INTRODUCTION
Various clinical terms to describe the osteochondral lesions of the talar dome, such as transchondral fractures, osteochondral fractures, osteochondritis dissecans, talar dome fractures, and flake fractures-which have been used interchangeably-exist [1]. In 1737, the initial report of osteochondral loose bodies after trauma was made by Monro [2]. Later in 1888, König [3] first began to use the term osteochondritis dissecans of the knee to describe the natural onset of osteonecrosisinduced formation of osteochondral loose bodies. In 1922, Kappis [4] applied this terminology to the same condition in the ankle. Conversely, Berndt and Harty [5] used the term transchondral fracture to describe an osteochondral fractureinduced traumatic lesion in 1959. Subsequent studies investigated the pathological origin of osteochondral lesions and in 1966, Campbell and Ranawat [6] suggested that focal bleeding in the talus is one cause of osteonecrosis. Thus, the various terminologies used to describe osteochondral fractures of the talus are closely related to the mode of fracture onset. However, in recent years, it has been proposed to collectively call these lesions, osteochondral lesions of
talus (OLT), where all lesions called under this group have similar radiological findings. Lesions of OLT group whose pathological origin may differ and includes even chronic lesions that may result from trauma or trivial trauma from focal bleeding in the talar dome [1].
OLT makes up 0.09% of all bony lesions, 1% of all lesions of the talus, and approximately 4% of all osteochondral lesions [7]. OLT had been a condition whose radiological identification by simple radiographs had been readily missed. However, various factors such as improvements in diagnostic tools such as bone scintigraphy, increases in knee arthroscopies, and increases in sports activities in all ages are set to increase the prevalence of OLT in the future [7].
A traumatic experience is one of the clearest causes of the onset of OLT. Other possible causes include focal bleeding induced by osteonecrosis, systemic vascular disease, acute trauma, neglected trivial trauma, endocrine or metabolic disorders, degenerative joint diseases, misalignment of joints, and genetic predispositions. In general, the occurrence of OLT is more common on the medial in the region of posterior talus, and in case of the lateral talus, it occurs more commonly on the anterior side, where the Osteochondral lesions of the talus are usually induced by injuries of the ankle or repeated microfractures. If left untreated it can be the cause of chronic pain in the ankle joints. Radiological examination, computed tomography, or magnetic resonance imagingbased diagnoses are most effective in detecting osteochondral lesions of the talus.
The recommended first line of treatment options for ostechondral lesions of the talus are arthroscopic debridement, arthropscopic microfracture, and arthroscopic multiple drilling. In case where the first line of approach fails or the lesion is large, alternative options are to use autologous osteochondral graft transplantation, autologous chondrocyte implantation, and osteochondral allograft transplantation.
Keywords: Talus; Osteochondral lesion; Arthroscopy; Microfracture; Mosaicplasty
Surgical treatment of osteochondral lesion of talus
Min-Ho Shin, Hong-Geun Jung, Sang-Hun Lee
Department of Orthopedic Surgery, Konkuk University School of Medicine, Seoul, Korea
Copyright © 2014 Korean Arthroscopy Society and Korean Orthopedic Society for Sports Medicine. All rights reserved.
CC This is an open-access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/
by-nc/3.0) which permits unrestricted noncommercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received November 29, 2013; Revised February 24, 2014; Accepted March 11, 2014
Correspondence to: Hong-Geun Jung, Department of Orthopedic Surgery, Konkuk University School of Medicine, 120-1 Neungdong-ro, Gwangjin-gu, Seoul 143-729, Korea. Tel: +82-2-2030-7609, Fax: +82-2-2030-7369, E-mail: [email protected]
Arthroscopy and Orthopedic Sports Medicine
AOSM
lesion is usually induced by trauma. Further, lesions of the lateral side have been shown to be in general more severe than the medial side.
DIAGNOSIS OF OLT
Clinical diagnosis
The average age of OLT onset is between 20-30 years of age. The likelihood of OLT is greater in males, the percentage of OLT occurrence in men being around 70%, and in women 30%. The bilateral occurrence of OLT is 10% [8]. An OLT patient usually has a history of varus injury of the ankle and chronic ankle pain, where the pain is usually localized to the region of the osteochondral lesion. Therefore, it is often that OLT patients also have local tenderness of the ankle. Other common findings in patients with OLT are recurrent edema, stiffness, or instability of the ankle. Taking consideration of the patient’s history, if there is a suspected lesion, both the anterolatral side of the talar dome in a plantarflexion and the medial and posterior side of the talar dome in a dorsiflexion should be investigated. However, even if the patient has no history of tenderness of the ankle, a diagnosis of OLT cannot be dismissed.
