문맥염: 충수염의 합병증으로 발생한 증례 보고와 국내에서 보고 된 증례 고찰
황미원, 김백남
인제대학교 의과대학 상계백병원 내과학교실
Submitted: February 4, 2010 Revised: April 23, 2010 Accepted: April 23, 2010
Corresponding author: Baek-Nam Kim, M.D.
Department of Internal Medicine, Inje University Sanggye- Paik Hospital, Nowon-gu, Seoul 139-707, Korea
Tel: +82-2-950-8863, Fax: +82-2-950-1955 E-mail: [email protected]
Copyright © 2010 by The Korean Society of Infectious Diseases | Korean Society for Chemotherapy
Infect Chemother 2010;42(3):203-207
www.icjournal.org
Pylephlebitis: Report of a Case Secondary to Appendi- citis and Review of Cases Reported in Korea
Pylephlebitis occurs secondary to infection in the region drained by the portal venous system. We described a case of pylephlebitis which developed as a complication of appendicitis and reviewed 22 cases of pylephlebitis, including the current case, reported in Korea. Appendicitis, followed by diverticulitis, was the most common infection associated with pylephlebitis. Fever and abdominal pain were the most common presenting symptoms. Bacteremia was present in 60%
of cases. Streptococci, enteric gram-negative bacilli, and Bacteroides fragilis were common organisms isolated from the blood. Liver abscess was identified in 3 cases.
All patients survived regardless of anticoagulation therapy. Although pylephlebitis is a rare disease, it should be included in the differential diagnosis in patients with fever of unknown origin who present with nonspecific abdominal symptoms or abnormal liver function test.
Key Words: Thrombophlebitis, Portal vein, Mesenteric veins, Appendicitis,
DiverticulitisMee Won Hwang and Baek-Nam Kim
Department of Internal Medicine, Inje University College of Medicine, Seoul, Korea
서론
문맥염은 간문맥과 그 분지에 생기는 패혈성 혈전정맥염으로, 보통 간문맥계로 배 액되는 곳이나 간문맥에 인접한 부위(예: 총담관)의 화농성 병변에 의해 발생한다(1, 2). 원인이 밝혀지지 않는 경우도 있지만, 급성 대장 게실염이 문맥염의 가장 흔한 원인 이며 그 외에도 충수염, 염증성장질환, 회장 게실염, 화농성 췌장염, 장천공, 골반감염 등도 문맥염의 원발병소가 된다(3). 문맥염으로 인한 사망률은 11-32% (1980년대는 80%까지)로 보고되었다(1, 4, 5). 문맥염은 드문 질환이나, 복부 질환을 감별하기 위하 여 흔히 전산단층촬영이나 초음파를 이용함에 따라 국내에서도 1999년부터 문맥염 의 증례 보고가 늘고 있다(6). 저자들은 급성 충수염 치료로 충수절제술을 받은 환자 에서 발생한 문맥염 1예를 보고하며, 문헌 조사를 통하여 국내에서 발생한 문맥염 증례 를 정리하여 외국보고와 비교하였다.
