VOL. 19, NO. 2, 2020 Case Report
CLINICAL PAIN
116
https://doi.org/10.35827/cp.2020.19.2.116
접수일 : 2020 년 3 월 27 일 , 게재승인일 : 2020 년 7 월 10 일 책임저자 : 김영삼 , 부산시 서구 대신공원로 26
뿸 49201, 동아대학교 의과대학 동아대학교병원 재활
의학과
Tel: 051-240-5690, Fax: 051-254-8511 E-mail: [email protected]
덱사메타손을 이용한 경추 7번 경막 외 스테로이드 주사 후 척수 경색
1
동아대학교 의과대학 동아대학교병원 재활의학과,
2메드윌 병원 재활의학과
이종화1ㆍ김영삼1ㆍ김상범1ㆍ이경우1ㆍ김영환2
Spinal Cord Infarction after C7 Transforaminal Epidural Steroid Injection Using Dexamethasone
Jong Hwa Lee, M.D.
1, Young Sam Kim, M.D.
1, Sang Beom Kim, M.D.
1, Kyeong Woo Lee, M.D.
1and Young Hwan Kim, M.D.
21
Department of Physical Medicine and Rehabilitation, Dong-A University College of Medicine,
2
Department of Physical Medicine and Rehabilitation, Medwill Hospital, Busan, Korea
Cervical transforaminal epidural steroid injection (TFESI) is commonly performed to provide relief of pain caused by radiculopathy. Intra-arterial injection of particulate steroid or direct needle injury can lead to spinal artery embolism or thrombosis.
Also there is a possibility of vascular spasm. To our knowledge, this is the first reported case of spinal cord infarction that occurred after TFESI with non-particulate steroid in Korea. A 47-year-old female patient underwent C7 TFESI at local pain clinic. Injected materials were dexamethasone and mepivacaine. Right after the intervention, she felt muscle weakness and decreased sensation. On physical examination, she had decreased sensation from C4 to T2 dermatome in light touch and pin-prick test. Proprioception and vibration were intact. The motor grades of upper extremities were grade 1. Cervical and thoracic spine MRI was checked. Diffusion-weighted image and apparent diffusion coefficient image showed long extension of spinal cord infarction from C2 to T1 level. (Clinical Pain 2020;19:116-119)
Key Words: Spinal cord infarction, Non-particulate steroids, Transforaminal epidural steroid injection
INTRODUCTION
Cervical transforaminal epidural steroid injection (TFESI) is commonly performed to provide symptomatic relief of pain caused by radiculopathy.
1This procedure allows direct therapeutic benefit of injected corticosteroids to the nerve root and enables suppression of the inflammatory response surrounding the targeted area.
2The reported incidence of significant complications is low, and complications include dural puncture, trauma to the spinal nerve, infection, vasovagal reaction, and allergic and anaphylactic reaction to the medication. Also, there is a possibility of vascular spasm. There were largely based
on case reports of TFESI performed with particulate steroids.
3To our knowledge, this is the first reported case of spinal cord infarction that occurred after TFESI with non-partic- ulate steroid in Korea.
CASE REPORT
A 47-year-old female patient with 6-month history of right upper arm pain visited local pain clinic. She was diag- nosed as C7 radiculopathy by electrodiagnostic study. She had no past medical history like DM, HTN or allergy reaction.
The patient underwent C7 TFESI. Fluoroscopy was uti- lized to guide needle into the foramina. Injected materials were 6 mg of dexamethasone and 5 ml of 2% mepivacaine.
Right after the intervention, she felt weakness and de-
creased sensation in whole body and mild respiratory
difficulty. At the time of onset, vital signs such as blood
pressure and respiratory rate were normal. Cervical spine
magnetic resonance image (MRI) was checked and it
이종화 외 4인: 덱사메타손을 이용한 경추 7번 경막 외 스테로이드 주사 후 척수 경색
CLINICAL PAIN 117 Fig. 1. Cervical MRI was taken about an hour after the symptom
onset. (A) T2-weighted image and (B) diffusion-weighted image showed no signal change throughout the cervical spinal cord.