Radiological diagnosis
In simple radiographs of an ankle (anteroposterior and frontal views under weightbearing, mortise) in patients
with OLT, the anterior to middle osteochondral lesion is seen as a nonpenetrative identity from the shoulder of the talus, and loss of bone continuity is seen. The posterior osteochondral lesion can be seen on mortise radiographs taken with the patient standing with their heels 4 cm above ground [9]. Although not seen in 30%-43% of simple radiographs [7], there is a tendency of lesions to become larger, thus it is clinically meaningful to take periodical radiographs over time in OLT patients.
In comparison to simple radiographs, computed tomography (CT) of OLT patients is useful in that it can locate the position, size, shape of the lesion and extent of the displacement of osteochondral fragments, but its usefulness is limited in the detection of articular cartilage, bony contusions, and nondisplaced lesions.
Bone scintigraphy is effective in detecting lesions that were not detected by simple radiographs, having a negative predictive value of 94%. Thus, a negative bone scintigraphy is a fairly reliable marker to exclude the diagnosis of osteochondral lesions, thereby omitting the requirement of subsequent diagnostic tests.
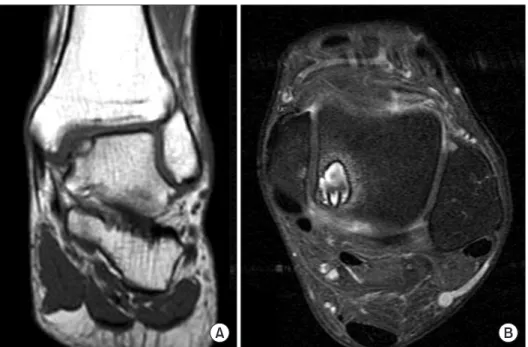
Magnetic resonance imaging (MRI) can be used to detect both lesions of articular cartilage and subchondral bone and even the surrounding soft tissue can be assessed. Although other benefits of MRI include early detection of premature subchondral lesions (Fig. 1) [8], a concern one should be aware of MRIs is that the severity of bony lesions can often be overestimated [10].
Fig. 1. Magnetic resonance imaging finding of osteochondral lesion of talus (OLT). (A) Coronal view shows osteo chon
dral lesion of medial talar dome. (B) Axial view shows cystic type OLT.
Classification of osteochondral lesions of talus
The classification of OLT can be based on findings from simple radiographs, CT scans, MRIs, or arthroscopic findings. In 1959, Berndt and Harty [5] published a classification system based on findings from simple radiographs. However, the specificity and the selectivity of this system are limited and only OLT that are detectable by radiography and that can be classified according to the system can be considered. In contrast, Ferkel et al.
[11] proposed a CTbased classification system, whereas Anderson et al. and many others have proposed MRI
based classification systems [12-14]. These classification systems have been merited for their ability to determine the severity of lesions. However, the accuracy of MRI
based classification systems to discern severity of lesions has been under dispute as when edema occurs, as in mild ankle injury, it can be seen as large changes in MRI, thus an overdiagnosis of OLT can often be made (Table 1) [15].
Other classification systems are based on arthroscopic findings. In 1986, Pritsch et al. [16] established a 3class arthroscopic classification system of articular cartilage.
Cheng et al. [17] in 1995, also using arthroscopy, based their OLT diagnosis on a 6level classification system that ranges from a scale of smooth, intact but soft to displaced osteochondral fragments (Table 2).
SURGICAL TREATMENT OF OLT
The treatment of OLT can be broadly classified into non
surgical and surgical treatment. Factors determining which treatment method is employed are symptoms of OLT, age of patient at OLT onset, and size, depth, or
location of lesion. In general, nonsurgical treatments include cast immobilization and physiotherapy. Surgical treatments include fixative methods for acute fractures and large lesions, whereas debridement, multiple drilling, and microfracture treatments are standard procedures.
