ABSTRACT
Merkel cell carcinoma (MCC) is an uncommon neuroendocrine cutaneous malignancy. The thyroid gland is an exceptionally rare site of metastasis for MCC. Thus, metastasis to the thyroid gland may entail diagnostic difficulties. An 82-year-old man presented with a palpable neck tumor in the right anterior neck. Computed tomography scan revealed a 3.4 cm, enhancing tumor in the right thyroid gland. The patient underwent fine needle aspiration, and cytologic and immunohistochemical findings revealed metastasis of MCC to thyroid gland. We decided to perform surgical excision of the right thyroid gland. The patient was discharged 2 days after surgery without any complications. Various immunohistochemical studies were performed with the surgical specimen. The tumor cells were positive for CK 20 and CD 56, but negative for thyroid transcription factor-1. Finally, the histopathologic diagnosis confirmed as metastasis of MCC to the thyroid gland. Here, we present an exceedingly rare metastasis of MCC to the thyroid gland and discuss its diagnosis and treatment. In patients with a known history of a primary malignancy, the differential diagnosis of any abnormal findings in the thyroid gland should always include possibility of potential metastasis.
Keywords: Thyroid gland; Merkel cell carcinoma; Metastasis
INTRODUCTION
Merkel cell carcinoma (MCC) is a highly aggressive and rare neuroendocrine malignancy arising from the skin. The tumor was first described in 1972 by Cyril Toker (1) as a variant of sweat gland carcinoma called trabecular cell carcinoma of the skin. MCC is an uncommon tumor, with its reported incidence of 0.6 per 100,000 person-years (2). It is predominantly seen in the elderly on the sun-exposed areas of the body (3,4). Some reports suggest
ultraviolet radiation as a risk factor, as most MCCs occur on sun-damaged skin (5,6). Another risk factor related to the pathogenesis of MCC is immune suppression. MCC is found to be more common among patients with human immunodeficiency virus, lymphoma, or leukemia (7-9).
MCC commonly presents with a nonspecific erythematous or violaceous firm nodule.
The most common clinical features of MCC have been summarized by the acronym AEIOU: 1) A for asymptomatic tenderness; 2) E for expanding rapidly (<3 months); 3) I for
Short Communication
Received: Feb 5, 2021 Revised: Feb 21, 2021 Accepted: Feb 22, 2021 Correspondence to Kwangsoon Kim
Department of Surgery, College of Medicine, The Catholic University of Korea, 222 Banpo- daero, Seocho-gu, Seoul 06591, Korea.
E-mail: [email protected]
Copyright © 2021. Korean Association of Thyroid and Endocrine Surgeons; KATES This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (https://
creativecommons.org/licenses/by-nc/4.0/).
ORCID iDs Kwangsoon Kim
https://orcid.org/0000-0001-6403-6035 Chan Kwon Jung
https://orcid.org/0000-0001-6843-3708 Ja Seong Bae
https://orcid.org/0000-0002-6271-2105 Jeong Soo Kim
https://orcid.org/0000-0002-9982-7838 Funding
This research was supported by Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Education (NRF- 2015R1D1A1A01058798).
Conflict of Interest
No potential conflict of interest relevant to this article was reported.
Author Contributions
Conceptualization: Kwangsoon Kim;
Investigation: Kwangsoon Kim, Chan Kwon Jung; Methodology: Kwangsoon Kim, Ja Seong
Kwangsoon Kim 1, Chan Kwon Jung 2, Ja Seong Bae 1, Jeong Soo Kim 1
1Department of Surgery, College of Medicine, The Catholic University of Korea, Seoul, Korea
2Department of Hospital Pathology, College of Medicine, The Catholic University of Korea, Seoul, Korea
Metastasis of Merkel Cell Carcinoma
to the Thyroid Gland: a Case Report
Bae; Project administration: Kwangsoon Kim;
Resources: Kwangsoon Kim, Chan Kwon Jung, Ja Seong Bae, Jeong Soo Kim; Supervision:
Chan Kwon Jung, Ja Seong Bae, Jeong Soo Kim; Validation: Kwangsoon Kim, Ja Seong Bae, Jeong Soo Kim; Visualization: Kwangsoon Kim, Chan Kwon Jung; Writing - original draft:
Kwangsoon Kim; Writing - review & editing:
Kwangsoon Kim, Chan Kwon Jung, Ja Seong Bae, Jeong Soo Kim.
immunosuppression; 4) O for older than age 50; and 5) U for ultraviolet-exposed sites. Up to 89% of patients with MCC met 3 or more of the AEIOU criteria (6).