증례
60세 남자가 7일 전부터 시작된 발열, 오한, 명치부위 불편감과 식욕 부진으로 입원하였다. 이 환자는 27일 전 충수염으로 복강경 충수절 제술을 받았으며, 위와 같은 증상이 생겨 1차 의료기관에서 감기로 5 일 동안 치료받았으나 호전되지 않았다. 다른 장기와 관련된 증상은 호 소하지 않았다. 7년 전에 당뇨병을 진단받고 경구혈당강하제를 복용 중 이었다. 입원 당시 혈압은 140/90 mmHg, 맥박수는 94회/분, 호흡수 는 20회/분, 체온은 39.2℃이었다. 배에 압통은 없었고 Murphy징후는 음성이었으며 간비종대도 없었다. 말초혈액에서 백혈구 수는 16,850/
mm3 (다핵구 86.3%), 혈색소는 11.3 g/dL, 혈소판은 191,000/mm3이 었다. 간기능검사는 아스파라진산 아미노전이효소가 35 U/L, 알라닌 아미노전이효소는 50 U/L, 총 빌리루빈은 1.0 mg/dL, 알칼리인산분 해효소는 77 IU/L, 총 단백은 6.0 g/dL, 알부민은 3.4 g/dL이었다. C- 반응성 단백질은 14.8 mg/L이었다. 요검사에서 단백은 ±, 당은 +++
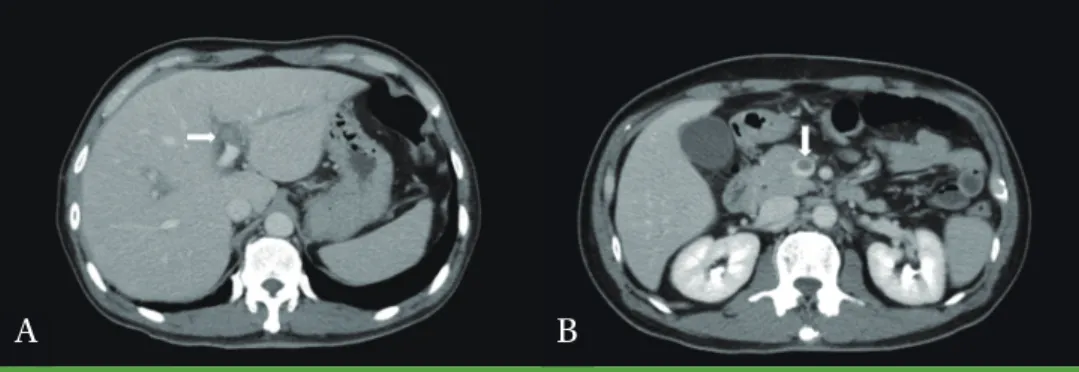
이었다. 복부 전산단층촬영에서 수술부위는 이상이 없었으나 오른쪽 문맥과 상장간막정맥에서 혈전(Fig. 1)이 관찰되어 문맥염으로 진단 하였다. 입원 당일부터 ceftriaxone을 경험적으로 정맥투여하였으나 입원 4일째 혈액배양에서 Klebsiella pneumoniae (ampicillin 내성;
ampicillin-sulbactam, cefazolin, cefoxitin, cefotaxime, imipenem, gentamicin, ciprofloxacin 감수성)가 동정되어 경구 ciprofloxacin 으로 교체하였다. 입원 5일째 발열은 없어졌고 복부 불편감 등의 증상 도 호전되어 입원 7일째 퇴원하였다. 1개월 후 전산단층촬영 추적을 원 하지 않았으나 상태가 안정적이었고 남은 증상이 없어 ciprofloxacin 을 총 30일 투여하고 치료를 종결하였다.
국내문헌 고찰
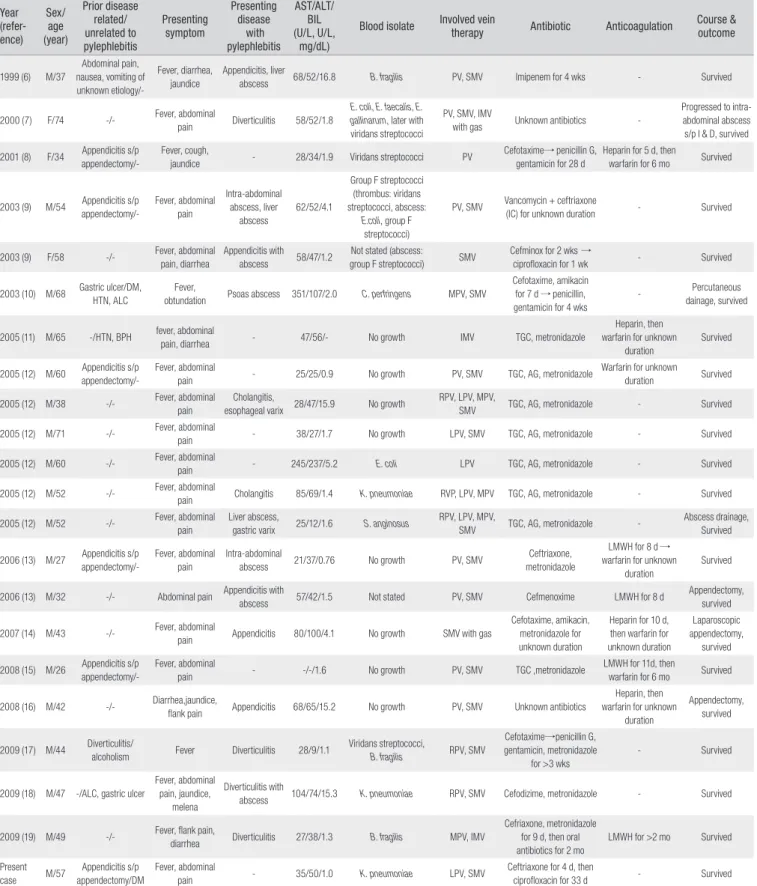
KoreaMed, KMbase, PubMed 등의 문헌데이터베이스를 pylephlebitis, thrombophlebitis, portal vein, mesenteric vein 등의 용어로 검색한 결과, 1999년부터 현재까지 이 증례를 포함하여 22예 가 국내에서 보고되었다(Table 1) (6-19). 19명(86.4%)이 남자였고 평 균 나이는 47.6세(범위 26-74세)이었다. 문맥염 유발과 상관 있을 것으 로 추정되는 선행 복부질환이 9명(40.9%)에서 있었는데, 충수염이 6예
