: . . , . . : 1994 6 2002 3 - 1987 2 109 , , . : 109 18 (16.5%), 91 (83.5%) 45.1± 14.2 . 64
(58.7%) , 45 (41.3%) . 31%, 13% (p=0.047). (8045.3±2543.3/ vs 6835.6±1957.6/ , p=0.009) (305±81.7x103/ vs 264.4±83.2x103/ , p=0.01) . (49.1±36.8 /hr vs 26.6±24.3 /hr, p=0.001) C (2.9±4.1 / vs 0.8±1.2 / , p=0.001) .
disease modifying antirheumatic drug (DMARD)
(92.2% vs 71.1%, p=0.003), (46.9% vs 28.9%, p<0.05). : . : , , , DMARD,
그 림 차 례
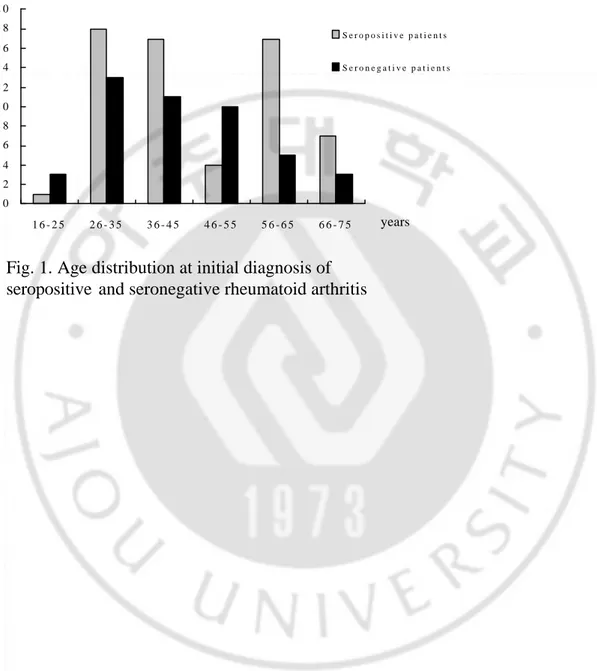
Fig 1. Age distribution at initial diagnosis of seropositive and seronegative
rheumatoid arthritis ... 19
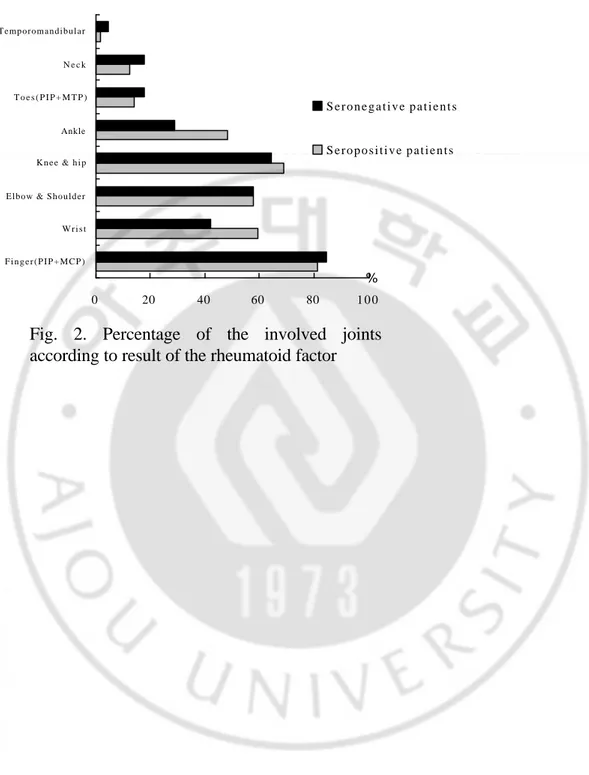
Fig 2. Percentage of the involved joints according to result of the rheumatoid factor
... 20
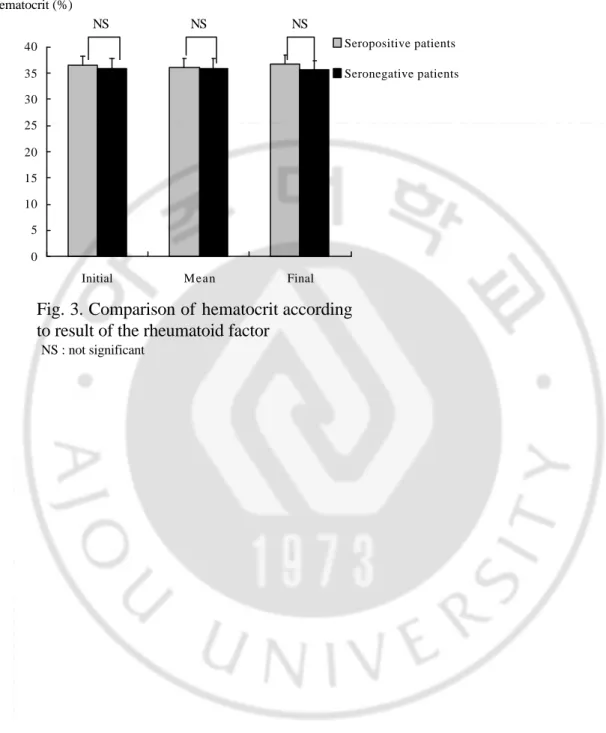
Fig 3. Comparison of hematocrit according to result of the rheumatoid factor ... 21
Fig 4. Comparison of white blood cell (WBC) count according to result of the
rheumatoid factor ... 22
