. J Shoulder Elbow Surg 2006;15:527-540. 10.1016/j.jse.2006.01.003
3. Boileau P, Watkinson DJ, Hatzidakis AM, Balg F. Grammont reverse prosthesis: design, rationale, and biomechanics. Journal of shoulder and elbow surgery 2005;14:147S-161S. 10.1016/j.jse.2004.10.006
4. de Witte PB, Henseler JF, van Zwet EW, Nagels J, Nelissen RG, de Groot JH. Cranial humerus translation, deltoid activation, adductor co-activation and rotator cuff disease - different patterns in rotator cuff tears, subacromial impingement and controls. Clin Biomech (Bristol, Avon) 2014;29:26-32. 10.1016/j.clinbiomech.2013.10.014
5. Ekstrom RA, Donatelli RA, Soderberg GL. Surface electromyographic analysis of exercises for the trapezius and serratus anterior muscles. J Orthop Sports Phys Ther 2003;33:247-258.
25
maximum voluntary isometric contractions for the serratus anterior and trapezius muscles during surface EMG analysis. J Electromyogr Kinesiol 2005;15:418-428. 10.1016/j.jelekin.2004.09.006
7. Ernstbrunner L, Werthel JD, Wagner E, Hatta T, Sperling JW, Cofield RH. Glenoid bone grafting in primary reverse total shoulder arthroplasty. J Shoulder Elbow Surg 2017;26:1441-1447. 10.1016/j.jse.2017.01.011
8. Ettinger L, Weiss J, Shapiro M, Karduna A. Normalization to Maximal Voluntary Contraction is Influenced by Subacromial Pain. Journal of applied biomechanics 2016;32:433-440. 10.1123/jab.2015-0185
9. Farina D, Madeleine P, Graven-Nielsen T, Merletti R, Arendt-Nielsen L. Standardising surface electromyogram recordings for assessment of activity and fatigue in the human upper trapezius muscle. Eur J Appl Physiol 2002;86:469-478. 10.1007/s00421-001-0574-0
10. Fischer C, Krammer D, Hug A, Weber MA, Kauczor HU, Krix M et al. Dynamic contrast-enhanced ultrasound and elastography assess deltoid muscle integrity after reverse shoulder arthroplasty. J Shoulder Elbow Surg 2017;26:108-117. 10.1016/j.jse.2016.04.012
11. Flury M, Kwisda S, Kolling C, Audige L. Latissimus dorsi muscle transfer reduces external rotation deficit at the cost of internal rotation in reverse shoulder arthroplasty patients: a cohort study. J Shoulder Elbow Surg 2019;28:56-64. 10.1016/j.jse.2018.06.032
12. Greiner SH, Back DA, Herrmann S, Perka C, Asbach P. Degenerative changes of the deltoid muscle have impact on clinical outcome after reversed total shoulder arthroplasty. Arch Orthop Trauma Surg 2010;130:177-183. 10.1007/s00402-009-1001-y
26
13. Hawkes DH, Alizadehkhaiyat O, Kemp GJ, Fisher AC, Roebuck MM, Frostick SP. Shoulder muscle activation and coordination in patients with a massive rotator cuff tear: an electromyographic study. Journal of orthopaedic research : official publication of the Orthopaedic Research Society 2012;30:1140-1146. 10.1002/jor.22051
14. Hermens HJ, Freriks B, Disselhorst-Klug C, Rau G. Development of recommendations for SEMG sensors and sensor placement procedures. Journal of electromyography and kinesiology : official journal of the International Society of Electrophysiological Kinesiology 2000;10:361-374.
15. Huskisson EC. Measurement of pain. Lancet 1974;2:1127-1131.
16. Katolik LI, Romeo AA, Cole BJ, Verma NN, Hayden JK, Bach BR. Normalization of the Constant score. Journal of shoulder and elbow surgery 2005;14:279-285. 10.1016/j.jse.2004.10.009
17. Madeleine P, Farina D, Merletti R, Arendt-Nielsen L. Upper trapezius muscle mechanomyographic and electromyographic activity in humans during low force fatiguing and non-fatiguing contractions. European journal of applied physiology 2002;87:327-336. 10.1007/s00421-002-0655-8
18. Meyer DC, Rahm S, Farshad M, Lajtai G, Wieser K. Deltoid muscle shape analysis with magnetic resonance imaging in patients with chronic rotator cuff tears. BMC musculoskeletal disorders 2013;14:247. 10.1186/1471-2474-14-247 19. Mulieri P, Dunning P, Klein S, Pupello D, Frankle M. Reverse shoulder arthroplasty for the treatment of irreparable rotator cuff tear without glenohumeral arthritis. The Journal of bone and joint surgery American volume 2010;92:2544-2556. 10.2106/JBJS.I.00912
27
Electromyographic analysis of the rotator cuff in postoperative shoulder patients during passive rehabilitation exercises. Journal of shoulder and elbow surgery 2013;22:102-107. 10.1016/j.jse.2012.01.021
21. Naveed M, Kitson J, Bunker T. The Delta III reverse shoulder replacement for cuff tear arthropathy: a single-centre study of 50 consecutive procedures. The Journal of bone and joint surgery British volume 2011;93:57-61.