로 가장 많았으며 모두 충수절제술을 받은 상태였다. 나머지는 게실염 과 원인이 불분명한 복통, 위궤양(저자들은 연관 있다고 하였음) 등이 었다. 22명 중 3명은 알코올간경화가 있거나 알코올중독자이었다. 2명 을 제외한 모든 환자(90.9%)에서 발열이 있었으며, 18명(81.8%)은 배 나 옆구리에 통증이나 불편감을 호소하였다. 5명(22.7%)은 설사를 동 반하였으며 4명(18.2%)은 황달을 호소하였다. 간효소(아스파라진산 아미노전이효소 또는 알라닌 아미노전이효소 >50 U/L) 치와 총 빌리루 빈(>1.5 mg/dL) 치 이상은 각각 15명(21명만 검사하여 71.4%)에서 관 찰되었다. 15명(68.2%)이 문맥염과 함께 복강내 감염질환도 발병하였 는데, 충수염(충수고름집 혹은 충수절제술 후 수술부위 고름집)이 7예 (31.8%)로 가장 흔하였고 나머지는 게실염(4예), 담도염(2예), 간농양 (1예-2예가 더 있으나 다른 감염과 동반됨)과 허리근고름집(1예) 등이 었다. 다른 복강내감염질환은 없고 문맥염만 발견된 증례는 7건 이었 다. 두 명에서 내시경으로 식도나 위에서 정맥류가 확인되었는데 추적 검사에서 모두 사라졌다.
복부 전산단층촬영 또는 초음파 검사로 혈전은 문맥과 장간막정맥 (16명), 문맥(3명), 상장간막정맥염(2명), 하장간막정맥(1명)에서 발견 되었다. 장간막경색은 아무도 관찰되지 않았다. 2명에서는 정맥 안에 서 공기가 관찰되었다. 혈액배양검사 결과는 20명에서 기술되었는데, 12명(60.0%)이 배양양성이었으며 2예는 여러균 감염이었다. 균종으로 는 사슬알균이 가장 흔하여 5명에서 분리되었으며, K. pneumoniae 와 Bacteroides fragilis가 각각 3명에서, 대장균이 2명에서, 장알균과 Clostridium perfringens이 각각 1명에서 배양되었다. 항생제 이름과 투여기간을 정확히 파악하기 어려우나, 항생제는 대부분 2주 이상 투 여되었다. 9명 환자에게 8일에서 6개월 동안 heparin이나 warfarin이 투여되었다. 추적 방사선촬영은 19명(전산단층촬영 17명, 초음파 2명) 에서 진단 후 2주에서 20개월 사이 시행되었는데, 4명은 혈전증이 완전 히 없어졌고 나머지 환자에서는 일부 남아있거나 변화가 없었다. 우리 나라에서 보고된 문맥염 환자 중 사망한 경우는 없었다.