Fig 5. Comparison of platelet count according to result of the rheumatoid factor
... 23
Fig 6. Comparison of erythrocyte sedimentation rate (ESR) according to result of the
rheumatoid factor ... 24
Fig 7. Comparison of C-reactive protein (CRP) according to result of the rheumatoid
factor ... 25
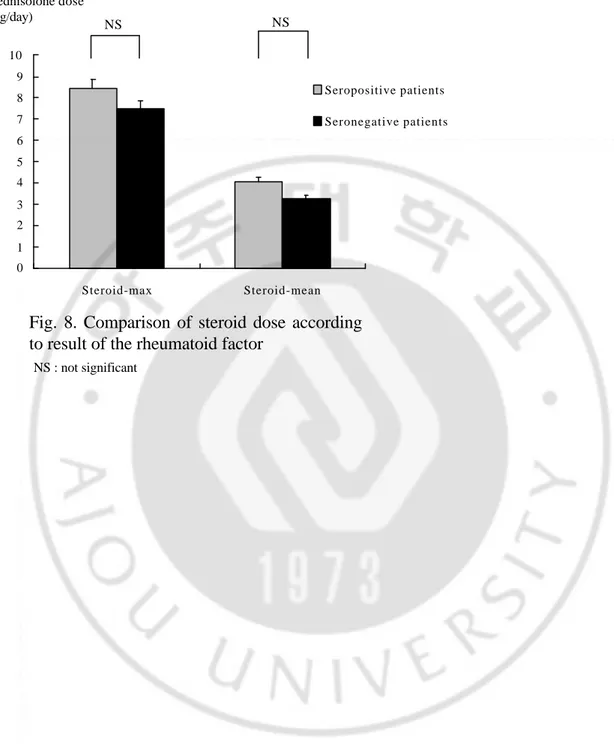
Fig 8. Comparison of steroid dose according to result of the rheumatoid factor
... 26
Table 1. Demographic characteristics of the study subject ... 27
Table 2. Disease modifying antirheumatic drug usage according to result of the
rheumatoid factor ... 28
I.
. , , , , , , , , .1,2 , C , .2,3 G Fc 1940 Waaler Rose ,4 1949 Pike .5 , , , , 5%, 25% . , .6,7 , , .II.
A. 1994 6 2002 3 -230 1987 2 109 . B. 109 , , , , , , , , Sicca , , C , , , , , ., DMARD (disease modifying antirheumatic drug) , .
C.
SPSS version 10.0 (Statistical Package for
the Social Sciences, Chicago, Il) , T
, ± p 0.05
III.
