REVIEW ARTICLE
비알코올 지방간 질환에서 심혈관 질환의 위험
김학수, 조용균
성균관대학교 의과대학 강북삼성병원 소화기내과
Cardiovascular Risk in Patients with Non-alcoholic Fatty Liver Disease
Hak Soo Kim and Yong Kyun Cho
Division of Gastroenterology, Department of Internal Medicine, Kangbuk Samsung Hospital, Sungkyunkwan University School of Medicine, Seoul, Korea
Non-alcoholic fatty liver disease (NAFLD) includes a wide spectrum of diseases that range from simple steatosis to non-alcoholic stea- tohepatitis (NASH) and cirrhosis. In addition, the burden of NAFLD is rapidly growing. Previously, NAFLD was regarded as a hepatic manifestation of metabolic syndrome, which is a traditional cardiovascular disease (CVD) risk factor. However, there has been an increasing evidence that suggest NAFLD to be an independent risk factor of CVD. Therefore, currently, NAFLD should be reconsidered as not only a simple manifestation of metabolic syndrome, but also a systemic disease that contribute to CVD. There are some reason- able hypotheses about the relationship between NAFLD and CVD. Moreover, many studies have been performed to better understand this relationship. Nonetheless, the underlying mechanisms and pathogenesis of NAFLD that contribute to CVD have not yet been fully elucidated to date. This review focuses on the underlying mechanisms and relationship between NAFLD and CVD. (Korean J Gastroenterol 2017;69:333-340)
Key Words: Non-alcoholic fatty liver disease; Cardiovascular disease
Received May 12, 2017. Revised May 23, 2017. Accepted May 28, 2017.
CC This is an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/
by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Copyright © 2017. Korean Society of Gastroenterology.
교신저자: 조용균, 03181 서울시 종로구 새문안로 29, 성균관대학교 의과대학 강북삼성병원 소화기내과
Correspondence to: Yong Kyun Cho, Division of Gastroenterology, Department of Internal Medicine, Kangbuk Samsung Hospital, Sungkyunkwan University School of Medicine, 29 Saemunan-ro, Jongno-gu, Seoul 03181, Korea. Tel: +82-2-2001-8557, Fax: +82-2-2001-2610, E-mail: choyk2004.cho@samsung.com
Financial support: None. Conflict of interest: None.
서 론
비알코올 지방간 질환(non-alcoholic fatty liver disease, NAFLD)은 간 질환을 초래하는 약물 및 알코올 등의 복용력 이 없으면서, 영상학적 검사나 조직검사 내에서 간 내에 지방 이 침착되어 알코올 간 질환과 유사한 조직학적 소견을 보이 는 질환을 통칭하는 용어로, 간 내에 지방 침착은 보이지만 간세포 손상이나 섬유화가 없는 비알코올 단순 지방간(simple steatosis)에서부터 간세포 손상을 동반하는 비알코올 지방간 염(non-alcoholic steatohepatitis, NASH) 및 섬유화를 동반 하여 간경화가 발생하는 비알코올 지방간 질환 연관 간경변증 을 포함한다.1이러한 NAFLD는 현재 서구사회에서 발생하는
만성 간 질환의 가장 흔한 원인으로 알려져 있고, 성인 인구에 서의 유병률은 20-30%까지 보고되고 있으며, 특히 비만하거 나 당뇨병이 있는 환자군에서는 유병률이 70-90%까지 증가 하는 경향을 보이고 있다.2-5 국내에서도 서구화된 식생활과 운동량의 부족, 생활 습관의 변화 등으로 인해 NAFLD의 유 병률은 꾸준하게 증가되는 양상으로, 대략 16-33% 정도로 보 고되고 있으며, 예방접종 및 우수한 효과를 보이는 항바이러 스제의 개발로 만성 B형 및 C형간염의 유병률이 감소하는 상 황에서 더욱 중요한 간 질환의 하나로 자리매김할 것으로 생 각된다.6,7
과거 비알코올 간 질환은 단순히 대사증후군의 간 내 표현 형으로 여겨졌으나, 최근 NAFLD 자체가 심혈관계 질환
(cardiovascular disease, CVD), 고혈압, 당뇨병, 대사증후군 등 다양한 만성 질환의 독립적인 위험인자라는 사실이 알려지 고 있다.8-10 또한 NAFLD 환자의 가장 흔한 사망 원인이 CVD로 밝혀지면서 NAFLD와의 관계 및 이에 대한 메커니즘 에 대한 연구들이 활발히 진행되고 있어 본 종설에서는 NAFLD와 CVD와의 연관성 및 이에 대한 가설들에 대해 논 하고자 한다.