The treatment modalities for MCC remains inconsistent and recommendations are not uniform.
Mainstay of treatment is multidisciplinary management with local excision, postoperative radiotherapy and adjuvant chemotherapy depending on the stage of the disease (10).
The head and neck are the most common site of occurrence, accounting for about 50% (11).
Majority of patients present with a localized skin tumor and clinically negative lymph nodes. At the time of diagnosis, 30% have metastatic disease in the skin, liver, bone, lung, brain or distant lymph nodes (12,13). However, the thyroid gland is a rare site of metastasis for MCC with only few cases published to date. Here, we report a case of metastatic MCC to the thyroid gland.
CASE REPORT
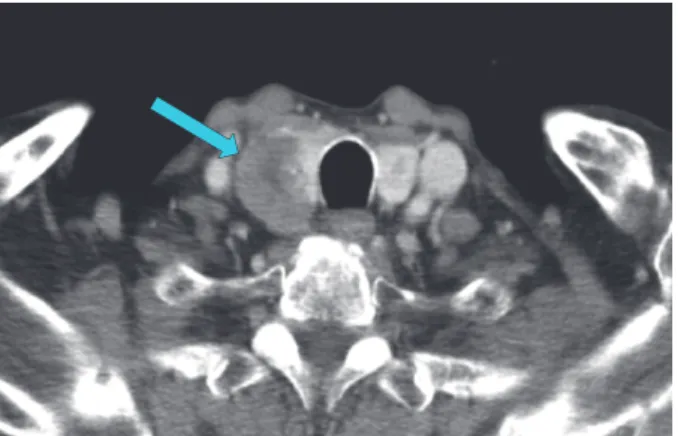
An 82-year-old man was referred to the division of thyroid and endocrine surgery with palpable neck tumor in the right anterior neck. The tumor had been detected 7 months before. Computed tomography (CT) scan revealed a 3.4 cm heterogenous enhancing tumor with calcification in right thyroid gland (Fig. 1), which indicated metastasis from MCC.
The patient initially presented with a 5 cm left axillary lesion for 2 months. Within the past month, the lesion rapidly grew to 10 cm. A needle biopsy was performed, and the tumor was diagnosed as MCC. This patient underwent wide excision of the left axillary region with axillary lymph node dissection due to MCC's high rate of metastasis to lymph nodes.
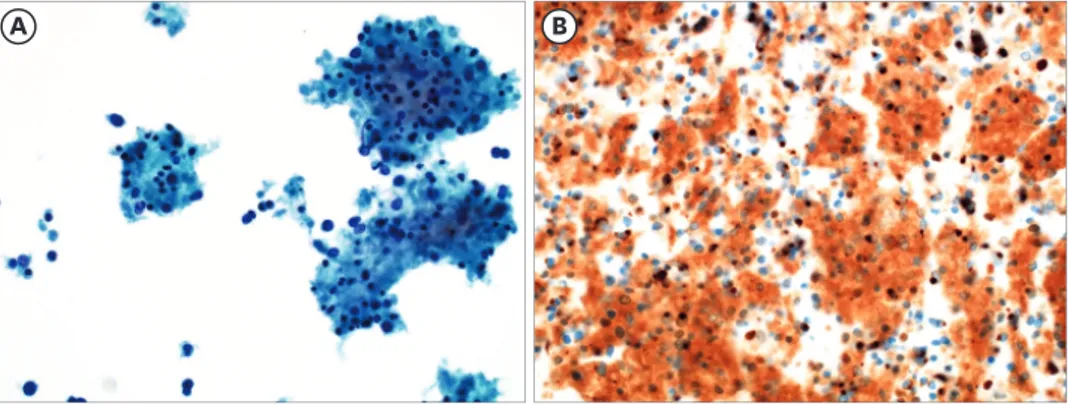
Afterwards, the patient was admitted to our department for further clinical evaluation and treatment. At initial sonographic examination, the tumor in his right anterior neck was microlobulated with microcalcification. Findings showed high suspicion for malignancy, such as anaplastic thyroid carcinoma. The patient underwent fine needle aspiration (FNA) of the largest tumor located in the right thyroid gland. Cytology features on FNA revealed irregular clusters of small to intermediate sized cells which showed monomorphous tumor cells with scant cytoplasm and round hyperchromatic nuclei with finely granular chromatin (Fig. 2A). Numerous mitosis and karyorrhectic nuclei were present. Immunohistochemical study was performed, and results were positive for CK 20 and CD 56. Immunostaining for CK
Fig. 1. Computed tomography scan revealed a 3.4 cm heterogenous enhancing tumor with calcification in right thyroid gland.