More invasive methods include autologous osteochondral graft transplantation, autologous chondrocyte implan
tation (ACI), and osteochondral allograft transplantation, where tissue transplantation is used.
Chondral plate fixation (internal fixation)
When large and unstable osteochondral lesions contain salvageable subchondral parts, as in either type 3 or type 4 acute osteochondral lesions, chondral plate fixation to repair lesions over resection is advised. Anderson and Pagnani [18] have reported that resection of large and unstable lesions, rather than fixing them, leads to long
term pain and degenerative changes in the ankle. Thus, the chondral plate fixation approach is initially taken as an approach. One example of this conservative approach to fix lesions is the use of locking plates. Although this approach has the downside that if complications arise the locking plates must be postsurgical removed, nowadays, the use of bioabsorbable screws avoids the post
surgical removal of the plate [19]. Lastly, chondral plate fixation has been used to satisfactorily treat acuteonset osteochondral lesions, but the results have been poor for treatment of chronic osteochondral lesions [18].
Microfracture and multiple drilling
In general, arthroscopic surgeries are less invasive than openankle surgeries. Arthroscopic surgeries are associated with less complication and less incidence of ankylosis, and are associated with early rehabilitation. Arthroscopic surgical techniques that promote formation of fibrous cartilage through the stimulation of the subchondral bone marrow of the talus are endoscopic curettage, debridement, multiple drilling, and microfracture etc.
These have been considered as the firstline of approach in the treatment of OLT.
The main surgical goal of such treatment methodologies is to regain vascularization at the region of bone deficit to promote healing. In comparison to fibrous cartilage, hyaline cartilage is an avascular tissue and its regenerative abilities are weak. The generation of fibrous cartilage occurs with sufficient blood supply. Therefore, injuries that do not pass through the subchondral plate, does not regenerate fibrous cartilage through induction of Table 1. Magnetic resonance imaging staging for osteochondral lesions
of talus [15]
Stage I Stage IIA Stage IIB Stage III Stage IV
Subchondral trabecular compression Subchondral cyst
Incomplete separation of fragment Unattached, undisplaced fragment Displaced fragment
Table 2. Arthroscopic classification [17]
Arthroscopic classification Grade A
Grade B Grade C Grade D Grade E Grade F
Smooth, intact but soft or ballotable Rough surface
Fibrillations and fissures Flap present or bone exposed Loose, undisplaced fragment Displaced fragment
an inflammatory response as they do not have access to blood circulation. However, if the injury passes deep into the subchondral bone, this causes the bone marrow to bleed, and subsequent necrosis of the region of cartilage deficit occurs. As the resultant blood clots contain stem cells originating from the bone marrow, this leads to differentiation of the chondrocytes and chondrocyte regeneration fills up the area of deficit [14,20]. Although during this process the regenerated fibrous cartilage can fill the area of deficit, since it lacks many of the biomechanical properties of hyaline cartilage, despite regeneration of tissue complications can occur [21,22]. Since the use of debridement, multiple drilling, and microfractures can lead to greater fibrous cartilage regeneration than hyaline cartilage, these methods should be used for lesions with a diameter of less than 10 mm and those that have minimal injuries to the subchondral bone.
To initially examine which technique should be employed for the treatment of OLT in a patient, a diagnostic arthro
scopic examination should be made. For example, if by arthro scopy a subchondral lesion is seen to contain cartilage damage it is advised to use retrograde drilling, whereas if an unstable, extensive lesion is seen, endoscopic curettage, microfracture, or multiple drilling is advised. Although it is yet controversial as to whether the multiple drilling or the microfracture is the better approach, in case of the multiple drilling technique, the heat generated from the drill may damage the tissue further and as a tibial penetration or medial osteotomy is required to access the lesion, it is considered a relatively more invasive technique [12,23]. Microfracture can, irrespective of the lesion position, use a bendable awl to directly access the osteochondral lesion without causing any additional
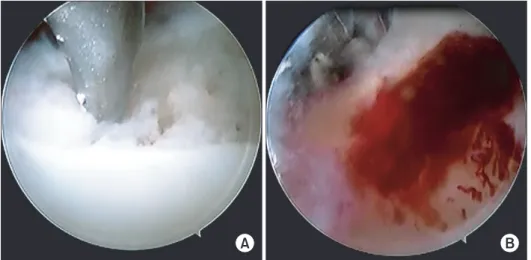
tissue invasion. In microfracture, leveled drilling of the lesion allows homogenization of blood clots that are released from the bone marrow (Fig. 2) [20]. Good clinical outcomes using microfracture in OLT patients have been shown. For example, Berndt and Harty [5], in a patient group of 105, performed microfracture when lesions were smaller than 15 mm, and found that irrespective of the lesion position, a good clinical outcome was seen. Further, Becher and Thermann [24] found that microfracture of OLT gave significantly good clinical results in patients with osteochondral bone deficits even when degenerative articular deficits were concomitant-the clinical results were moderate in patients over the age of 50. Other groups have shown that microfractures successfully treat OLT of subchondral cyst shaped lesions [25]. Thus, microfractures are one of the most useful invasive treatments to repair OLT.