본 론
1. 일반적인 고찰
1) CVD 지표들과 NAFLD
혈관의 죽상경화성 변화를 동반하게 되는 심혈관 질환의 혈관 변화를 예측하는 지표 중 대표적인 것으로, 경동맥 내중 막 두께(carotid artery intima-media thickness)의 증가, 경 동맥 죽상반(carotid artery plaque), 혈관 내피세포의 기능이 상(endothelial dysfunction), 동맥벽의 탄성 저하(increased arterial wall stiffness), 관상동맥 석회화 지수 상승(increased coronary artery calcium score), 좌심실 기능이상, 관상동맥 관류 저하 등이 있다.11-16
복부 초음파로 진단된 NAFLD 3,497명을 대상으로 진행된 메타분석에서 경동맥 내중막 두께 증가가 확인되었고, 경동맥 죽상경화반의 빈도도 유의하게 높았으며,17 27개의 연구를 대 상으로 진행된 메타분석에서도 NAFLD군에서 경동맥 내중막 두께 증가 및 관상동맥 석회화 지수 상승이 기존에 알려진 전통적인 심혈관계 위험 요소와 독립적으로 유의하게 나타났 다.18이러한 유의성은 국내 연구에서도 발견되는데, 만 명 이 상의 직업 코호트 연구에서 기존에 알려진 심혈관계 위험 요 소와 독립적으로 관상동맥 석회화 지수의 상승(increased coronary artery calcium score)이 확인되었다.19
동맥경화의 초기 지표이며 혈관내피세포이상(endothelial dysfunction)을 보여주는 상완동맥의 혈관확장능력(brachial artery endothelial flow-mediated vasodilatation)이 당뇨병 과 독립적으로 NAFLD군에서 감소하였고, 이러한 감소는 간 의 조직학적 중증도와 비례한 반면, 나이, 성별, 체질량 지수, 인슐린 저항성 및 다른 대사증후군 인자들과 독립적인 것으로 나타났다.20-22또한 초기에 나타나는 좌심실 기능이상이 NAFLD 군에서 나타났고,23-26제2형 당뇨병과 NAFLD가 동반된 군에 서 관상동맥의 관류 저하 소견이 제2형 당뇨병만 있는 군에 비해 유의하게 높게 관찰되었다.27
2) NAFLD 환자의 심혈관계 유병률, 사망률
지역사회 기반으로 미국에서 진행된 대규모 코호트 연구인
National Health and Nutrition Examination Survey-III에 서 복부 초음파로 진단된 총 11,371명의 NAFLD 환자를 추적 관찰한 결과, NAFLD군에서 인구학적 요소 및 기존의 위험인 자들과 독립적으로 CVD의 유병률이 높았다.28,29 이탈리아에 서 제2형 당뇨병을 가진 환자 2,103명을 대상으로 한 연구에 서도 NAFLD가 CVD의 유병률 및 이로 인한 사망률을 높이 는 위험 요소로 확인되었으며,30 중국에서 있었던 지역사회 기 반의 코호트 연구에서도 NAFLD군을 4년간의 추적 관찰한 결과 정상군에 비해 CVD로 인한 사망률이 약 3배 정도 높은 것으로 보고되었다.31 최근 대규모 메타분석에서도 NAFLD가 심혈관계의 위험 요소인 고혈압, 동맥경화 및 CVD의 유병률 과 관련이 있었다.32
이를 종합해볼 때 NAFLD와 CVD 사이의 유의한 관련성은 분명해 보인다. 다만, NAFLD가 인슐린 저항성을 기초로 하 고 있는 전통적인 심혈관계 위험인자인 당뇨병, 대사증후군과 그 뿌리를 같이 하고 있어 그 영향의 독립성을 규명하기 어려 운 점이 있으나, 최근의 연구 결과를 토대로 NAFLD가 분명 한 심혈관계 독립적 위험인자로 증명되고 있는 점이 주목된 다. 또한 진단 방법적인 측면에서 보면, 현재까지의 연구는 대부분이 비침습적인 복부 초음파로 NAFLD를 진단하였는 데, 이것이 연구의 제한점이 될 수 있겠으나, 조직학적으로 진단된 NAFLD 229명을 대상으로 한 후향적 코호트 연구 결 과에서도 CVD로 인한 사망이 유의하게 높았다는 점을 고려 해 보면, 진단 방법의 차이가 NAFLD와 CVD의 관련을 규명 하는 데 큰 영향을 미치지 않을 것으로 보인다.33