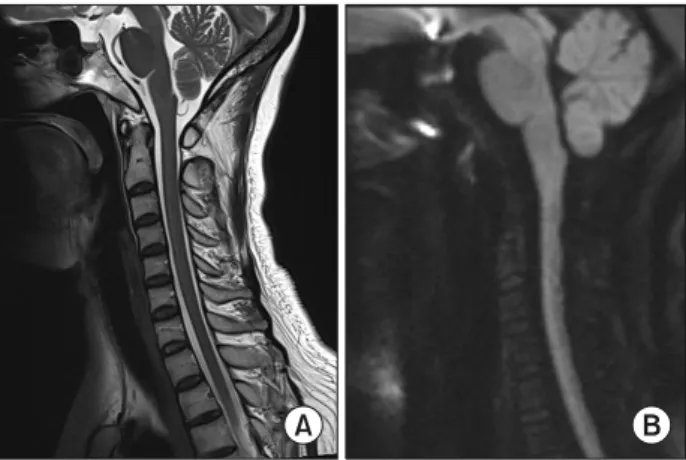
Fig. 2. Cervical MRI was taken 5 days after the symptom onset. Cervical and thoracic MRI showed spinal cord lesions compatible with spinal cord infarction. (A) In sagittal view, T2-weighted high signal intensity in spinal cord showed from C2 to T1 (arrows).
(B) In axial view, T2-weighted high signal intensity in spinal cord showed in bilateral areas on C4 level (arrows). (C) Diffusion-weighted image and (D) apparent diffusion coefficient image showed long extension of spinal cord infarction from C2 to T1 level (arrows).
showed no signal change in spinal cord (Fig. 1). After 10 hours from the onset of the symptoms, the weakness of lower extremities and respiratory difficulty disappeared.
But, the patient continued to complain of weakness in both upper extremities and decreased sensation on both whole arm. On physical examination, she had decreased sensation from C4 to T2 dermatomes in light touch and pin-prick test in both upper extremities. Proprioception and vibration were intact. The motor grades of upper extremities were grade 1 at C5∼T1 myotomes. A digital rectal examination revealed slightly decreased deep anal pressure and anal tone. No specific findings were observed in the blood test
and spinal tapping test.
Cervical and thoracic spine MRI was checked again to identify lesions in spinal cord after 5 days of symptom onset. High signal intensity was noted from C2 to T1 level in T2-weighted image, which was compatible with spinal cord infarction (Fig. 2). Diffusion-weighted image and ap- parent diffusion coefficient image showed long extension of spinal cord infarction from C2 to T1 level (Fig. 2).
When the patient was referred to rehabilitation unit after 5 days of symptom onset, activity of daily living was im- possible with upper extremities. She could stand and walk on even surface under supervision. But, she needed help in changing her posture. Bladder and bowel function was normal. Her Korean version of the Modified Barthel Index (K-MBI) score was 44 points.
Rehabilitation therapy was performed with ROM ex- ercise, therapeutic electrical stimulation, occupational ther- apy for daily activities, matt exercises for body balance.
Aspirin and atrovastatin were administered for secondary prevention of spinal infarction.
After six months, recovery of muscle weakness was
observed. The motor grades of both elbow flexor, wrist ex-
tensor and elbow extensor improved to Grade 3. But, both
finger flexors, finger abductors were still grade 1. She
needed moderate assistance for the activities such as wash-
ing, toileting, bathing and clothing due to poor strength of
distal parts of upper extremities. K-MBI score improved to
60 points.
VOL. 19, NO. 2, 2020
CLINICAL PAIN
118
DISCUSSION
TFESI is commonly performed in the nonsurgical treat- ment of lumbosacral radiculopathy.
3The transforaminal ap- proach allows concentrated delivery of medications to tar- geted neural foramen. The beneficial effect of TFESI has been proven by multiple study.
