Copyright 2018 The Korean Society of Neuro-Ophthalmology http://neuro-ophthalmology.co.kr 37
미로경색의 임상진단: 증례보고와 문헌고찰
전승호, 신병수, 서만욱, 오선영 전북대학교 의과대학 신경과학교실
Clinical Diagnosis of Labyrinth Infarction: Report of a Case and Literature Review
Seung-Ho Jeon, MD, Byoung-Soo Shin, MD, Man-Wook Seo, MD, Sun-Young Oh, MD Department of Neurology, Chonbuk National University Medical School and Hospital, Jeonju, Korea
Labyrinth infarction is leading to prolonged vertigo and hearing loss without other brainstem or cerebellar symptoms or signs, which are indistinguishable from viral labyrinthitis. If brainstem or cerebellar lesions manifest vertigo without other neurological signs, they are easily misdiagnosed as peripheral-type of vertigo. Herein, we report a patient with stenosis of mid basilar artery presenting with prolonged vertigo, unidirectional spontaneous nystagmus and ipsilateral sensory hearing impairment. The symp- toms and signs resembled acute peripheral labyrinthitis, and the caveats for differential diagnosis were discussed. A 75-year-old female visited the emergency room due to acute onset of severe vertigo, nausea and gait ataxia. Neurologic examination revealed the left-beating horizontal-torsional mixed nystagmus, dysmetria on the left side and falling tendency to the left during tandem gait. Hearing impairment on the right ear was also observed. Video head-impulse test (vHIT) revealed a covert and overt catch-up saccade in right posterior and lateral canals. Brain magnetic resonance imaging showed acute multifocal infarctions in the cerebel- lum, occipital and frontal lobe on the left side and the right occipital lobe. Brain magnetic resonance angiography showed mid basilar artery stenosis. We diagnosed as acute infarction due to a stenosis of basilar artery which supply labyrinthine arteries. Physi- cian should consider labyrinthine artery infarction in patients with acute onset of severe vertigo with unilateral hearing impair- ment.
Keywords: Inner ear infarction; Anterior inferior cerebellar artery; Labyrinth infarction
서 론
전하소뇌동맥(anterior inferior cerebellar artery, AICA)은 전정기관 에 혈액을 공급하는 중요한 혈관으로 내이뿐만 아니라 가쪽뇌교, 중 간소뇌다리, 타래(flocculus)를 포함하는 전하소뇌를 지배하고 있으 며, 완전 전하동맥경색에서는 동측으로의 안구기울임반응(ocular tilt reaction), 청력소실, 안면마비, 사지와 안면 감각소실, 실조, 겨냥이상 과 같은 증상이 동반될 수 있다. 내이의 혈액공급은 전하소뇌동맥의 분지인 미로동맥(labyrinthine artery)으로부터 이루어지며, 다른 신경 학적 증상 또는 징후를 동반하지 않는 단독 내이기능장애만을 보이
는 경우, 즉, 갑자기 시작된 극심한 지속적인 어지럼, 청력소실, 회선성 분을 동반한 일측성 자발수평안진만을 보이는 경우에는 중추성 병터 인지 감별이 쉽지 않다. 이러한 환자들에서 전하소뇌동맥의 국소 협 착이나 폐색에 의한 증상인지 감별하는 것이 임상적으로 중요하겠다.
저자들은 최근 우측 전정기능이상과 청력소실로 내원하여 말초성 어지럼을 시사하였으며 신경학적 검진에서 소뇌증상과 함께 전하소 뇌동맥 기시부인 기저동맥의 중앙부위의 국소협착이 동반되어 있어 임상적으로 내이동맥 영역의 허혈성 뇌졸중에 의한 증상으로 판단되 는 한 증례를 경험하여, 중추성 전전병증과 말초성 전정병증의 감별 에 대한 고찰과 함께 증례보고 하고자 한다.