Nevertheless, we recommend that the first line of treatment option for OLT is a noninvasive arthroscopic approach. However, when the region of deficit becomes larger in OLT, many of the treatment options cannot overcome the problem of excessive fibrous cartilage generation in the region of deficit. In such cases, methods such as autologous osteochondral graft transplantation, ACI, and osteochondral allograft transplantation that can promote the growth of hyaline cartilage are recommended.
Retrograde drilling
Retrograde drilling can be used if the osteocondral bone covering the subcondral lesion is intact. The technique of retrograde drilling allows treatment of the lesion without compromising the integrity of the joint surface. Early studies by Lee and Mercurio [26] in 1981 had used open
Fig. 2. Arthroscopic finding shows microfracture procedure using a micro
spike (A) and bleeding from subchondral plate after microfracture procedure (B).
surgery, but nowadays, arthroscopic methods are used.
Even imposing a small pressure on the lesion may lead to collapse of the articular surface, therefore, allograft transplantation to fill the space after resection of the lesion is usually performed. If it is difficult to find an allograft whose size fits well into the articular space, recently, graft replacement materials such as, calcium sulfate, have been used in parallel or instead of allografts [27].
A main difficulty in the retrograde drilling technique is determining the exact location of the lesion and performing the drilling without damaging the upper layer of the osteochondral lesion. Recent computerassisted technique has been used to improve the accuracy and hurdles of this technique, and has shown good clinical outcomes in OLT treatment [28].
Autologous osteochondral graft transplantation, autologous chondrocyte implantation, and osteochondral allograft transplantation
If the size of osteochondral lesions is large, autologous osteochondral graft transplantation, ACI, and osteo chon
dral allograft transplantation are alternative treatment options. Such graft transplantations require a vertical approach of the lesion, and thus require additional steps such as the osteotomy. The majority of talar domes can be accessed vertically without osteotomy, but 17% of medial talar domes, and 20% of lateral talar domes cannot be accessed vertically without osteotomy [29]. The technique of transmalleolar osteotomy to expose the medial and lateral talar domes in general allows vertical access;
however, around 15% of central talar domes cannot be accessed vertically even with transmalleolar osteotomy.
Complications at postosteotomy such as nonunion or misunion of the osteotomized region can occur.
Autologous osteochondral graft transplantation
In autologous osteochondral graft transplantation, osteo
chondral fragments extracted from articular cartilage of the femoral head of the knee under no weight bearing are used as grafts for transplantation (Fig. 3). Yamashita et al.
[30] were the initial group to implement this technique, and showed that it gives good clinical outcomes in OLT treatment. Subsequent studies by Draper and Fallat [31]
found that in relative to other techniques, the outcome of autologous osteochondral graft transplantation is superior. This is because the region of deficit is filled by osteochondral fragments, and this allows resumption of normal weight bearing at the joint which in turn reduces
compensatory load from the preserved talus. Further, as osteochondral lesion is replaced by the hyaline cartilage
subchondral bone complex, the replaced graft executes anatomically the biomechanical properties of the cartilage better than the fibrous cartilage generated by microfracture or multiple drilling techniques [5]. However, when using this technique for lesions where the deficit is large, using a sizeable donor site may be too invasive and lead to donor site complications. Therefore, in 1993, Matsusue et al. [32] took an approach to transplant multiple grafts in chondral lesions of the knee, termed as mosaicplasty, which reduced donor sites complications.