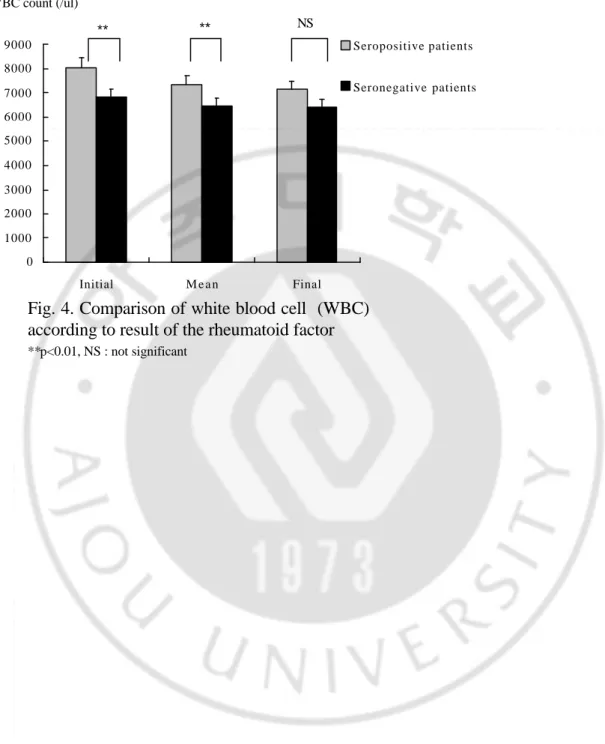
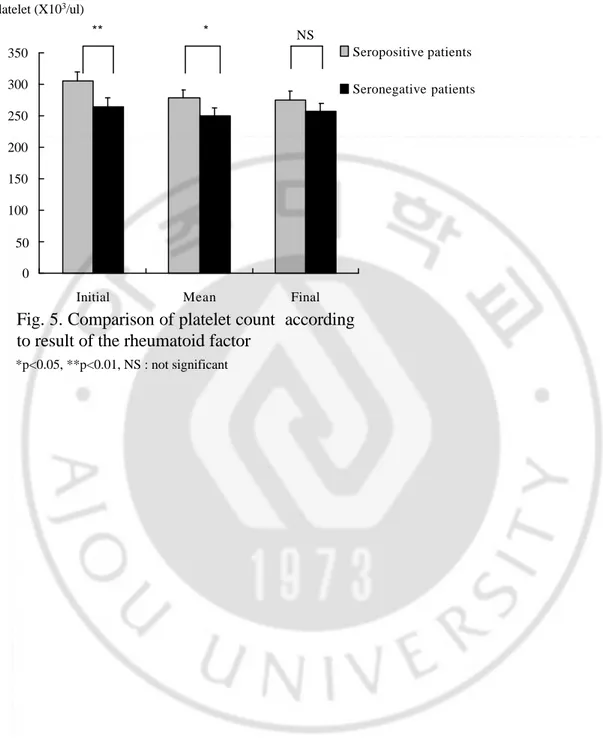
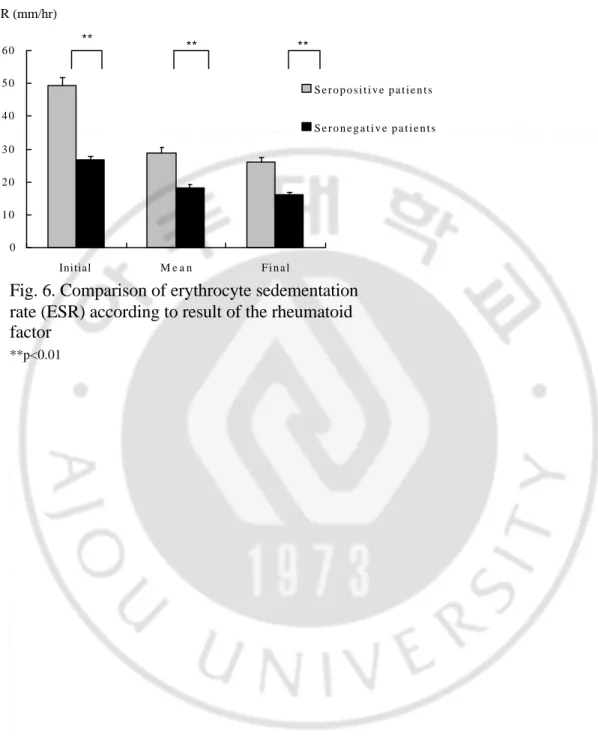
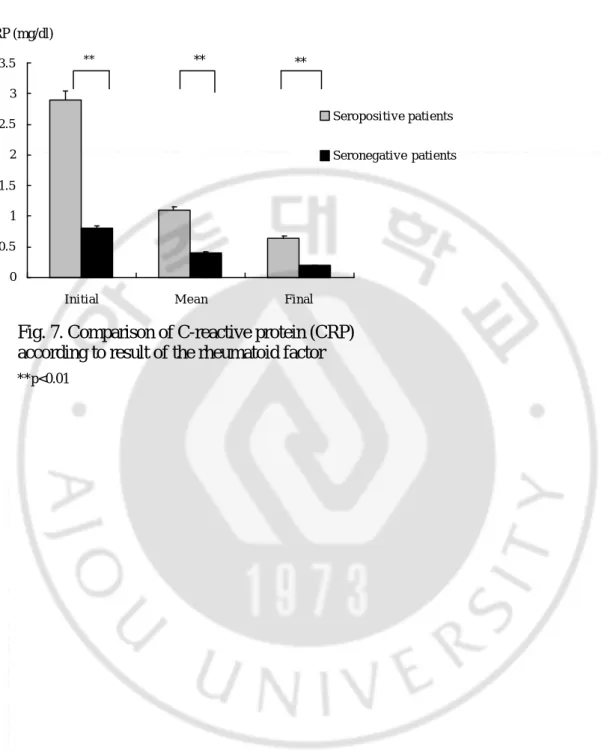
A. 109 64 (58.7%) , 45 (41.3%) . 12 , 52 1:4.3 , 6 , 39 1:6.5 . 46.2± 14.5 ( : 16-75 ), 43.6± 13.8 ( : 20-75 ) (Fig. 1). 30.9±26.8 , 21.5±21.1 , 36.6±16.8 , 35.5±17 . 85%, 93% (Table 1). ( ), , , , , , , (p=0.041) (Fig. 2). 14 , 5 , Sicca 64 8 45 8 , 3 2 .B. 31%, 13% .(p=0.047) 36.4±4.7% 36±4.1% (p=0.7, NS), 36.7± 4.7% 35.7±4.7% (p=0.27, NS), 36.1±4.2% 36±2.9% (p=0.97, NS) (Fig. 3a), 8045±2543/ 6836±1957/ (p<0.01), 7154±2397/ 6436±1908/ (p=0.09, NS), 7327±1922/ 6460±1292/ (p=0.01) (Fig. 3b). 305±81.7x103/ 264.4±83.2x103/ (p<0.01), 275.9±80.5x103/ 257.9±72.3x103/ (p=0.23, NS), 277.8±71.3x103/ 249.4±58.8x103/ (p<0.05) (Fig. 3c). 49.1±36.8 /hr 26.6±24.3 /hr (p<0.01), 26.1±20.8 /hr 16±9.4 /hr (p<0.01), 28.8±19.3 /hr 18.2±13.2 /hr (p<0.01) (Fig. 4). C 2.9±4.1 / 0.8±1.2 / (p<0.01), 0.6±1.1 /