Correspondence to: Sun-Young Oh, MD
Department of Neurology, Chonbuk National University Hospital, 20 Geonji-ro, Deokjin-gu, Jeonju 54907, Korea Tel: +82-63-250-1896, Fax: +82-63-251-9363, E-mail: [email protected]
Received: Oct. 17, 2017 / Accepted: Jan. 14, 2018
CASE REPORT
ISSN: 2234-0971 대한안신경의학회지: 제8권 제2호
Clin Neuroophthalmol 8(2):37-40, December 2018
Jeon SH, et al. • Clinical Diagnosis of Labyrinth Infarction
Clin Neuroophthalmol 8(2):37-40, December 2018 38 http://neuro-ophthalmology.co.kr
증 례
평소 건강하던 75세 여자가 갑자기 발생한 어지럼을 주소로 응급실 에 내원했다. 비회전성 어지럼으로 균형을 잡지 못하고 왼쪽으로 쓰러 지는 경향과 중심을 잡지 못하고 흔들거리는 불균형(imbalance)과 실 조(ataxia)를 보였다. 내원 전날 자다가 화장실에 가려고 하던 중 어지
럼이 발생하였고, 평소 먹지 않던 한약을 복용한 후 체한 것 같다고 호 소하였으며 오심과 구토를 동반하였다. 자세변화에 따른 악화나 완화 는 없었다. 내원 당시 활력지수는 혈압 130/80 mmHg, 맥박 70회/분, 호 흡수 18회/분, 체온 36.7°C이었으며, 혈액검사, 생화학검사, 흉부방사 선 및 심전도 검사상 경한 심방세동 이외 뚜렷한 이상소견은 관찰되 지 않았다. 당뇨나 고혈압, 음주, 흡연 등의 과거력은 없었으며, 2년 전
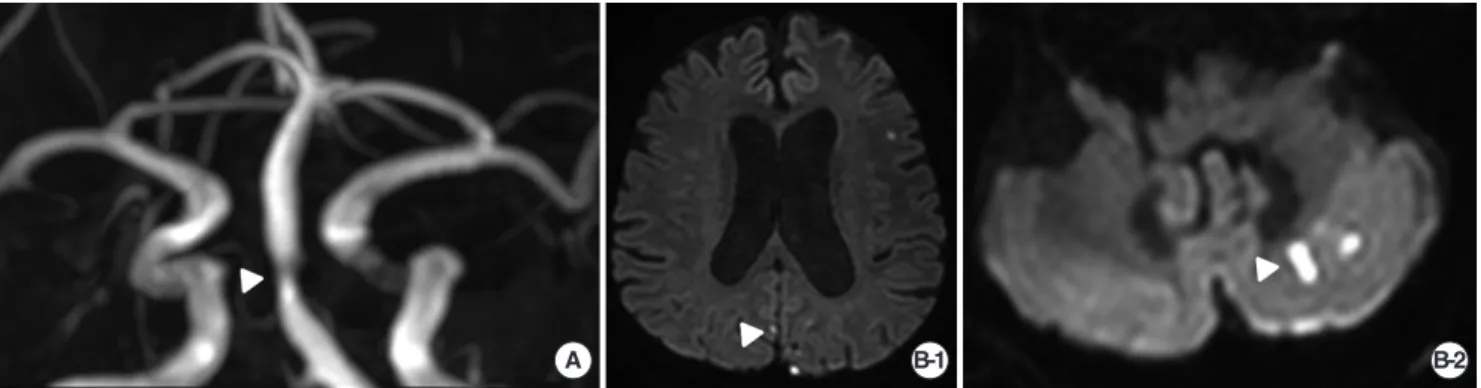
Fig. 1. Brain MR imaging of the patient with acute unilateral vestibulo-cochlear syndrome. (A) Intracranial MR angiography of the patient shows focal stenosis in the mid basilar artery (arrow head). (B) Diffusion-weighted images (DWI) show acute multifocal infarction involving the right medial occipital lobe (arrow head, B-1) and the left cerebellum (arrow head, B-2).
B-2 B-1
A
Fig. 2. Laboratory findings of the patient with acute unilateral vestibulo-cochlear syndrome. (A) Ocular VEMP and Cervical VEMP induced by sound stimulation (500 Hz tone burst) show no response at the right side. (B) Video Head-impulse test reveals decreased gain (0.55) with overt catch-up saccades in the right posterior and in the right lateral semicircular canal. (C) Caloric test reveals caloric paresis on the right side with 57.8% of CP. (D) Pure tone audiogram (PTA) shows severe conduction and sensory-neural mixed hearing loss on the right side. VEMP, vestibular-evoked myogenic potentials.