It has the added advantage that the deficit shape can be easily matched, and it bypasses the need for fixative screws. Hangody et al. [33] performed mosaicplasty on 36 OLT patients, and found good clinical outcomes in around 94% of patients, where none had complications arising from donor sites. They found at followup studies, arthroscopic followup was normal and continuity of the articular surface was seen. Recently, Sammarco and Makwana [34] reported of the attainment of donor site from a displaced talus rather than from the knee. In their report, 12 patients showed a significant improvement in recovery without any signs of complications. However, for such methods to work, the donor site surface area must not go over 8 mm, thus only OTL deficits of size smaller than this area can be treated.
Autologous osteochondral graft transplantation is by large a complicated procedure, and choice of cartilage donor sites is restricted. The candidates for donor sites are further reduced by the difficultly in matching the asymmetrically shaped osteochondral deficits, where ill
Fig. 3. Autologous osteochondral graft transplantation.
fitted sites are later unfavorably filled by fibrous cartilage [13].
Autologous chondrocyte implantation
ACI uses a section of knee cartilage and cultures them in vitro. First, cartilage cells are separated and cultured, which is then injected into the deficit region of OLT after resection of the lesion. During the subsequent healing process hyaline cartilage formation is promoted, as in the autologous osteochondral graft transplantation.
Early studies by Grande et al. [35] showed reconstruction of lesions in rabbits were injected with in vitro cultured grafts. Following this study, Brittberg et al. [36] prepared autologous chondrocytes from 23 patients in the same way and performed graft implantation in knee joints, and found good clinical outcomes in 18 patients, where 12 out of 22 grafts showed formation of hyaline cartilage.
Giannini et al. [37] applied this technique to treat OLT.
Their histological findings showed hyaline cartilage growth in the area of deficit and that these resembled the surrounding healthy chondrocytes. ACI uses a small sample of chondrocytes to start a culture, and therefore is not restricted by the size of the donor site and can be grown superfluously to fill up deficit of any sizes. However, limitations such as the need for two additional surgical steps due to the process of extracting and culturing of the chondrocytes, expensive costs, complicated surgical techniques, and layering due to overgrowth of chondrocytes exist [13].
Osteochondral allograft transplantation
Osteochondral allograft transplantation is a method that uses allografts to transplant into deficits from excised osteochondral fragments. It is used for lesions that have large osteochondral deficits, and is not limited by the size of the donor site, and thus is especially frequently implemented in knee surgeries [26]. Recently, it has been applied in the treatment of OLT. When Gross et al. [38]
used osteochondral allograft transplantation to treat OLT,
6 out of 9 patients (67%) saw satisfactory outcome. The main benefits of using allografts are that it bypasses the need for a donor site and the use of a singular sizeable graft minimizes the formation of fibrous cartilage between graft bones, which is a main disadvantage of mosaicplasty.
One limitation to this method is that, compared to the autologous graft transplantation method, the survival of cells posttransplantation is low. Survival of cells is lower in frozen allografts than in fresh allografts [39]. Another limitation is a possible immunological response. An immunological response is a greater problem in fresh allografts than in frozen allografts. Research to improve tissue compatibility in such transplantation procedure is required.
There are many opinions as to which treatment is most appropriate for the treatment of osteochondral lesions.
Zengerink et al. [40] have suggested that various treatments should be categorized based upon their most effectiveness in terms of the lesion state, size, and symptom, whereas Giannini and Vannini [13] suggested that the pros and cons of each type of treatments should be taken into consideration to decide on the best treatment option case
bycase (Table 3).
CONCLUSION
Asymptomatic or trivial OLT can be considered for con
servative treatment. For the surgical treatment of OLT, using arthroscopic debridement and microfracture have been shown to be an effective method with minimal complications and early rehabilitation, and thus has been recommended as the primary treatment option.
However, for the treatment of larger lesions, such as large cystic lesions, or of a previously failed arthroscopic treatment of OLT, using autologous osteochondral graft transplantation, ACI, and osteochondral allograft transplantation can be considered.
Table 3. Algorithmic treatment for osteochondral lesion of talus Size of lesion
(cm2)
Treatment used for patients
≤ 55 yr > 55 yr
1.5
3.0
Arthroscopic debridement, microfracture/multiple drilling
Arthroscopic debridement, microfracture/multiple drilling AOT or ACI
AOT or ACI
Arthroscopic debridement Microfracture/multiple drilling
Arthroscopic debridement, microfracture/multiple drilling AOT (in case of intact knee cartilage)
Arthrodesis or total joint arthroplasty AOT, autologous osteochondral graft transplantation; ACI, autologous chondrocyte implantation.