20 on cell block showed a paranuclear dotlike pattern (Fig. 2B). The patient was subsequently diagnosed as metastasis of MCC to the thyroid gland.
We decided to perform right hemithyroidectomy to resolve patient's symptoms. Intraoperative findings showed apparent extrathyroidal extension to the recurrent laryngeal nerve and strap muscles, but no enlarged lymph nodes. The patient had the recurrent laryngeal nerve cut off during operation, but was discharged the next day without any specific symptoms.
Histopathologic examination showed infiltration of the thyroid gland by MCC. The tumor consisted of small to intermediated sized cells with round nucleus, inconspicuous nucleoli and scant cytoplasm infiltrating the thyroid gland (Fig. 3A). Numerous mitoses and areas with necrosis were observed. Immunohistochemical studies were performed for synaptophysin, CD 56 (Fig. 3C), CK 20 (Fig. 3D), and thyroid transcription factor-1. The tumor cells were positive for synaptophysin (Fig. 3B), CD 56 (Fig. 3C) and CK 20 (Fig. 3D), but negative for thyroid transcription factor-1 (Fig. 3E) and calcitonin (Fig. 3F). These results finally confirmed the diagnosis of metastasis of MCC to the thyroid gland.
Adrenal metastasis was confirmed on abdominal CT 3 months after right hemithyroidectomy, and adrenalectomy was performed. The patient was referred to the department of
hematology and oncology for additional systemic treatment. However, the patient refused further treatment due to economic burden and old age.
DISCUSSION
Primary thyroid cancer is the most common endocrine malignancy, and its incidence accounts for 1%–1.5% of all cancers (14,15). Despite rich vascular supply of the thyroid gland, metastatic thyroid cancers are an exceptionally rare. Possible reason for such a low incidence of metastatic thyroid cancers, is abundant arterial supply which is associated high oxygen saturation and iodine content in the thyroid gland. This inhibits the growth of malignant cells in the thyroid gland (16,17). Clinical metastasis to the thyroid gland occurs less than 3%, but this number may increase in the future due to greater use of high-resolution ultrasonography and FNA (18,19). The most common cancers metastasizing to the thyroid gland are renal cell, lung, colorectal, breast, stomach, and melanoma (20,21). However, MCC is rare type of cancer to metastasize to the thyroid gland.
A B
Fig. 2. Fine needle aspiration cytology. (A) Liquid based cytology shows monomorphous tumor cells with scant cytoplasm and round hyperchromatic nuclei with finely granular chromatin (Papanicolaou stain, ×400). (B) Immunostain for CK 20 on cell block shows a paranuclear dotlike pattern of staining (×400).
MCC is a highly rare neuroendocrine malignancy of the skin, accounting for less than 1%
of skin cancers. It is a fast-growing tumor and commonly metastasizes to bone and lymph nodes (22). The protocol of treatment for MCC should be based on a multidisciplinary approach, including wide local excision, chemotherapy and radiotherapy (23). Surgical removal of the primary tumor is most important due to its aggressiveness. Postoperative radiation therapy is generally recommended for locoregional control (24). The role of chemotherapy remains controversial in patients with no metastatic disease, and although many chemotherapeutic regimens show positive results, survival benefit has not been conclusively demonstrated (24). MCC shows an aggressive clinical course and local recurrence and distant metastasis are common. Overall survival at 5 years is approximately 51% for local disease, 35% for nodal disease, and 14% for distant disease (25).
Metastasis of MCC to the thyroid gland is an exceptionally rare clinical finding. Only 3 other cases have been described in literature (4,26). Primary diagnostic method for metastatic thyroid cancers is FNA cytology (27). Classic cytologic features of MCC are small to intermediate cells with scant cytoplasm, large round-to-oval nuclei with homogenous chromatic pattern, no nuclear infoldings or indentations, and several mitoses (4). For further evaluation of thyroid lesions, magnetic resonance imaging, CT, or positron emission tomography/CT can be used to distinguish malignancy from benign tumors (24).