고찰
문맥염은 복강내감염질환의 합병증이며, 복강내질환은 어느 위치 든 문맥염의 원인이 된다(5). 충수염이 문맥염의 가장 흔한 원인으로 알
A B
Figure 1. Enhanced computed tomography of abdomen and pelvis shows (A) thrombosis of left portal vein (arrow) and (B)
a thrombus in the lumen of the superior mesenteric vein (arrow) on venous phase.Table 1. Summary of 22 Cases of Pylephlebitis Reported in Korea Year
(refer- ence)
Sex/
(year) age
Prior disease related/
unrelated to pylephlebitis
Presenting symptom
Presenting disease
with pylephlebitis
AST/ALT/
BIL (U/L, U/L,
mg/dL)
Blood isolate Involved vein
therapy Antibiotic Anticoagulation Course &
outcome
1999 (6) M/37Abdominal pain, nausea, vomiting of unknown etiology/-
Fever, diarrhea, jaundice
Appendicitis, liver
abscess 68/52/16.8 B. fragilis PV, SMV Imipenem for 4 wks - Survived
2000 (7) F/74 -/- Fever, abdominal
pain Diverticulitis 58/52/1.8
E. coli, E. faecalis, E.
gallinarum, later with viridans streptococci
PV, SMV, IMV
with gas Unknown antibiotics -
Progressed to intra- abdominal abscess s/p I & D, survived 2001 (8) F/34 Appendicitis s/p
appendectomy/-
Fever, cough,
jaundice - 28/34/1.9 Viridans streptococci PV Cefotaxime→ penicillin G,
gentamicin for 28 d
Heparin for 5 d, then
warfarin for 6 mo Survived
2003 (9) M/54 Appendicitis s/p appendectomy/-
Fever, abdominal pain
Intra-abdominal abscess, liver
abscess
62/52/4.1
Group F streptococci (thrombus: viridans streptococci, abscess:
E.coli, group F streptococci)
PV, SMV Vancomycin + ceftriaxone
(IC) for unknown duration - Survived
2003 (9) F/58 -/- Fever, abdominal
pain, diarrhea
Appendicitis with
abscess 58/47/1.2 Not stated (abscess:
group F streptococci) SMV Cefminox for 2 wks →
ciprofloxacin for 1 wk - Survived
2003 (10) M/68 Gastric ulcer/DM, HTN, ALC
Fever,
obtundation Psoas abscess 351/107/2.0 C. perfringens MPV, SMV
Cefotaxime, amikacin for 7 d → penicillin, gentamicin for 4 wks
- Percutaneous
dainage, survived
2005 (11) M/65 -/HTN, BPH fever, abdominal
pain, diarrhea - 47/56/- No growth IMV TGC, metronidazole
Heparin, then warfarin for unknown
duration
Survived
2005 (12) M/60 Appendicitis s/p appendectomy/-
Fever, abdominal
pain - 25/25/0.9 No growth PV, SMV TGC, AG, metronidazole Warfarin for unknown
duration Survived
2005 (12) M/38 -/- Fever, abdominal
pain
Cholangitis,
esophageal varix 28/47/15.9 No growth RPV, LPV, MPV,
SMV TGC, AG, metronidazole - Survived
2005 (12) M/71 -/- Fever, abdominal
pain - 38/27/1.7 No growth LPV, SMV TGC, AG, metronidazole - Survived
2005 (12) M/60 -/- Fever, abdominal
pain - 245/237/5.2 E. coli LPV TGC, AG, metronidazole - Survived
2005 (12) M/52 -/- Fever, abdominal
pain Cholangitis 85/69/1.4 K. pneumoniae RVP, LPV, MPV TGC, AG, metronidazole - Survived
2005 (12) M/52 -/- Fever, abdominal
pain
Liver abscess,
gastric varix 25/12/1.6 S. anginosus RPV, LPV, MPV,