22. Pegreffi F, Pellegrini A, Paladini P, Merolla G, Belli G, Velarde PU et al. Deltoid muscle activity in patients with reverse shoulder prosthesis at 2-year follow-up. Musculoskelet Surg 2017;101:129-135. 10.1007/s12306-017-0516-6
23. Reinold MM, Wilk KE, Fleisig GS, Zheng N, Barrentine SW, Chmielewski T et al. Electromyographic analysis of the rotator cuff and deltoid musculature during common shoulder external rotation exercises. J Orthop Sports Phys Ther 2004;34:385-394.
24. Saha A. Zero Position of the Gleno-Humeral Joint: Its Recognition and Clinical Importance: Hunterian Lecture delivered at the Royal College of Surgeons of England on 10th July 1957. Annals of the Royal College of Surgeons of England 1958;22:223.
25. Schwartz DG, Cottrell BJ, Teusink MJ, Clark RE, Downes KL, Tannenbaum RS et al. Factors that predict postoperative motion in patients treated with reverse shoulder arthroplasty. Journal of shoulder and elbow surgery 2014;23:1289-1295. 10.1016/j.jse.2013.12.032
26. Sousa AS, Tavares JMR. Surface electromyographic amplitude normalization methods: a review. Electromyography: new developments, procedures and applications 2012.
28
PM. Pathological muscle activation patterns in patients with massive rotator cuff tears, with and without subacromial anaesthetics. Man Ther 2006;11:231-237. 10.1016/j.math.2006.07.004
28. Steenbrink F, de Groot JH, Veeger HE, van der Helm FC, Rozing PM. Glenohumeral stability in simulated rotator cuff tears. Journal of biomechanics 2009;42:1740-1745. 10.1016/j.jbiomech.2009.04.011
29. Walker D, Wright TW, Banks SA, Struk AM. Electromyographic analysis of reverse total shoulder arthroplasties. J Shoulder Elbow Surg 2014;23:166-172. 10.1016/j.jse.2013.05.005
30. Walker DR, Kinney AL, Wright TW, Banks SA. How sensitive is the deltoid moment arm to humeral offset changes with reverse total shoulder arthroplasty? J Shoulder Elbow Surg 2016;25:998-1004. 10.1016/j.jse.2015.10.028
31. Walker DR, Struk AM, Matsuki K, Wright TW, Banks SA. How do deltoid muscle moment arms change after reverse total shoulder arthroplasty? J Shoulder Elbow Surg 2016;25:581-588. 10.1016/j.jse.2015.09.015
32. Whatley AN, Fowler RL, Warner JJ, Higgins LD. Postoperative rupture of the anterolateral deltoid muscle following reverse total shoulder arthroplasty in patients who have undergone open rotator cuff repair. Journal of shoulder and elbow surgery 2011;20:114-122. 10.1016/j.jse.2010.04.049
33. Wiater BP, Koueiter DM, Maerz T, Moravek JE, Jr., Yonan S, Marcantonio DR et al. Preoperative deltoid size and fatty infiltration of the deltoid and rotator cuff correlate to outcomes after reverse total shoulder arthroplasty. Clin Orthop Relat Res 2015;473:663-673. 10.1007/s11999-014-4047-2
34. Winter DA. Biomechanics and motor control of human movement: John Wiley & Sons; 2009. (ISBN No. 0470398183)
29
35. Yoon JP, Seo A, Kim JJ, Lee CH, Baek SH, Kim SY et al. Deltoid muscle volume affects clinical outcome of reverse total shoulder arthroplasty in patients with cuff tear arthropathy or irreparable cuff tears. PLoS One 2017;12:e0174361. 10.1371/journal.pone.0174361