ABSTRACT
Background and Objectives: Nonalcoholic fatty liver disease (NAFLD) is an excessive accumulation of fat into the liver as a result of increased inflammation and insulin resistance.
Although there can be common pathogenic mechanisms for NAFLD and hypertension associated with the development of cardiovascular diseases, little data are showing the association between NAFLD and hypertension in a large-scale cohort study. Thus, we evaluated the ability of the fatty liver index (FLI), a surrogate marker of NAFLD, to predict the development of hypertension in healthy individuals.
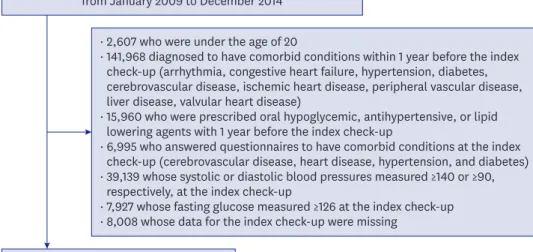
Methods: We included 334,280 healthy individuals without known comorbidities who underwent the National Health check-ups in South Korea from 2009 to 2014. The association between the FLI and hypertension was analyzed using multivariate Cox proportional-hazards models.
Results: During a median of 5.2 years' follow-up, 24,678 subjects (7.4%) had new-onset hypertension. We categorized total subjects into quartile groups according to FLI (range: Q1, 0–4.9; Q2, 5.0–12.5; Q3, 12.6–31.0; and Q4, >31.0). The incidence of hypertension was higher in subjects with the highest FLI than in those with the lowest FLI (Q4, 9,968 [11.9%] vs. Q1, 2,277 [2.7%]; p<0.001). There was a significant correlation between the highest FLI and an increased risk of new-onset hypertension (adjusted hazard ratio between Q4 and Q1, 2.330;
95% confidence interval, 2.218–2.448; p<0.001). FLI was significantly associated with an increased risk of new-onset hypertension regardless of baseline characteristics.
Conclusions: Higher FLI was independently associated with increased risk of hypertension in a healthy Korean population.
Keywords: Fatty liver, nonalcoholic; Hypertension; Healthy people programs
Original Article
Received: Nov 19, 2019 Revised: Feb 10, 2020 Accepted: Mar 10, 2020 Correspondence to Jae-Hyeong Park, MD, PhD
Department of Cardiology in Internal Medicine, Chungnam National University Hospital, Chungnam National University School of Medicine, 282, Munhwa-ro, Jung-gu, Daejeon 35015, Korea.
E-mail: [email protected]
Copyright © 2020. The Korean Society of Cardiology
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (https://
creativecommons.org/licenses/by-nc/4.0) which permits unrestricted noncommercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
ORCID iDs Jae-Hyung Roh
https://orcid.org/0000-0003-3675-3541 Jae-Hyeong Park
https://orcid.org/0000-0001-7035-286X Hanbyul Lee
https://orcid.org/0000-0002-1479-8995 Yong-Hoon Yoon
https://orcid.org/0000-0002-5598-003X Minsu Kim
https://orcid.org/0000-0001-9230-3137 Yong-Giun Kim
https://orcid.org/0000-0002-0816-9025 Gyung-Min Park
https://orcid.org/0000-0001-5846-0606
Jae-Hyung Roh , MD, PhD
1, Jae-Hyeong Park , MD, PhD
1, Hanbyul Lee , MS
2, Yong-Hoon Yoon , MD
1, Minsu Kim , MD, PhD
1, Yong-Giun Kim , MD, PhD
3, Gyung-Min Park , MD, PhD
3, Jae-Hwan Lee , MD, PhD
1, and
In-Whan Seong , MD, PhD
11
Department of Cardiology in Internal Medicine, Chungnam National University Hospital, Chungnam National University School of Medicine, Daejeon, Korea
2
Department of Statistics, Kyungpook National University, Daegu, Korea
3