SMV TGC, AG, metronidazole - Abscess drainage,
Survived
2006 (13) M/27 Appendicitis s/p appendectomy/-
Fever, abdominal pain
Intra-abdominal
abscess 21/37/0.76 No growth PV, SMV Ceftriaxone,
metronidazole
LMWH for 8 d → warfarin for unknown
duration
Survived
2006 (13) M/32 -/- Abdominal pain Appendicitis with
abscess 57/42/1.5 Not stated PV, SMV Cefmenoxime LMWH for 8 d Appendectomy,
survived
2007 (14) M/43 -/- Fever, abdominal
pain Appendicitis 80/100/4.1 No growth SMV with gas
Cefotaxime, amikacin, metronidazole for unknown duration
Heparin for 10 d, then warfarin for unknown duration
Laparoscopic appendectomy,
survived 2008 (15) M/26 Appendicitis s/p
appendectomy/-
Fever, abdominal
pain - -/-/1.6 No growth PV, SMV TGC ,metronidazole LMWH for 11d, then
warfarin for 6 mo Survived
2008 (16) M/42 -/- Diarrhea,jaundice,
flank pain Appendicitis 68/65/15.2 No growth PV, SMV Unknown antibiotics
Heparin, then warfarin for unknown
duration
Appendectomy, survived
2009 (17) M/44 Diverticulitis/
alcoholism Fever Diverticulitis 28/9/1.1 Viridans streptococci,
B. fragilis RPV, SMV
Cefotaxime→penicillin G, gentamicin, metronidazole
for >3 wks
- Survived
2009 (18) M/47 -/ALC, gastric ulcer
Fever, abdominal pain, jaundice,
melena
Diverticulitis with
abscess 104/74/15.3 K. pneumoniae RPV, SMV Cefodizime, metronidazole - Survived
2009 (19) M/49 -/- Fever, flank pain,
diarrhea Diverticulitis 27/38/1.3 B. fragilis MPV, IMV
Cefriaxone, metronidazole for 9 d, then oral antibiotics for 2 mo
LMWH for >2 mo Survived
Present
case M/57 Appendicitis s/p appendectomy/DM
Fever, abdominal
pain - 35/50/1.0 K. pneumoniae LPV, SMV Ceftriaxone for 4 d, then
ciprofloxacin for 33 d - Survived
AG, aminoglycoside; ALC, alcoholic liver cirrhosis; ALT, alanine aminotransferase; AST, aspartate aminotransferase; BIL, total bilirubin; BPH, benign prostate hypertrophy; d, day; DM, diabetes mellitus; HTN, hypertension; IC, intracatheter administration; I & D, incision and drainage; IMV, inferior mesenteric vein; LMWH, low molecular weight heparin; LPV, left portal vein; MPV, main portal vein; mo, month; PV, portal vein; RPV, right portal vein; SMV, superior mesenteric vein; s/p, status post; TGC, third-generation cephalosporin; wk, week
려졌으나 충수염에 따른 문맥염은 갈수록 감소하고 있다(5). 문맥염의 원인질환은 외국보고에 의하면 63.2% (12/19명)에서 복강내감염질환 으로 밝혀졌는데(1), 우리나라는 81.8% (18/22명)에서 복강내감염질 환이 문맥염에 선행하거나 동반되었다(Table 2). 1979-1995년 미국에 서 보고된 증례 고찰에 의하면 게실염이 가장 흔한 원인이었다(1). 비슷 한 시기 다른 병원에서는 문맥염의 원인으로 담낭염과 다음으로 게실 염이 흔한 원인질환이었다(5). 외국과 달리 우리나라에서는 아직도 충 수염이 문맥염과 가장 많이 연관된 감염질환이었으며 게실염은 그 다 음이었다. 이와 같은 복강내 감염질환뿐 만 아니라 과응고상태(암이나 응고인자 결핍)이나 간문맥 유량을 감소시키는 질환(간경화, 간담도 악 성종양)도 문맥염 발생을 촉진한다(5). 그 외 염증성 장질환(20), 괴사 성 또는 화농성 췌장염(21), 장천공(22), 감염성 총담관결석증(23), 베 체트병(24), 아메바큰창자염(5), 위궤양(10, 25), 치핵(26) 등 다양한 질 환이 문맥염을 유발하거나 촉진한다고 보고되었다.