A B
D C
미로경색의 임상진단 • 전승호 외
Clin Neuroophthalmol 8(2):37-40, December 2018 http://neuro-ophthalmology.co.kr 39
어지럼을 주소로 내원하여 촬영한 뇌자기공명영상검사는 정상이었 으며 기립경검사에서 기립성저혈압을 보여 외래 추시중이었다.
신경학적 진찰에서 좌측으로 향하는 수평 및 회선성분을 가진 자 발성 안진이 관찰되었고, 안진의 뱡향은 주시방향 및 자세에 관계없 이 일정하게 좌측으로 향하였으며 시고정에 의해 억제되었다. 스큐편 위는 관찰되지 않았으며, 두부충동검사에서 우측에서 교정성신속안 구운동(corrective catch-up saccades)이 관찰되었다. 소뇌기능검사에 서 왼쪽겨냥이상이 관찰되었으며, 보행 시 왼쪽으로 넘어지려는 경향 이 관찰되었다. 이외에 다른 신경학적인 장애는 보이지 않았으며, 뇌자 기공명영상검사에서 다발성 급성뇌경색이 왼쪽 소뇌, 후두엽, 전두엽 및 오른쪽 후두엽에서 관찰되었고 근위 및 원위 척추동맥 협착 없이 기저동맥 중앙부위의 국소협착이 관찰되었다(Fig. 1). 입원직후 시행 한 실조평가척도검사(Scale for the assessment and rating of ataxia, SARA)에서 9.5/40점이었고, 3차원 영상안구운동검사(3D Video-ocu- lography, 3D-VOG)에서 자발안진이 좌측, 반시계방향으로 관찰되었 으며 이는 시고정에 의해 억제되었으며, 좌측을 주시할 때 안진의 크 기가 커지는 알렉산더 법칙을 만족시켰으나 주시유발안진(gaze- evoked nystagmus)은 관찰되지 않았다. 진동유발과 두진, 자세변화에 서도 이상안진을 비롯한 안진의 역전은 없었다. 비디오두부충동검사 (video head-impulse test, vHIT)에서 우측전반고리관은 정상범위였으 나 우측후반고리관과 우측수평고리관의 이득값(gain)은 감소되었고 (0.55/0.56) 현성신속안구운동(overt catch-up saccade)과 숨은신속안 구운동(covert catch-up saccade)이 관찰되었다(Fig. 2B). 칼로리 검사에 서 우측 반고리관마비(57.8%)와 좌측으로 향하는 안진의 방향우위 (directional predonderance)가 관찰되었으며, 회전의자 검사에서 이득 의 감소, 위상선행 및 우측으로 비대칭이 관찰되었다. 주관적시수직 (subjective visual vertical, SVV) 검사에서는 우측으로 기울임(4.55°)이 관찰되었으며, 전정유발전위검사(vestibular evoked myogenic poten- tials, VEMP)에서 좌측은 정상이었으나 우측에서는 외안근 전정유발 근전위(oVEMP)가 소실되고 경부전정유발근전위(cVEMP)는 P1의 잠 복기가 연장되었는데 이는 우측 전정기능 저하에 의한 소견으로 판단 되었다(Fig. 2). 급성 뇌경색에 대하여 항응고제와 항혈소판제 병합요 법 시행하고 평형 재활치료를 시행하였다. 입원 10일째 시행한 실조평 가척도(SARA)에서 4.5점으로 호전되고 안구운동검사에서도 의미있 는 안진은 관찰되지 않았으며, 청력의 호전은 보이지 않았으나 어지럼 증 및 불균형과 실조 증상 호전되어 퇴원하였다.