2. NAFLD와 CVD와의 연관성에 대한 메커니즘
1) 간 내 혈관의 구조적 변화 및 혈관 형성 인자
NAFLD의 경우 fat laden hepatocytes에 의해 간의 기본 구조인 동모양혈관(sinusoids)이 압박되면서 염증 반응과 더 불어 해부학적 변화가 일어나게 된다.34,35 이런 변화는 non- cirrhotic NAFLD의 경우에서도 문맥압항진이 발생할 수 있 고, 혈관 형성 인자(angiogenic factor)들에 영향을 줄 수 있
다.36,37 NAFLD군에서 metalloproteinase가 증가하는 것이
알려져 있으며,38큰 동맥의 중피(media of the large arteries) 를 구성하는 탄성섬유(elastin fiber)의 감소와 콜라겐 구성 성 분의 증가를 유발하여, 동맥의 탄성도 저하(increased arterial stiffness)를 초래하게 된다. 혈관내피세포 성장인자(vascular endothelial growth factor, VEGF)에 관한 몇 가지 연구들이 있었으나, 현재까지 일치된 의견은 없는 상태이다.39-42하지만 혈관내피세포 성장인자가 심혈관계 질환의 병리와 관련이 있으 며, 특히 혈관의 죽상화와 죽상경화반의 불안정성에 기여한다 는 사실이 알려져 있어 추가적인 연구가 필요한 실정이다.43,44
다른 혈관 형성 관련 인자로 high motility group box-1 (HMGB-1)은 혈관 형성을 유도하고, 간손상과 더불어 전신 염증 반응과 관련이 있는 것으로 보이는데, 최근 연구에서 NAFLD만 있는 군과 NAFLD 및 CVD가 동시에 있는 두 군을 비교한 연구에서 NAFLD만 있는 군보다 유의하게 높은 혈중 농도를 보였다.45
2) 혈관내피세포의 기능이상
CVD의 초기 단계에서 혈관의 내피세포의 기능이상이 나 타나게 되는데,46 NAFLD에서 내피세포의 기능이상이 관찰되 며, NASH에서 이러한 기능이상은 더욱 진행된 형태로 나타 난다.22 이는 asymmetric dimethyl arginine (ADMA)의 혈 중 농도의 증가와 관련이 있는데, ADMA는 nitric oxide syn- thase (NOS)를 분해하는 물질로, 혈중 ADMA가 증가하게 되 면 nitric oxide (NO)의 합성이 저하되어 결과적으로 혈관 탄성 도(arterial wall stiffness)가 악화된다. NAFLD군에서 ADMA 가 기존에 알려진 심혈관계 인자를 보정한 이후에도 독립적으 로 증가하는 것이 확인되었다.47 또한 내피세포가 파괴되면서 생성되는 endothelial microparticles와 내피세포의 교정에 관여하는 endothelial progenitor cell이 NAFLD군에서 각각 증가하고 감소하는 것이 확인되어, 직접적으로 내피세포의 기 능이상을 초래하는 것으로 보인다.48,49
3) 염증 반응과 사이토카인
NAFLD 환자에서 전신염증상태와 관련 있는 interleukin (IL)-1b의 혈중 상승이 유의하게 나타났고,50 IL-6가 간의 조직 학적 진행 정도와 비례하여 증가하는 양상을 보였다.51,52 이뿐만 아니라, high sensitivity C-reactive protein (hs-CRP), tumor necrosis factor (TNF)-a, chemokine (C-C motif) ligand 3 (CCL3), soluble intercellular adhesion moleculre-1 (slCAM-1)도 NAFLD 환자에서 증가하는 양상을 보였는데,51,53 간 내에는 다 양한 면역세포가 존재하며, 이러한 세포에서 분비되는 다양한 cytokines가 전신적인 염증 반응을 일으킬 수 있다는 점을 고려해볼 때 염증 반응이 CVD의 초기 반응인 혈관내피세포 의 기능 저하를 비롯하여 혈관의 죽상화와 과응고성을 초래할 수 있다는 주장은 설득력이 있어 보인다.