문맥염은 발열, 오한, 다양한 양상의 복통, 식욕부진과 체중감소 등 비특이적인 증상으로 나타난다. Plemmons 등의 보고에 의하면 발열 은 100%에서 복통은 74%에서 나타났다(1). Baril 등의 보고에서는 모 든 문맥염 환자가 발열과 복통을 호소하였다(5). 우리나라 환자는 발 열(90.9%)과 복통(81.8%)이 흔한 증상이었다(Table 1). 따라서 복강 내 감염과 동반되어 불명열이 있거나 원인을 알 수 없는 복통이 발열과 함께 지속될 때 감별진단에 문맥염도 염두에 두어야 한다.
감염된 혈전은 문맥계에서 간으로 떨어지면 간농양을 일으킨다(27).
국내 환자에서는 13.6%에서 간농양이 동반되었으나 외국보고에 의하 면 52.6%에서 발견되었다(1). 앞의 연구자들은 간농양을 동반한 문맥 염의 경우 증상 발현 5일 이후에 황달이 생기는데 비해, 담도염에 의한 문맥염은 질환 초기부터 황달이 있어 구분이 된다고 주장하였다(1). 그 러나 국내보고에서는 증상보유기간이 명확하게 기술되지 않아 이를 확 인하기 어려웠다(6, 9, 12). 복강내감염이 있는 환자에서 그것으로는 설 명되지 않는 황달이 있다면 문맥염 동반 여부를 확인할 필요가 있다.
문맥염 환자에서 혈액배양은 국내는 60.0% 외국에서는 22.7-88.2
% 양성이었다(1, 5). 여러균 감염이 외국에서는 88%인데(1) 비하여 우 리나라에서는 16.7% (2/12명)에 불과하였다. 혈액배양균은 비율에 조 금 차이가 나나 그 종류는 국내보고와 외국보고가 비슷하였다(Table 2). 우리나라에서는 사슬알균이 가장 흔히 배양되었으며 나머지는 장 내 그람음성막대균과 혐기균이었다. 1995년 19예를 종합한 보고에서 는 Bacteroides와 대장균이 가장 흔히 분리되었다(1). 이런 자료를 바 탕으로 문맥염의 경험적 치료에 장내 그람음성막대균, 사슬알균, 혐기 균 등을 표적으로 하는 항생제를 선택하는 것이 권장된다(28). 초기 경 험적 항생제 치료는 배양검사와 항생제감수성검사 결과에 따라 나중 에 수정해야 한다(28).
항생제 사용기간에 대하여 아직 정립된 바는 없으나 문맥염 합병증 으로 간농양이 흔하고 간농양 발생 단계에서는 전산단층촬영에 발견 되지 않을 수 있다는 점을 감안하여 최소 4주 사용이 권장되고 있다 (1). 만약 초기 전산단층촬영에서 간농양이 확인되면 최소 6주 항생제 치료가 권고된다(1). 직경 3 cm 이상의 간농양은 항생제 치료와 함께 경피적배액술이 필요하다(3). 우리나라에서 보고된 환자에서는 방사 선촬영 추적시기가 일정하지 않아 혈전 해소의 정확한 시기를 확인하 기 어려웠으나, 항생제 치료 4-6주가 지나면 문맥의 혈전은 해면성 변 형을 보이거나 완전히 없어진다(28).