0.2± 0.4 / (p<0.01), 1.1± 1.4 / 0.4±0.5 / (p<0.01)
(Fig. 5).
C.
DMARD (disease modifying antirheumatic drug) hydroxychloroquine, sulfasalazine, methotrexate, bucillamine
hydroxychloroquine 64 58 90.6%, 45 36 80% , sulfasalazine 64 54 84.4%, 45 37 82.2% , methotrexate 64 47 73.4%, 45 27 60% , bucillamine 64 1 1.6%, 45 2 4.4% . DMARD 64 59 92.2% , 45 32 71.1% (p=0.003) 64 30 46.9%, 45 13 28.9% (p<0.05)(Tab 2). ( ) ( )
4.07±2.98 /day 3.27±3.01 /day (p=0.16), 8.49±4.12
IV.
, , , , , , , , , , C .1,2,3 .8 Papadopoulos , , , , , , ,9 Masi ,10 Van de heijde , , C , , .3 , ,, , , . , 20-30% 11 . , Amos C ,12 , C , , .13,14 , C , . ,15 ,16 . DMARD
. , 31% 13% , 35% speckled homogeneous ,17 Masi ,10 .18 Papadopoulos
hydroxychloroquine, D-penicillamine, methotrexate
,9 MÖttÖnen 6.2 3.3 DMARD 19 DMARD . DMARD , DMARD . , , DMARD
.
, .
V.
, DMARD .