4) 혈중 호모시스테인(homocystein) 변화와 염증 반응 호모시스테인혈증은 CVD로 인한 사망률의 증가와 관련이 있다는 사실이 알려져 있으며, 독립적인 심혈관계 위험 요소 로 보인다.54,55 간은 이러한 호모시스테인을 포함하는 아미노 산을 대사하는 주요 장기로, NAFLD군에서 높은 호모스시테 인혈증이 일반적으로 관찰된다.56,57 호모시스테인의 대사이상 은 cysteine의 trans-sulfuration 감소와 methionine의 re-meth-
ylation과 동반되어 나타나는데,58-60 이러한 변화는 산화 스트 레스(oxidative stress)를 유발하며, 비알코올 단순 지방간 (simple steatosis)에서 NASH로의 진행에 관여할 뿐 아니라 호모시스테인혈증은 직접적으로 NO의 합성을 저해하고 간 내에 혈관 저항을 상승시킨다.61
5) Hepatokine과 인슐린 저항성
Hepatokine은 간에서 분비되는 물질로, paracrine 및 en- docrine의 효과를 나타낸다. 이 중에서 fetuin-A (FetA)는 간 과 근육에 존재하는 insulin receptor tyrosine kinase에 작 용하여 인슐린 저항성을 나타낸다.62 이뿐 아니라 FetA는 각 종 염증 cytokine 증가와 adiponectin의 감소를 유발하고,63 당과 지질 대사에 있어 중요한 역할을 하는 것으로 알려져 있으며, NAFLD, CVD 및 뇌졸중에서도 상승하는 것으로 밝 혀지면서 이에 대한 연구가 진행되었다. 하지만 Sato 등의 연 구에서, NAFLD군에서 경동맥 내중막 두께 증가와 FetA는 오히려 반대의 결과로 나타났는데,64 이는 FetA가 trans- forming growth factor (TGF)-β1 신호체계를 억제하는 방향 으로 작용하는 것과 관련이 있다. 종합해보면, NAFLD 환자 에서 보이는 FetA의 농도 증가는 인슐린 저항성을 일으켜 CVD를 일으키는 요인이 되기도 하며, 이와 더불어 TGF-β1 의 신호체계를 억제하여 혈관의 석회화(vascular calcifica- tion)를 억제하는 역할도 한다는 사실이 밝혀졌다.65
Fibroblast growth factor-21 (FGF-21)은 인슐린 감수성에 긍정적인 효과를 미치는 물질로, NAFLD군에서 그 값이 떨어 져 있을 것으로 추정하였으나 오히려 상승하는 소견이 관찰되 는데, 이는 인슐린 저항성에 대한 일종의 보상 반응으로 추정 된다.66-68
Selenoprotein P (SeP)는 인슐린 저항성과 더불어 염증 지 표인 high sensitivity C-reactive protein (hs-CRP)과 경동맥 내중막 두께 증가와 관련이 있는 물질로,69,70심혈관계 질환과 관련성이 있으나 10명의 비만 수술(bariatric surgery) 후 추 적 관찰 결과를 보면 오히려 SeP가 증가하는 양상을 보여 추 가적인 연구가 필요한 상황이다.71
6) 혈중 내 지질 변화
간은 지방대사의 주요 장기로, 각종 지질단백을 합성하고 대사 및 분비하는 기관이다. NAFLD에서 혈중 내에 지질의 변화가 나타나는데, 중성지방(triglyceride, TG) 및 저밀도 지 질단백(low density lipoprotein, LDL)이 증가하고, 고밀도 지질단백(high density lipoprotein, HDL)이 감소하게 되며, 혈관의 죽상화를 악화시키는 요인이 된다.72 특히 small dense LDL particles인 LDL3, LDL4가 증가하며, 이러한 경 향은 NASH 환자에서 더욱 뚜렷하게 나타난다.73
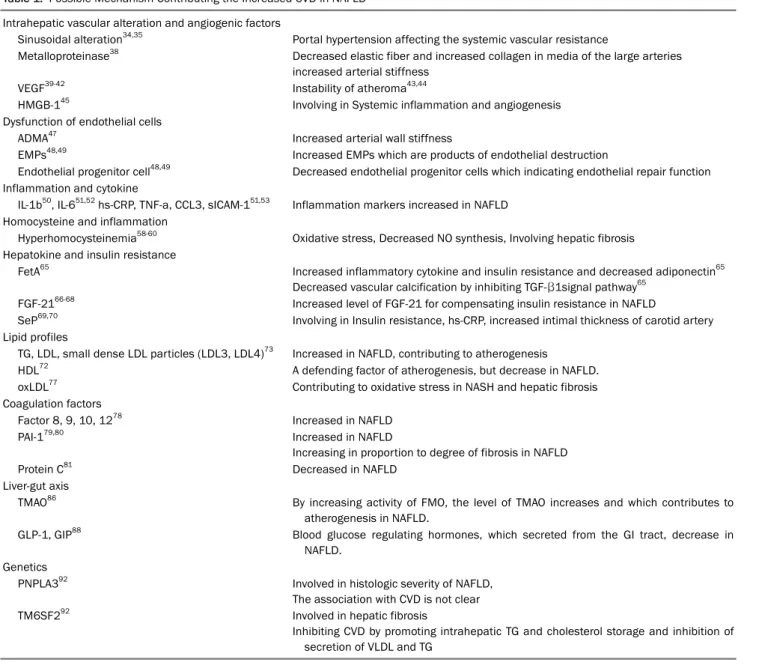
Table 1. Possible Mechanism Contributing the Increased CVD in NAFLD Intrahepatic vascular alteration and angiogenic factors
Sinusoidal alteration34,35 Portal hypertension affecting the systemic vascular resistance
Metalloproteinase38 Decreased elastic fiber and increased collagen in media of the large arteries increased arterial stiffness
VEGF39-42 Instability of atheroma43,44
HMGB-145 Involving in Systemic inflammation and angiogenesis
Dysfunction of endothelial cells
ADMA47 Increased arterial wall stiffness
EMPs48,49 Increased EMPs which are products of endothelial destruction
Endothelial progenitor cell48,49 Decreased endothelial progenitor cells which indicating endothelial repair function Inflammation and cytokine