고 찰
급성전정증후군(acute vestibular syndrome)은 말초성 또는 중추성
전정병증에 의한 어지럼 증후군으로 두 가지를 감별하는 것이 임상 에서 중요하다.1 전형적인 말초성 급성 전정병증은 지속적인 회전성 어지럼, 주변 환경이 도는 느낌, 병측으로 몸이 치우치는 증상과 자세/
보행 불안정, 오심과 구토 등의 증상을 보인다. 특징적인 신경이학적 징후로는 건측으로 향하는 수평회전성 안진이 시고정에 의해 억제가 능하고, 주관적시수직이 병측으로 편위되며, 두부충동검사(HIT)에 서 병측에서 이상소견을 보이며, 자세불안정과 롬버그검사상 병측으 로 기울어짐, 건측을 향할 때만 관찰되는 톱니바퀴추종안구운동과 주시유발 시에 안진의 방향이 바뀌지 않는 점을 들 수 있다.1 증례 환자 에 있어 왼쪽으로 쓰러지려는 경향, 불균형, 오심과 구토의 임상증상 과 좌측으로 향하는 수평회전성 안진, 주관적 시수직의 편위 및 두부 충동검사는 말초성 병변을 시사하는 징후로 볼 수 있으나, 실조와 갑 작스런 청력 저하는 중추성 병변을 의심해 볼 수 있는 증상으로 볼 수 있다.
전하소뇌동맥(AICA)으로부터 분지되는 미로동맥은 총와우동맥 (common cochlear artery)과 앞전정동맥(anterior vestibular artery)을 내게 되는데 이들로부터 말초전정계는 혈류를 공급받게 되고, 이들 혈관에 허혈이 발생하게 되면 회전성 현훈을 비롯하여 오심, 구토, 자 세불안, 안진 등 말초전정증상도 유발하게 된다.2 즉, AICA 경색에 의 한 소뇌병변에서도 급성 회전성 현훈과 함께 말초성 전정증상이 나 타날 수 있고, 특히 후하소뇌동맥(posterior inferior cerebellar artery, PICA) 영역의 소뇌하부에 국한된 경색에서는 전형적인 소뇌징후 없 이 말초성 일측전정병증 증상만을 보여 임상적으로 구분이 어려울 수 있다.3 이와 같이 임상적으로 말초성 급성 일측전정병증 소견을 보 여 구분이 어려운 중추성 질환들을 가성 전정신경염(pseudo-vestibu- lar neuritis)이라 한다.4
어지럼을 호소하는 대부분의 허혈성 뇌졸중 환자들은 급성전정증 후군의 형태로 보이게 되며, 약 20%만이 국소적 신경학적 징후를 나타 낸다.5 중추성 급성전정증후군을 일으킬 수 있는 해부학적 위치는 8 번 뇌신경의 뿌리 입구 영역(root entry zone), 전정 핵(vestibular nucle- us), 소뇌결절(nodulus), 타래(flocculus)로 알려져 있으나,6 뇌혈관 이상 에 의한 어지럼의 영상학적 진단 정확도는 매우 낮아 약 35%로 알려졌 다.5 전통적으로 지속성 현훈은 뇌졸중의 증상으로 여겨지지 않아왔 었으나, 최근 연구 결과에 의하면 지속성 현훈은 척추기저동맥 허혈 의 초기증상으로 나타날 수 있으며 일과성 또는 지속성 현훈은 후순 환 일과성허혈성발작(TIA)과 뇌졸중의 증상으로 볼 수 있다.7 HINTS
“plus”는 중추성 급성전정증후군을 감별하는 데 99%의 민감도와 97%
의 특이도를 갖는 검사방법으로 기존의 HINT방법보다 예민한 것으 로 알려졌다.7,8 본 증례의 경우도 HINTS상으로는 말초성 급성전정증 후군에 해당하였으나 HINTS plus 평가 시 청력저하가 동반되어 있어
Jeon SH, et al. • Clinical Diagnosis of Labyrinth Infarction
Clin Neuroophthalmol 8(2):37-40, December 2018 40 http://neuro-ophthalmology.co.kr
중추성 급성전정증후군으로 평가할 수 있었다.
전하동맥(AICA)의 폐쇄는 대부분의 경우에서 죽상혈전증(athero- thrombotic)에 의하며, 기저동맥의 플라크가 전하동맥의 입구까지 연 장되어 있거나 미세죽상판(microatheroma)이 막는 기전으로 설명한 다.9 이러한 이유로 전하동맥 영역 단독 뇌경색의 경우 혈관조영술에 서 기저동맥이 대개 정상으로 보이는 것이다. 본 증례의 경우, 심방 세 동으로 인한 색전성 뇌경색의 가능성도 고려할 수 있으나, 전하동맥 영역에 대하여는 2년 전 촬영한 뇌자기공명영상과 비교 시 기저동맥 의 죽상혈전증에 의한 협착이 진행되었음이 관찰되고 있어 죽상동맥 경화에서 시작된 미세 색전에 의한 다발성 색전성 허혈 뇌졸중이 발 생한 것으로 보인다.