Fig. 1. Age distribution at initial diagnosis of
seropositive and seronegative rheumatoid arthritis
0 2 4 6 8 1 0 1 2 1 4 1 6 1 8 2 0 1 6 - 2 5 2 6 - 3 5 3 6 - 4 5 4 6 - 5 5 5 6 - 6 5 6 6 - 7 5 S e r o p o s i t i v e p a t i e n t s S e r o n e g a t i v e p a t i e n t s Number of persons years
Fig. 2. Percentage of the involved joints
according to result of the rheumatoid factor
0 20 40 60 80 1 0 0
F i n g e r ( P I P + M C P ) W r i s t Elbow & Shoulder K n e e & h i p Ankle T o e s ( P I P + M T P ) N e c k Temporomandibular S e r o n e g a t i v e p a t i e n t s S e r o p o s i t i v e p a t i e n t s %
Fig. 3. Comparison of hematocrit according
to result of the rheumatoid factor
Hematocrit (%) 0 5 10 15 20 25 30 35 40
Initial Mean Final
Seropositive patients Seronegative patients
NS NS NS
Fig. 4. Comparison of white blood cell (WBC)
according to result of the rheumatoid factor
0 1000 2000 3000 4000 5000 6000 7000 8000 9000 Initial M e a n Final Seropositive patients Seronegative patients **p<0.01, NS : not significant ** NS WBC count (/ul) **Fig. 5. Comparison of platelet count according
to result of the rheumatoid factor
0 50 100 150 200 250 300 350
Initial Mean Final
Seropositive patients Seronegative patients *p<0.05, **p<0.01, NS : not significant ** NS Platelet (X103/ul) *
Fig. 6. Comparison of erythrocyte sedementation
rate (ESR) according to result of the rheumatoid
factor
0 1 0 2 0 3 0 4 0 5 0 6 0 Initial M e a n F i n a l S e r o p o s i t i v e p a t i e n t s S e r o n e g a t i v e p a t i e n t s **p<0.01 ESR (mm/hr) ** ** **Fig. 7. Comparison of C-reactive protein (CRP)
according to result of the rheumatoid factor
0 0.5 1 1.5 2 2.5 3 3.5 Initial M e a n Final Seropositive patients Seronegative patients ** **p<0.01 CRP (mg/dl) ** **Fig. 8. Comparison of steroid dose according
to result of the rheumatoid factor
0 1 2 3 4 5 6 7 8 9 10 Steroid-max Steroid-mean Seropositive patients Seronegative patients Prednisolone dose (mg/day) NS NS NS : not significant
Table 1. Demographic characteristics of the study subject
NS 43.6±13.8 20-75 46.2±14.5 16-75 Age at diagnosis (years)Mean Range
NS 35.5±17.0
36.6±16.8 Follow up time (months)
0.047* 13 31 ANA (%) NS 93 85 Morning stiffness (%) NS 21.5 30.9 Disease duration before
diagnosis (months) NS 1:6.5 1:4.3 M:F ratio NS 39 52 Female NS 6 12 Male P-value Seronegative (n=45) Seropositive (n=64) *p<0.05 , NS : not significant
Table 2. DMARD dose according to result of the rheumatoid factor
0.003* 71.1 32 92.2 59 Combination 0.37 4.4 2 1.6 1 Bucilamine 0.05* 28.9 13 46.9 30 Triple combination 0.75 42.2 19 45.3 29 Double combination 0.14 60 27 73.4 47 Methotrexate 0.77 82.2 37 84.4 54 Sulfasalazine 0.12 80 36 90.6 58 Hydroxychloroquine % n % n P value Seronegative (n=45) Seropositive (n=64) *p<0.051. Deal CL, Meenan RF, Goldenberg DL, Anderson JJ, Sack B, Pastan RS, et al: The clinical features of elderly-onset rheumatoid arthritis. Arthritis Rheum 28:987-94, 1985
2. Fleming A, Crown JM, Corbett M: Prognostic value of early features in rheumatoid disease. Br Med J 1:1243-5, 1976
3. Van de Heijde DM, Van Riel PL, Van Rijswij MH, Van de Putte LB: Influence of prognostic features on the final outcome in rheumatoid arthritis: a review of literature. Semin Arthritis Rheum 17:284-92, 1988
4. Waaler E: On the occurrence of a factor in human serum activating the specific agglutination of sheep blood corpuscles. Acta Pathol Microbiol Scand 17:172-88, 1940
5. Pike RM, Sulkin SE, Coggeshall HC: Serological reactions in rheumatoid arthritis. II. Concerning the nature of the factor in rheumatoid arthritis serum responsible for increased agglutination of sensitized sheep erythrocytes. J Immunol 63:448-63, 1949
6. Scott DL: Prognostic factors in early rheumatoid arthritis. Rheumatology 39:24-9, 2000
7. Kaltenhauser S, Wagner U, Schuster E: Immunogenetic markers and seropositivity predict radiological progression in early rheumatoid arthritis independent of disease activity. J Rheumatol 28:735-44, 2001