IL-1b50, IL-651,52 hs-CRP, TNF-a, CCL3, sICAM-151,53 Inflammation markers increased in NAFLD Homocysteine and inflammation
Hyperhomocysteinemia58-60 Oxidative stress, Decreased NO synthesis, Involving hepatic fibrosis Hepatokine and insulin resistance
FetA65 Increased inflammatory cytokine and insulin resistance and decreased adiponectin65 Decreased vascular calcification by inhibiting TGF-β1signal pathway65
FGF-2166-68 Increased level of FGF-21 for compensating insulin resistance in NAFLD
SeP69,70 Involving in Insulin resistance, hs-CRP, increased intimal thickness of carotid artery
Lipid profiles
TG, LDL, small dense LDL particles (LDL3, LDL4)73 Increased in NAFLD, contributing to atherogenesis
HDL72 A defending factor of atherogenesis, but decrease in NAFLD.
oxLDL77 Contributing to oxidative stress in NASH and hepatic fibrosis
Coagulation factors
Factor 8, 9, 10, 1278 Increased in NAFLD
PAI-179,80 Increased in NAFLD
Increasing in proportion to degree of fibrosis in NAFLD
Protein C81 Decreased in NAFLD
Liver-gut axis
TMAO86 By increasing activity of FMO, the level of TMAO increases and which contributes to atherogenesis in NAFLD.
GLP-1, GIP88 Blood glucose regulating hormones, which secreted from the GI tract, decrease in NAFLD.
Genetics
PNPLA392 Involved in histologic severity of NAFLD,
The association with CVD is not clear
TM6SF292 Involved in hepatic fibrosis
Inhibiting CVD by promoting intrahepatic TG and cholesterol storage and inhibition of secretion of VLDL and TG
ADMA, asymmetric dimethyl arginine; CCL3, Chemokine (C-C motif) ligand 3; CVD, cardiovascular disease; EMPs, endothelial microparticles; FetA, fetuin-A; FGF21, fibroblast growth factor 21; FMO, flavin monooxygenase; GI, gastrointestinal; GIP, gastric inhibitory protein; GLP-1, glucagon-like peptide; HDL, high-density lipoproteins; HMGB-1, high mobility group box 1; hs-CRP, high sensitivity C-reactive protein; IL-1b, interleukin 1b; IL-6, interleukin 6; LDL, low-density lipoproteins; NAFLD, non-alcoholic fatty liver disease; NASH, non-alcoholic steatohepatitis; NO, nitric oxide; oxLDL, oxidized low-density lipoprotein; PAI-1, plasminogen activator inhibitor 1; PNPLA3, patatin-like phospholipase domain containing protein 3; SeP, selenoprotein P; sICAM, soluble intercellular adhesion molecule-1; TG, triglyceride; TGF-β, transforming growth factor beta; TM6SF2, transmembrane 6 superfamily member 2; TMAO, trimethylamine-N-Oxide; TNF-a, tumor necrosis factor a; VEGF, vascular endothelial growth factor; VLDL, very low-density lipoproteins.