1However, although the in- cidence of complications of TFESI is relatively low, it can be accompanied by serious complication such as spinal cord infarction. The exact mechanism for this has not been revealed.
Most TFESI complications which have historically been revealed in case reports are related to particulate steroids.
As seen in this present case report, the drug used in this patient was not particulate steroid. Prior the most suggested mechanism of the ischemic complications of the central nervous system is embolus caused by intra-vascular in- jection of particulate corticosteroid.
4Particulate cortico- steroids are usually poorly soluble in water, thus they might precipitate out of a solution and crystallize within a hydro- philic environment. Most of the particles cover a size range between 0.5 and 100 μm, however sporadic particles even exceed a size of more than 1,000 μm.
5In contrast, Non-particulate steroids like dexamethasone sodium phos- phate are sporadic and small particles might be seen under the microscope with a typical particle size of 0.5 μm.
5Compared with the particulate steroid solutions, dex- amethasone sodium phosphate had particles that were sig- nificantly smaller than red blood cells, had the least ten- dency to aggregation, and had the lowest density.
6Given these properties of dexamethasone particles, therefore, there must be independent mechanisms of spinal cord in- farction aside from injectate aggregation and embolization.
Another hypothesis has been considered needle-induced vasospasm.
7Several studies have issued the potential of mechanical stimuli to cause vasoconstriction.
8In a pro- spective study of 504 cervical TFESI, it demonstrates that fluoroscopically confirmed venous or arterial intravascular contrast injections during TFESI occur 19.4% of the time.
9As a result, it can be inferred that there would be more mechanical stimuli causing vasospasm. Generally, Vaso- constriction was a focal effect affecting at the site in few minutes. However, when the vessels was puncture, it is af- fected not only by punctured area but also by a consid- erable distance on either side of it.
10In animal studies with
monkeys, it was confirmed that immediate intense vaso- spasm occurs when the cerebral blood vessels are punctured. This affected decrease of distal perfusion, which lasted from 4 hours up to 4 days.
8These results suggest that needle induced vasospasm could be a potential etiol- ogy of spinal cord infarction.
We suggest that this infarction was the result of an im- paired perfusion of the major feeding anterior radicular ar- tery, which supplying anterior spinal artery. It is assumed that hypoperfusion of the sulcal artery, which is relatively vulnerable to infarction, has occurred. When the patient’s clinical features and imaging are correlated, the mechanism can be suggested as above. However, The exact cause of this perfusion problem remains unclear.
According to our own knowledge, this is the first case report of spinal cord infarction following cervical TFESI using dexamethasone in Korea. According to announce- ment of the FDA, “The FDA is warning that injection of corticosteroids into the epidural space of the spine may re- sult in rare but serious adverse events, including loss of vi- sion, stroke, paralysis, and death”. This suggests that there may still be damage caused by various mechanisms regard- less of steroid type in epidural steroid injection.
Although the incidence of serious complications caused by non-particulated steroid is rare, practitioners who per- form TFESI should be aware of the potentially devastating complication like spinal cord infarction. Therefore, a care- ful caution is needed for this procedure. To reduce this po- tential damage risk, the use of Whitacre needles, blunt tip needles, and interlaminar procedures may be safer than transforaminal procedure in vascular damage. In addition, injecting an inferior and posterior approach during trans- foraminal approach could reduce the possibility of damag- ing the radicular artery.
REFERENCES
1. Bush K, Hillier S. Outcome of cervical radiculopathy treated with periradicular/epidural corticosteroid injections: a pro- spective study with independent clinical review. Eur Spine J 1996; 5: 319-325
2. Molloy RE, Benzon HT. Interlaminar epidural steroid in- jections for lumbosacral radiculopathy. In: Benzon HT, Raja SN, Molloy RE, Liu SS, Fishman SM, editors: Essentials of Pain Medicine and Regional Anesthesia, 2nd ed, Philadelphia:
Churchill Livingstone, 2005, 331-340
이종화 외 4인: 덱사메타손을 이용한 경추 7번 경막 외 스테로이드 주사 후 척수 경색