8. Drosos AA, Lanchbury JS, Panayi GS, Moutsopoulos HN: Rheumatoid arthritis in Greek and British patients: a comparative clinical radiological and serological study. Arthritis Rheum 35:745-8, 1992
9. Papadopoulos IA, Katsimbri P, Katsaraki A, Temekonidis T, Georgiadis A, Drosos AA: Clinical course and outcome of early rheumatoid arthritis. Rheumatol Int
20:205-10, 2001
10. Masi AT, Maldonado-Cocco JA, Kaplan SB, Feigenbaum SL, Chandler RW: Prospective study of the elderly course of rheumatoid arthritis in young adults: comparison of patients with and without rheumatoid factor positivity at entry and identification of variables correlating with outcomes. Semin Arthritis Rheum 5:299-326, 1976
11. Lipsky P: Rheumatoid arthritis: Harrison's principles of internal medicine. 15th ed. (ed. Wilson JD, Petersdorf RG and Martin JB), NewYork, McGraw-Hill, 2001, pp 1928-37
12. Amos RS, Constable TJ, Crockson RA, Crockson AP, McConkey B: Rheumatoid arthritis: relation of serum C-reactive protein and erythrocyte sedimentation rates to radiographic changes. Br Med Jr 22:195-7, 1977
13. Van Zeben D, Hazes JMW, Zwinderman AH, Cats A, Van der Voort EAM, Breadveld FC: Clinical significance of rheumatoid factor in early rheumatoid arthritis-results of a follow up study. Ann Rheum Dis 51:1029-35, 1992
14. Sjoblom KG, Saxne T, Petterson H, Wollheim FA: Factors related to the progression of joint destruction in rheumatoid arthritis. Scand J Rheumatol 13:21-7, 1984
15. , , , , , :
. 47:821-9, 1994
16. , : .
56:745-52, 1999
17. Nishimura S, Nishiya K, Hisakawa N, Chikazawa H, Ookubo S, Nakatani K, et al: Positivity for antinuclear antibody in patients with advanced rheumatoid arthritis. Acta Med Okayama 50:261, 1996
Laboratory, and radiographic features of rheuamtoid arthritis with and without nodules. Rev Rheum Engl Ed 64:11, 1997
19. MÖttÖnen T, Paimela L, Ahonen J, Helve T, Hannonen P, Leirisalo-repo M:
Outcome in patients with early rheumatoid arthritis treated according to the "sawtooth" strategy. Arthritis Rheum 39:996-1005, 1996
-Abstract-Clinical Significance of Rheumatoid Factor in Rheumatoid Arthritis
Yoo-Seob Shin
Department of Medical Sciences
The Graduate School, Ajou University
(Supervised by Assistant Professor Chang-Hee Suh)
Purpose : Serum rheumatoid factor (RF) is important in the diagnosis and prognosis
of rheumatoid arthritis (RA). This purpose of this study is to evaluate the clinical characteristics and treatments of RA according the presence of RF in Korean.
Materials and Method : A retrospective analysis was performed on the records of
109 patients followed at least 2 years at Ajou University Hospital among 230 RA patients fulfill the 1987 revised American College of Rheumatology criteria of RA from June, 1994 to March 2002.
Results : Sixty-four patients had positive RF (58.7%) and 91 patients were female
(83.5%). There were no difference in demographic characteristics, joint involvements and duration of morning stiffness between RF positive and negative patients. Antinuclear antibody was detected more frequently in the RF positive (p=0.047). In RF positive RA patients, white blood cell and platelets counts were higher 8045.3± 2543.3/ vs 6835.6±1957.6/ , p=0.009 and 305±81.7x103/ vs 264.4±83.2x103/ , p=0.01, respectively. Inflammatory markers such as ESR and CRP were also higher in the RF positive 49.1±36.8 /hr vs 26.6±24.3 /hr, p=0.001 and 2.9±4.1 / vs 0.8±1.2 / , p=0.001, respectively. There is no difference in the use of disease modifying antirheumatic drug (DMARD) except that combination therapy was more commonly used in the RF positive RA patients (p<0.05).
Conclusion : Disease activity was more severe in RF positive than RF negative RA
patients. More aggressive treatments were needed in RF positive patients.
Key word : Rheumatoid arthritis, Rheumatoid factor, inflammation, DMARD, combination therapy