NAFLD 환자군에서 보이는 식후 지질 변화는 혈관의 죽상 경화를 악화시키는 요인으로, 식후에 chylomicron remnants, LDL, VLDLs 및 TG 증가와 HDL의 감소가 더욱 뚜렷하게 나타
나며,74-76 NASH에서 관찰되는 산화된 저밀도 지질단백(oxidized
low density lipoprotein)은 산화 스트레스를 악화시키는 요인으로 간섬유화와 간손상을 유발하는 악순환이 발생하 게 된다.77
7) 응고 장애
간은 다양한 응고 관련 물질의 주요 생산 장기로서, NAFLD에 서 항응고인자들의 혈중 농도 변화가 발생한다. 대부분의 연구 에서, 응고유발물질(pro-thrombotic factor)들이 증가하는 경향 을 보였으며, factor 8, 9, 10, 12 등의 응고인자들의 혈중 농도 상승을 보였다.78 Plasminogen activator inhibitor-1 (PAI-1) 는 NASH와 NAFLD에서 증가하는 양상을 보였으며, 조직학적 섬
유화 정도와 비례하는 양상을 보였다.79,80또한 protein C의 활성 도 감소 및 factor 8의 증가로 인해 과응고성(hypercoagulability) 을 나타낼 수 있다는 연구도 발표되었다.81 그러나 이러한 과 응고성을 나타내는 혈중 지표들이 실제 CVD의 증가를 일으 키는지에 대해 아직까지 대규모 연구가 없는 실정으로, 추가 적인 연구가 필요할 것으로 보인다.
8) Liver-gut axis
장관 내에 미생물의 변화는 NAFLD에서 관찰되며, 혈관의 죽상화 및 심근경색과 심부전 등과 관련이 있다는 사실이 알 려져 있다.82-85 위장관 내에 서식하는 미생물들은 위장관 벽을 통해 다양한 물질을 혈관 내로 분비하는데, 그중 잘 알려진 것이 2차성 담즙의 일종인 trimethylamine (TMA)과 short chain fatty acids 등이다. 이러한 물질들은 인슐린 저항성과 생체 대사에 관여함으로써 NAFLD와 CVD에 영향을 줄 수 있다.
Trimethylamine–N-oxidase (TMAO)는 간 내에서 choline, L-carnitine, phosphatidylcholine을 기질로 하여, TMA에 flavin monoxygenase (FMO)라는 효소에 의해 생성되는데, 이렇게 생성된 TMAO는 혈관의 죽상화에 기여한다. 쥐를 이 용한 실험에서 FMO가 간 내에 있는 중성지방에 비례하는 것 이 밝혀졌고,86 이후 NASH 동물모델에서도 입증되었는데,87 NAFLD/NASH 환자에서 FMO의 활성 증가로 인한 TMAO 의 생성 증가로 인해 심혈관 질환의 위험이 증가할 수 있으며, 이와 관련하여 위장관 내에 미생물의 변화가 영향을 줄 수 있을 것으로 보인다.
최근 새로운 당뇨병 치료제 기전과 관련되어 부각된 incretin은 식후 위장관에서 분비하는 혈당 조절 호르몬의 일 종으로 glucagon-like peptide-1 (GLP-1), gastric inhibitory protein (GIP) 등이 있다. NAFLD군에서 감소하는 것이 알려 져 있으며,88 치료적 약제 사용 시에 NASH를 호전시켰다는 결과가 보고되고 있다.89
9) 유전자
현재까지 다양한 연구에서 밝혀진 NAFLD 관련 유전인자로 는 patatin-like phospholipase domain containing protein 3 (PNPLA3)과 transmembrane 6 superfamily member 2 (TM6SF2)가 대표적이다. PNPLA3 rs738409 유전자 변이는 NAFLD 환자의 조직학적 중증도와 관련이 있으며,90 중성지 방의 대사와 관련될 것으로 추정된다. NAFLD의 중증도와 관 련이 있으며, 간세포암에 치료적 타깃으로 연구되고 있다.91 다만, 현재까지 심혈관계 질환과의 연관성에 대해서는 명확히 밝혀진 바는 없다.
TM6SF2는 NAFLD에서 섬유화와 관련이 있다.92 이 유전
자의 돌연변이는 간 내에 중성지방 및 콜레스테롤의 침착을 유발하지만,93 역설적이게도 VLDLs와 혈관 내에 TG 분비를 막아 혈관 내에 저농도를 유지하게 함으로써 CVD에는 도움 을 준다.94
NAFLD에 대한 쌍생아 연구 및 인종 차이에 대한 연구 등 을 통해 문헌에 따라 18-50%까지 유전적 관련성이 있는 것으 로 여겨지고 있으나,95,96 최근의 쌍생아 연구에서 이러한 유전 적 요인이 NAFLD의 발현과 심혈관 질환의 위험과 직접적인 연관성에 대한 입증에는 실패한 상태로 아직까지는 논쟁의 여 지가 있다.97
결 론
서구화된 식생활과 더불어 국내에서도 NAFLD의 유병률 이 꾸준히 증가하고 있으며, 심혈관계 질환은 NAFLD 환자의 주요 사망 원인으로 알려져 있다. NAFLD는 과거 대사증후군 의 간 내 표현형으로 여겨지며, 독립적인 역할과 그 중요성이 간과된 측면이 있었으나 최근 다양한 코호트 연구 및 메타분 석을 통해 독립적인 심혈관계 위험인자로서의 측면이 강조되 고 있는 상태이다.