Immunohistochemistry is essential to differentiate MCC from other malignancies (28). The tumor expresses CK 30, neuroendocrine markers (chromogranin A, CD 56), neurofilament, and thyroid transcription factor-1. Staining results for MCC is positive for CK 20 and neurofilament and negative for thyroid transcription factor-1. Small cell lung carcinoma must be differentiated from MCC, and using a panel of immunohistochemistry markers can be helpful. Especially, immunohistochemical stains for CK 20, neurofilament, and
A B C
D E F
Fig. 3. Metastatic Merkel cell carcinoma in the thyroid gland. (A) Low-power view of hematoxylin-eosin stained showing features of small round tumor infiltrating the thyroid gland (×100). Tumor cells are positive for (B) synaptophysin, (C) CD 56, and (D) CK 20, and negative for (E) thyroid transcription factor-1 and (F) calcitonin (×100).
thyroid transcription factor-1 are useful markers for differentiation of MCC from lung small cell carcinoma (29). MCC is positive for CK 20 and neurofilament and negative for thyroid transcription factor-1, while lung small cell carcinoma is positive for thyroid transcription factor-1 and negative for CK 20 and neurofilament.
Most patients with metastatic thyroid cancer were asymptomatic at presentation. However, some patients with metastatic thyroid cancer had symptoms such as palpable neck tumor, dysphagia, or hoarseness (30). In this case, the patient initially presented with palpable neck tumor.
Although surgical removal of metastatic thyroid cancer is performed to prevent potential morbidity related to recurrence in the neck. However, prognosis is poor in most patients. For metastatic thyroid cancer, systemic therapy with chemotherapy is the treatment of choice.
Radioactive iodine therapy is not indicated for metastatic thyroid cancer.
In conclusion, we present a highly rare case of a patient with metastasis of MCC to thyroid gland. In this case, thyroidectomy did not appear to affect the patient's prognosis, but our patient had some symptoms and we decided to undergo thyroid lobectomy. The clinical significance of this case is that any abnormal findings in the thyroid gland in patients with MCC, the possibility of metastasis from the primary malignancy should always be evaluated.
Early and prompt diagnosis can facilitate appropriate treatment and may improve prognosis.
REFERENCES
1. Toker C. Trabecular carcinoma of the skin. Arch Dermatol 1972;105:107-10.
PUBMED | CROSSREF
2. Albores-Saavedra J, Batich K, Chable-Montero F, Sagy N, Schwartz AM, Henson DE. Merkel cell carcinoma demographics, morphology, and survival based on 3870 cases: a population based study. J Cutan Pathol 2010;37:20-7.
PUBMED | CROSSREF
3. Bichakjian CK, Lowe L, Lao CD, Sandler HM, Bradford CR, Johnson TM, et al. Merkel cell carcinoma:
critical review with guidelines for multidisciplinary management. Cancer 2007;110:1-12.
PUBMED | CROSSREF
4. Stoll L, Mudali S, Ali SZ. Merkel cell carcinoma metastatic to the thyroid gland: aspiration findings and differential diagnosis. Diagn Cytopathol 2010;38:754-7.
PUBMED | CROSSREF
5. Medina-Franco H, Urist MM, Fiveash J, Heslin MJ, Bland KI, Beenken SW. Multimodality treatment of Merkel cell carcinoma: case series and literature review of 1024 cases. Ann Surg Oncol 2001;8:204-8.
PUBMED | CROSSREF
6. Heath M, Jaimes N, Lemos B, Mostaghimi A, Wang LC, Peñas PF, et al. Clinical characteristics of Merkel cell carcinoma at diagnosis in 195 patients: the AEIOU features. J Am Acad Dermatol 2008;58:375-81.
PUBMED | CROSSREF
7. Engels EA, Frisch M, Goedert JJ, Biggar RJ, Miller RW. Merkel cell carcinoma and HIV infection. Lancet 2002;359:497-8.
PUBMED | CROSSREF
8. Buell JF, Trofe J, Hanaway MJ, Beebe TM, Gross TG, Alloway RR, et al. Immunosuppression and Merkel cell cancer. Transplant Proc 2002;34:1780-1.
PUBMED | CROSSREF
9. Vlad R, Woodlock TJ. Merkel cell carcinoma after chronic lymphocytic leukemia: case report and literature review. Am J Clin Oncol 2003;26:531-4.
PUBMED | CROSSREF
10. Pectasides D, Pectasides M, Economopoulos T. Merkel cell cancer of the skin. Ann Oncol 2006;17:1489-95.
PUBMED | CROSSREF
11. Wong HH, Wang J. Merkel cell carcinoma. Arch Pathol Lab Med 2010;134:1711-6.
PUBMED | CROSSREF
12. Poulsen M. Merkel-cell carcinoma of the skin. Lancet Oncol 2004;5:593-9.
PUBMED | CROSSREF
13. Allen PJ, Bowne WB, Jaques DP, Brennan MF, Busam K, Coit DG. Merkel cell carcinoma: prognosis and treatment of patients from a single institution. J Clin Oncol 2005;23:2300-9.