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.
1. Ferkel RD, Hommen JP. Arthroscopy of the ankle. In: Coughlin MJ, Mann RA, Saltzman CL, editors. Surgery of the foot and ankle.
Vol. II. 8th ed. Philadelphia, PA: Mosby; 2007. p. 667-77.
2. Monro A. Part of the cartilage of the joint separated and ossified.
In: Philosophical Society of Edinburgh, editor. Medical essays and observations. 2nd ed. Edinburgh: Ruddimans; 1737. p.305.
3. König F. Über freie Körper in den Gelenken [on the presence of loose bodies in joints]. Deutsche Zeitschr f Chir 1888;27:90-109.
4. Kappis M. Weitere Beiträge zur traumatisch-mechanischen Entstehung der “spontanen” Knorpelablösungen. Deutsche Zeitschr f Chir 1922;171:13-29.
5. Berndt AL, Harty M. Transchondral fractures (osteochondritis dissecans) of the talus. J Bone Joint Surg Am 1959;41:988- 1020.
6. Campbell CJ, Ranawat CS. Osteochondritis dissecans: the question of etiology. J Trauma 1966;6:201-21.
7. Grossman JP, Lyons MC 2nd. A review of osteochondral lesions of the talus. Clin Podiatr Med Surg 2009;26:205-26.
8. Chew KT, Tay E, Wong YS. Osteochondral lesions of the talus.
Ann Acad Med Singapore 2008;37:63-8.
9. Verhagen RA, Maas M, Dijkgraaf MG, Tol JL, Krips R, van Dijk CN. Prospective study on diagnostic strategies in osteochondral lesions of the talus. Is MRI superior to helical CT? J Bone Joint Surg Br 2005;87:41-6.
10. O’Loughlin PF, Heyworth BE, Kennedy JG. Current concepts in the diagnosis and treatment of osteochondral lesions of the ankle.
Am J Sports Med 2010;38:392-404.
11. Ferkel RD, Zanotti RM, Komenda GA, et al. Arthroscopic treatment of chronic osteochondral lesions of the talus: long- term results. Am J Sports Med 2008;36:1750-62.
12. Flick AB, Gould N. Osteochondritis dissecans of the talus (transchondral fractures of the talus): review of the literature and new surgical approach for medial dome lesions. Foot Ankle 1985;5:165-85.
13. Giannini S, Vannini F. Operative treatment of osteochondral lesions of the talar dome: current concepts review. Foot Ankle Int 2004;25:168-75.
14. Gill TJ, Asnis PD, Berkson EM. The treatment of articular cartilage defects using the microfracture technique. J Orthop Sports Phys Ther 2006;36:728-38.
15. Anderson IF, Crichton KJ, Grattan-Smith T, Cooper RA, Brazier D.
Osteochondral fractures of the dome of the talus. J Bone Joint Surg Am 1989;71:1143-52.
16. Pritsch M, Horoshovski H, Farine I. Arthroscopic treatment of osteochondral lesions of the talus. J Bone Joint Surg Am 1986;68:862-5.
17. Cheng MS, Ferkel RD, Applegate GR. Osteochondral lesions of the talus: a radiologic and surgical comparison. In: American Academy of Orthopaedic Surgeons, editor. Oral paper presented at the 61st Annual Meeting of the American Academy of Orthopaedic Surgeons (AAOS); 1994 Feb; New Orleans, LA. [Place unknown]: Journal of Bone and Joint Surgery Inc.; 1995.
18. Anderson AF, Pagnani MJ. Osteochondritis dissecans of the femoral condyles. Long-term results of excision of the fragment.
Am J Sports Med 1997;25:830-4.
19. Dervin GF, Keene GC, Chissell HR. Biodegradable rods in adult osteochondritis dissecans of the knee. Clin Orthop Relat Res 1998;(356):213-21.
20. Williams RJ 3rd, Harnly HW. Microfracture: indications, technique, and results. Instr Course Lect 2007;56:419-28.
21. Gudas R, Kalesinskas RJ, Kimtys V, et al. A prospective randomized clinical study of mosaic osteochondral autologous transplantation versus microfracture for the treatment of osteochondral defects in the knee joint in young athletes.