NAFLD와 심혈관 질환과 관련성의 기저에는 다양한 메커 니즘이 있다. 유전적 요인을 포함하여, liver-gut axis와 전신 인슐린 저항성과 관련된 다양한 hepatokine, 염증 반응과 산 화 스트레스로 인한 내피세포의 기능 저하와 혈관 내의 구조 적 변화 및 혈중 응고인자의 변화 등이 상호 작용하는 것으로 보이며, 향후 추가적인 연구를 통해 좀 더 명확해질 것으로 기대한다(Table 1).
REFERENCES
1. Ahmed A, Wong RJ, Harrison SA. Nonalcoholic fatty liver disease review: diagnosis, treatment, and outcomes. Clin Gastroenterol Hepatol 2015;13:2062-2070.
2. Angulo P. Nonalcoholic fatty liver disease. N Engl J Med 2002;
346:1221-1231.
3. de Alwis NM, Day CP. Non-alcoholic fatty liver disease: the mist gradually clears. J Hepatol 2008;48 Suppl 1:S104-S112.
4. Kotronen A, Yki-Järvinen H. Fatty liver: a novel component of the metabolic syndrome. Arterioscler Thromb Vasc Biol 2008;28:
27-38.
5. Marchesini G, Moscatiello S, Di Domizio S, Forlani G. Obesity-as- sociated liver disease. J Clin Endocrinol Metab 2008;93(11 Suppl 1):S74-S80.
6. Bae JC, Cho YK, Lee WY, et al. Impact of nonalcoholic fatty liver disease on insulin resistance in relation to HbA1c levels in non- diabetic subjects. Am J Gastroenterol 2010;105:2389-2395.
7. Choi SY, Kim D, Kim HJ, et al. The relation between non-alcoholic
fatty liver disease and the risk of coronary heart disease in Koreans. Am J Gastroenterol 2009;104:1953-1960.
8. Kim D, Choi SY, Park EH, et al. Nonalcoholic fatty liver disease is associated with coronary artery calcification. Hepatology 2012;
56:605-613.
9. Musso G, Cassader M, Gambino R. Diagnostic accuracy of adi- pose insulin resistance index and visceral adiposity index for pro- gressive liver histology and cardiovascular risk in nonalcoholic fatty liver disease. Hepatology 2012;56:788-789.
10. Nestel PJ, Mensink RP. Perspective: nonalcoholic fatty liver dis- ease and cardiovascular risk. Curr Opin Lipidol 2013;24:1-3.
11. Brea A, Mosquera D, Martín E, Arizti A, Cordero JL, Ros E.
Nonalcoholic fatty liver disease is associated with carotid athero- sclerosis: a case-control study. Arterioscler Thromb Vasc Biol 2005;25:1045-1050.
12. Fracanzani AL, Burdick L, Raselli S, et al. Carotid artery in- tima-media thickness in nonalcoholic fatty liver disease. Am J Med 2008;121:72-78.
13. Kim HC, Kim DJ, Huh KB. Association between nonalcoholic fatty liver disease and carotid intima-media thickness according to the presence of metabolic syndrome. Atherosclerosis 2009;
204:521-525.
14. Targher G, Bertolini L, Padovani R, et al. Relations between car- otid artery wall thickness and liver histology in subjects with non- alcoholic fatty liver disease. Diabetes Care 2006;29:1325-1330.
15. Targher G, Bertolini L, Padovani R, Zenari L, Zoppini G, Falezza G. Relation of nonalcoholic hepatic steatosis to early carotid atherosclerosis in healthy men: role of visceral fat accumulation.
Diabetes Care 2004;27:2498-2500.
16. Volzke H, Robinson DM, Kleine V, et al. Hepatic steatosis is asso- ciated with an increased risk of carotid atherosclerosis. World J Gastroenterol 2005;11:1848-1853.
17. Bhatia LS, Curzen NP, Calder PC, Byrne CD. Non-alcoholic fatty liver disease: a new and important cardiovascular risk factor?
Eur Heart J 2012;33:1190-1200.
18. Oni ET, Agatston AS, Blaha MJ, et al. A systematic review: burden and severity of subclinical cardiovascular disease among those with nonalcoholic fatty liver; should we care? Atherosclerosis 2013;230:258-267.