문맥염 환자에서 혈전의 확산으로 인한 장허혈과 장경색 발생을 막 기 위하여 항응고요법이 시도되었으나, 아직까지 문맥염에서 항응고요 법에 대한 확실한 근거는 없다(28). Plemmons 등에 의하면 heparin 투여와 상관 없이 항생제 치료만으로도 대부분 회복되어, heparin이 문맥염의 치료에 꼭 필요한 약제는 아님이 알려졌다(1). Baril 등은 암이 나 응고인자 결핍에 의한 과다응고 상태에서는 문맥염 재발률이 높으 므로 항응고요법이 필요하다고 하였다(5). 응고장애가 없고 혈전이 문 맥에만 국한된 경우 항응고요법이 필요없으나, 장간맥정맥이 침범된 경 우는 장허혈과 경색의 위험이 높아질 수 있으므로 항응고요법이 도움 이 될 수 있다고 주장하였다(5).
요약하면, 우리나라에서 보고된 문맥염은 충수염과 가장 흔히 관련
Table 2. Comparison of Korean and Other Cases
Korean cases (1999-present)
(6-19) Plemmons et al. (1979-1995)
(1) Baril et al. (1993-1995)
(5)
Study patient 22 19 44
Intra-abdominal infection related to pylephlebitis 18 (81.8%) 12 (63.2%) 29 (65.9%)
Appendicitis/abscess
Diverticulitis 11 4 5
Biliary tract infection 4 6 7
Colon injury or perforation 2 - 10
Others - - 6
Presence of liver abscess 1 2 1
Positive blood culture 3 (13.6%) 10 (52.6%) 3 (6.8%)
Polymicrobial on blood culture 12/20 (60.0%) 15/17 (88.2%) 10/44 (22.7%)
Patient whose blood the following organism was isolated in: 2 (16.7%) 8/17 (47.1%) 4/10 (40.0%)
Streptococcus species
5 5 2*
Enteric gram-negative bacilli 5 8 3*
Bacteroides species 3 9 1*
* Polymicrobial culture results have been excluded since the species were not stated.
있고, 사슬알균, 장내 그람음성막대균, 혐기균 등의 장내세균이 주요 원인균이었으며, 항응고제 투여와 상관 없이 항생제 치료로 모두 치유 되었다. 문맥염은 흔하지 않지만 불명열 환자에서 비특이적인 복부 증 상이나 설명되지 않는 간효소 수치의 상승 등이 있을 때 감별진단에 고 려할 질환이다.
References
1. Plemmons RM, Dooley DP, Longfield RN. Septic thrombo
phlebitis of the portal vein (pylephlebitis): diagnosis and mana
gement in the modern era. Clin Infect Dis 1995;21:111420.
2. Kasper DL, Sahani D, Misdraji J. Case 252005 A 40year
old man with prolonged fever and weight loss. N Engl J Med 2005;353:71322.
3. Balthazar EJ, Gollapudi P. Septic thrombophlebitis of the mesenteric and portal veins: CT imaging. J Comput Assist Tomogr 2000;24:75560.
4. Witte CL, Brewer ML, Witte MH, Pond GB. Protean mani festations of pylethrombosis. A review of thirtyfour patients.
Ann Surg 1985;202:191202.
5. Baril N, Wren S, Radin R, Ralls P, Stain S. The role of anti
coagulation in pylephlebitis. Am J Surg 1996;172:44952.
6. Lim HE, Cheong HJ, Woo HJ, Kim WJ, Kim MJ, Lee CH, Park SC. Pylephlebitis associated with appendicitis. Korean J Intern Med 1999;14:736.
7. Lee JS, Hong CK, Kim KC, Hong SP, Hwang SG, Park PW, Rim KS, Kim JW, Kim HJ. A case of portal and mesenteric venous gas and thrombosis in sigmoid diverticulitis. Korean J Gastroenterol 2000;36:40812.
8. Kim JK, Hong SN, Yang BR, Park JH, Moung BH, Shin JH, Kim SJ, Shin DH. A case of septic portal vein thrombophlebitis:
presenting with fever of unknown origin. Korean J Infect Dis 2001;33:3469.
9. Hur H, Sung GY, Lee DS, Kim W, Park IY, Won JM. Pylephlebitis as a complication of acute appendicitis. J Korean Surg Soc 2003;64:1803.