Arthroscopy 2005;21:1066-75.
22. Shapiro F, Koide S, Glimcher MJ. Cell origin and differentiation in the repair of full-thickness defects of articular cartilage. J Bone Joint Surg Am 1993;75:532-53.
23. Alexander AH, Lichtman DM. Surgical treatment of transchondral talar-dome fractures (osteochondritis dissecans). Long-term follow-up. J Bone Joint Surg Am 1980;62:646-52.
24. Becher C, Thermann H. Results of microfracture in the treatment of articular cartilage defects of the talus. Foot Ankle Int 2005;26:583-9.
25. Jung HG, Carag JA, Park JY, Kim TH, Moon SG. Role of arthroscopic microfracture for cystic type osteochondral lesions of the talus with radiographic enhanced MRI support. Knee Surg Sports Traumatol Arthrosc 2011;19:858-62.
26. Lee CK, Mercurio C. Operative treatment of osteochondritis dissecans in situ by retrograde drilling and cancellous bone graft:
a preliminary report. Clin Orthop Relat Res 1981;(158):129-6.
27. Beaver RJ, Mahomed M, Backstein D, Davis A, Zukor DJ, Gross AE. Fresh osteochondral allografts for post-traumatic defects in the knee. A survivorship analysis. J Bone Joint Surg Br 1992;74:105-10.
28. Citak M, Kendoff D, Kfuri M Jr, Pearle A, Krettek C, Hüfner T.
Accuracy analysis of Iso-C3D versus fluoroscopy-based navigated retrograde drilling of osteochondral lesions: a pilot study. J Bone Joint Surg Br 2007;89:323-6.
29. Muir D, Saltzman CL, Tochigi Y, Amendola N. Talar dome access for osteochondral lesions. Am J Sports Med 2006;34:1457-63.
30. Yamashita F, Sakakida K, Suzu F, Takai S. The transplantation
REFERENCES
of an autogeneic osteochondral fragment for osteochondritis dissecans of the knee. lin Orthop Relat Res 1985;(201):43-50.
31. Draper SD, Fallat LM. Autogenous bone grafting for the treatment of talar dome lesions. J Foot Ankle Surg 2000;39:15-23.
32. Matsusue Y, Yamamuro T, Hama H. Arthroscopic multiple osteochondral transplantation to the chondral defect in the knee associated with anterior cruciate ligament disruption.
Arthroscopy 1993;9:318-21.
33. Hangody L, Kish G, Módis L, et al. Mosaicplasty for the treatment of osteochondritis dissecans of the talus: two to seven year results in 36 patients. Foot Ankle Int 2001;22:552-8.
34. Sammarco GJ, Makwana NK. Treatment of talar osteochondral lesions using local osteochondral graft. Foot Ankle Int 2002;23:693-8.
35. Grande DA, Pitman MI, Peterson L, Menche D, Klein M. The repair of experimentally produced defects in rabbit articular cartilage by autologous chondrocyte transplantation. J Orthop
Res 1989;7:208-18.
36. Brittberg M, Lindahl A, Nilsson A, Ohlsson C, Isaksson O, Peterson L. Treatment of deep cartilage defects in the knee with autologous chondrocyte transplantation. N Engl J Med 1994;331:889-95.
37. Giannini S, Buda R, Grigolo B, Vannini F. Autologous chondrocyte transplantation in osteochondral lesions of the ankle joint. Foot Ankle Int 2001;22:513-7.
38. Gross AE, Agnidis Z, Hutchison CR. Osteochondral defects of the talus treated with fresh osteochondral allograft transplantation.
Foot Ankle Int 2001;22:385-91.
39. Catanzariti A, Karlock L. The application of allograft bone in foot and ankle surgery. J Foot Ankle Surg 1996;35:440-51.
40. Zengerink M, Szerb I, Hangody L, Dopirak RM, Ferkel RD, van Dijk CN. Current concepts: treatment of osteochondral ankle defects. Foot Ankle Clin 2006;11:331-59.
![Table 2. Arthroscopic classification [17]](https://thumb-ap.123doks.com/thumbv2/123dokinfo/5363547.194326/3.892.77.425.841.922/table-arthroscopic-classification.webp)