미로동맥은 곁순환이 거의 없는 끝동맥으로 내이에 혈액공급을 하는 혈관이다. 내이는 미로동맥의 경색으로 인한 허혈성 손상에 매 우 취약한 기관으로, 허혈성 손상 발생 시 심하게 주위가 도는 현훈, 수평과 회선 성분을 가지는 자발안진과 함께 청력소실을 호소하게 된
다.10,11 일부 연구에 의하면 청각 및 평형 기능의 손상을 동반한 미로동
맥 뇌경색은 전하동맥 영역의 뇌경색의 중요한 징후라고 기술하고 있 다.12 전하소뇌동맥 경색의 7.4%는 단독 내이경색으로 대부분 자기공 명영상의 확산강조영상에서 정상으로 나타나게 된다.13 따라서 고혈 압, 당뇨와 같은 혈관손상 위험인자를 가진 노년층에서 급성 일측전 정병증과 함께 청력소실을 호소하는 증상이 발생했을 경우에는 반드 시 미로경색의 가능성을 염두에 두어야 한다(HINT plus). 특히 본 증 례의 환자에서처럼 자기공명혈관촬영영상에서 후방순환계 혈관의 심한 협착 또는 폐색이 관찰되는 경우 전하동맥 영역에서 의미 있는 병변이 관찰되지 않더라도 뇌경색 가능성을 두고 이에 대한 치료를 해야 하겠다.
REFERENCES
1. Strupp M, Magnusson M. Acute unilateral vestibulopathy. Neurologic Clinics 2015;33:669-685.
2. Grad A, Baloh RW. Vertigo of vascular origin: clinical and electronystag- mographic features in 84 cases. Archives of Neurology 1989;46:281-284.
3. Duncan GW, Parker SW, Fisher CM. Acute cerebellar infarction in the PICA territory. Archives of Neurology 1975;32:364-368.
4. Lee H, Sohn SI, Cho YW, Lee SR, Ahn BH, Park BR, et al. Cerebellar in- farction presenting isolated vertigo frequency and vascular topographical patterns. Neurology 2006;67:1178-1183.
5. Kerber KA, Brown DL, Lisabeth LD, Smith MA, Morgenstern LB. Stroke among patients with dizziness, vertigo, and imbalance in the emergency department. Stroke 2006;37:2484-2487.
6. Kim HA, Lee H. Recent advances in central acute vestibular syndrome of a vascular cause. Journal of the Neurological Sciences 2012;321:17-22.
7. Saber Tehrani AS, Kattah JC, Mantokoudis G, Pala JH, Nair D, Blitz A, et al. Small strokes causing severe vertigo: frequency of false-negative MRIs and nonlacunar mechanisms. Neurology 2014;83:169-173.
8. Kattah JC, Talkad AV, Wang DZ, Hsieh YH, Newman-Toker DE. HINTS to diagnose stroke in the acute vestibular syndrome. Stroke 2009;40:3504- 3510.
9. Lee H, Kim HJ, Koo JW, Kim JS. Progression of acute cochleovestibulop- athy into anterior inferior cerebellar artery infarction. Journal of the Neu- rological Sciences 2009;278:119-122.
10. Oas JG, Baloh RW. Vertigo and the anterior inferior cerebellar artery syndrome. Neurology 1992;42:2274.
11. Kim J, Lopez I, DiPatre P, Liu F, Ishiyama A, Baloh R. Internal auditory artery infarction Clinicopathologic correlation. Neurology 1999;52:40.
12. Lee H. Audiovestibular loss in anterior inferior cerebellar artery territory infarction: a window to early detection? Journal of the Neurological Sci- ences 2012;313:153-159.
13. Kim JS, Cho KH, Lee H. Isolated labyrinthine infarction as a harbinger of anterior inferior cerebellar artery territory infarction with normal diffu- sion-weighted brain MRI. Journal of the Neurological Sciences 2009;278:
82-84.