PUBMED | CROSSREF
14. Pellegriti G, Frasca F, Regalbuto C, Squatrito S, Vigneri R. Worldwide increasing incidence of thyroid cancer: update on epidemiology and risk factors. J Cancer Epidemiol 2013;2013:965212.
PUBMED | CROSSREF
15. Cramer JD, Fu P, Harth KC, Margevicius S, Wilhelm SM. Analysis of the rising incidence of thyroid cancer using the Surveillance, Epidemiology and End Results national cancer data registry. Surgery 2010;148:1147-53.
PUBMED | CROSSREF
16. Willis RA. Metastatic tumours in the thyreoid gland. Am J Pathol 1931;7:187-208.3.
PUBMED
17. Wychulis AR, Beahrs OH, Woolner LB. Metastasis of carcinoma to the thyroid gland. Ann Surg 1964;160:169-77.
PUBMED | CROSSREF
18. Papi G, Fadda G, Corsello SM, Corrado S, Rossi ED, Radighieri E, et al. Metastases to the thyroid gland:
prevalence, clinicopathological aspects and prognosis: a 10-year experience. Clin Endocrinol (Oxf ) 2007;66:565-71.
PUBMED | CROSSREF
19. Cichoń S, Anielski R, Konturek A, Barczyński M, Cichoń W. Metastases to the thyroid gland: seventeen cases operated on in a single clinical center. Langenbecks Arch Surg 2006;391:581-7.
PUBMED | CROSSREF
20. Nixon IJ, Coca-Pelaz A, Kaleva AI, Triantafyllou A, Angelos P, Owen RP, et al. Metastasis to the thyroid gland: a critical review. Ann Surg Oncol 2017;24:1533-9.
PUBMED | CROSSREF
21. Hegerova L, Griebeler ML, Reynolds JP, Henry MR, Gharib H. Metastasis to the thyroid gland: report of a large series from the Mayo Clinic. Am J Clin Oncol 2015;38:338-42.
PUBMED | CROSSREF
22. Tai PT, Yu E, Winquist E, Hammond A, Stitt L, Tonita J, et al. Chemotherapy in neuroendocrine/Merkel cell carcinoma of the skin: case series and review of 204 cases. J Clin Oncol 2000;18:2493-9.
PUBMED | CROSSREF
23. Eng TY, Boersma MG, Fuller CD, Goytia V, Jones WE 3rd, Joyner M, et al. A comprehensive review of the treatment of Merkel cell carcinoma. Am J Clin Oncol 2007;30:624-36.
PUBMED | CROSSREF
24. Coggshall K, Tello TL, North JP, Yu SS. Merkel cell carcinoma: an update and review: pathogenesis, diagnosis, and staging. J Am Acad Dermatol 2018;78:433-42.
PUBMED | CROSSREF
25. Harms KL, Healy MA, Nghiem P, Sober AJ, Johnson TM, Bichakjian CK, et al. Analysis of prognostic factors from 9387 Merkel cell carcinoma cases forms the basis for the new 8th edition AJCC staging system. Ann Surg Oncol 2016;23:3564-71.
PUBMED | CROSSREF
26. Vaiciunaite D, Beddell G, Ivanov N. Merkel cell carcinoma: an aggressive cutaneous carcinoma with rare metastasis to the thyroid gland. BMJ Case Rep 2019;12:e228273.
PUBMED | CROSSREF
27. Muratli A, Erdogan N, Sevim S, Unal I, Akyuz S. Diagnostic efficacy and importance of fine-needle aspiration cytology of thyroid nodules. J Cytol 2014;31:73-8.
PUBMED | CROSSREF
28. Becker JC, Stang A, DeCaprio JA, Cerroni L, Lebbé C, Veness M, et al. Merkel cell carcinoma. Nat Rev Dis Primers 2017;3:17077.
PUBMED | CROSSREF
29. Bobos M, Hytiroglou P, Kostopoulos I, Karkavelas G, Papadimitriou CS. Immunohistochemical distinction between merkel cell carcinoma and small cell carcinoma of the lung. Am J Dermatopathol 2006;28:99-104.
PUBMED | CROSSREF
30. Chung AY, Tran TB, Brumund KT, Weisman RA, Bouvet M. Metastases to the thyroid: a review of the literature from the last decade. Thyroid 2012;22:258-68.
PUBMED | CROSSREF