10. Shin DH, Park JH, Yoon KW, Shin JH, Kim SJ. Clostridium perfringens septicemia with thrombophlebitis of the portal vein. J Infect 2003;46:2535.
11. Lee IK, Kim SA, Lee YS, Oh ST, Jeon HM, Kim EK, Chang SK, Jung SE. Thrombophlebitis of the inferior mesenteric vein. J Korean Soc Coloproctol 2005;21:32932.
12. Kim TD, Kim TN, Oh HJ, Kim JH, Lee HJ, Park WK, Jang JC. Clinical characteristics and radiologic findings of pylephlebitis. Korean J Med 2005;69 (Suppl 3):S798806.
13. Park MS, Choi JY, Lee SM, Hong SW. Portal pyelophlebitis asso
ciated with acute appendicitis. J Korean Surg Soc 2006;71:3047.
14. Kim BK, Lee SK. A case of thrombophlebitis in superior mesenteric vein due to appendicitis. Korean J Gastroenterol 2007;49:2679.
15. Chang YS, Min SY, Joo SH, Lee SH. Septic thrombophlebitis of the portomesenteric veins as a complication of acute appendicitis. World J Gastroenterol 2008;14:45802.
16. Kim SH, Hong ES, Kim WY, Ahn R, Hong JS. Acute appendicitis with superior mesenteric vein thrombosis and portal vein thrombosis. J Korean Soc Emerg Med 2008;19:1426.
17. Ku BH, Kim YS, Kim JH, Choi YK, Yeon JW, Lee SG, Kim SY.
A case of pylephlebitis with Streptococcus viridans and Bacteroides fragilis bacteremia secondary to diverticulitis.
Korean J Med 2009;76:6226.
18. Lee BK, Ryu HH. A case of pylephlebitis secondary to cecal diverticulitis. J Emerg Med 2009 [Epub ahead of print].
19. Jung HS, Shim KN, Jung JM, Kang MJ, Na YJ, Jung SA, Yoo K. A case of pylephlebitis of the inferior mesenteric vein and portal vein. Intest Res 2009;7:1059.
20. Aguas M, Bastida G, Nos P, Beltran B, Grueso JL, Grueso J.
Septic thrombophlebitis of the superior mesenteric vein and multiple liver abscesses in a patient with Crohn's disease at onset. BMC Gastroenterol 2007;7:22.
21. Nouira K, Bedioui H, Azaiez O, Belhiba H, Messaoud MB, Ksantini R, Jouini M, Menif E. Percutaneous drainage of suppurative pylephlebitis complicating acute pancreatitis.
Cardiovasc Intervent Radiol 2007;30:12424.
22. Peters TG, Locke JR, Weight GR. Suppurative pylephlebitis caused by toothpick perforation. South Med J 1988;81:4145.
23. Uzun GV, Gusarenko VD, Piskunova NV, Gerasimenko AI, Kurennaia SS. Suppurative pylephlebitis in suppurative cholecystitis and cholangitis. Klin Khir 1990:257.
24. Gelber AC, Schachna L, Mitchell L, Schwartzman G, Hartnell G, Geschwind JF. Behcet's disease complicated by pylephlebitis and hepatic abscesses. Clin Exp Rheumatol 2001;19 (Suppl 24):S5961.
25. Drabick JJ, Landry FJ. Suppurative pylephlebitis. South Med J 1991;84:13968.
26) Chau NG, Bhatia S, Raman M. Pylephlebitis and pyogenic liver abscesses: a complication of hemorrhoidal banding. Can J Gastroenterol 2007;21:6013.
27. Slovis TL, Haller JO, Cohen HL, Berdon WE, Watts FB Jr.
Complicated appendiceal inflammatory disease in children:
pylephlebitis and liver abscess. Radiology 1989;171:8235.
28. Chirinos JA, Garcia J, Alcaide ML, Toledo G, Baracco GJ, Lichtstein DM. Septic thrombophlebitis: diagnosis and management. Am J Cardiovasc Drugs 2006;6:914.