19. Sung KC, Wild SH, Kwag HJ, Byrne CD. Fatty liver, insulin resist- ance, and features of metabolic syndrome: relationships with coronary artery calcium in 10,153 people. Diabetes Care 2012;
35:2359-2364.
20. Davignon J, Ganz P. Role of endothelial dysfunction in ather- osclerosis. Circulation 2004;109(23 Suppl 1):III27- III32.
21. Pacifico L, Anania C, Martino F, et al. Functional and morpho- logical vascular changes in pediatric nonalcoholic fatty liver disease. Hepatology 2010;52:1643-1651.
22. Villanova N, Moscatiello S, Ramilli S, et al. Endothelial dysfunc- tion and cardiovascular risk profile in nonalcoholic fatty liver disease. Hepatology 2005;42:473-480.
23. Bonapace S, Perseghin G, Molon G, et al. Nonalcoholic fatty liver disease is associated with left ventricular diastolic dysfunction in patients with type 2 diabetes. Diabetes Care 2012;35:389- 395.
24. Fallo F, Dalla Pozza A, Sonino N, et al. Non-alcoholic fatty liver dis-
ease is associated with left ventricular diastolic dysfunction in essential hypertension. Nutr Metab Cardiovasc Dis 2009;19:
646-653.
25. Goland S, Shimoni S, Zornitzki T, et al. Cardiac abnormalities as a new manifestation of nonalcoholic fatty liver disease: echo- cardiographic and tissue doppler imaging assessment. J Clin Gastroenterol 2006;40:949-955.
26. Hallsworth K, Hollingsworth KG, Thoma C, et al. Cardiac structure and function are altered in adults with non-alcoholic fatty liver disease. J Hepatol 2013;58:757-762.
27. Lautamäki R, Borra R, Iozzo P, et al. Liver steatosis coexists with myocardial insulin resistance and coronary dysfunction in pa- tients with type 2 diabetes. Am J Physiol Endocrinol Metab 2006;291:E282-E290.
28. Lazo M, Hernaez R, Bonekamp S, et al. Non-alcoholic fatty liver disease and mortality among US adults: prospective cohort study. BMJ 2011;343:d6891.
29. Stepanova M, Younossi ZM. Independent association between nonalcoholic fatty liver disease and cardiovascular disease in the US population. Clin Gastroenterol Hepatol 2012;10:646- 650.
30. Targher G, Bertolini L, Padovani R, et al. Prevalence of non- alcoholic fatty liver disease and its association with car- diovascular disease among type 2 diabetic patients. Diabetes Care 2007;30:1212-1218.
31. Zhou YJ, Li YY, Nie YQ, Huang CM, Cao CY. Natural course of non- alcoholic fatty liver disease in southern China: a prospective co- hort study. J Dig Dis 2012;13:153-160.
32. Wu S, Wu F, Ding Y, Hou J, Bi J, Zhang Z. Association of non-alco- holic fatty liver disease with major adverse cardiovascular events: a systematic review and meta-analysis. Sci Rep 2016;6:
33386.
33. Ekstedt M, Hagström H, Nasr P, et al. Fibrosis stage is the stron- gest predictor for disease-specific mortality in NAFLD after up to 33 years of follow-up. Hepatology 2015;61:1547-1554.
34. Farrell GC, Teoh NC, McCuskey RS. Hepatic microcirculation in fatty liver disease. Anat Rec (Hoboken) 2008;291:684-692.
35. Francque S, Laleman W, Verbeke L, et al. Increased intrahepatic resistance in severe steatosis: endothelial dysfunction, vaso- constrictor overproduction and altered microvascular architecture.
Lab Invest 2012;92:1428-1439.
36. Coulon S, Legry V, Heindryckx F, et al. Role of vascular endothelial growth factor in the pathophysiology of nonalcoholic steatohepa- titis in two rodent models. Hepatology 2013;57:1793-1805.
37. Francque S, Verrijken A, Mertens I, et al. Noncirrhotic human non- alcoholic fatty liver disease induces portal hypertension in rela- tion to the histological degree of steatosis. Eur J Gastroenterol Hepatol 2010;22:1449-1457.
38. Gkaliagkousi E, Douma S. The pathogenesis of arterial stiffness and its prognostic value in essential hypertension and car- diovascular diseases. Hippokratia 2009;13:70-75.
39. Cayón A, Crespo J, Guerra AR, Pons-Romero F. Gene expression in obese patients with non-alcoholic steatohepatitis. Rev Esp Enferm Dig 2008;100:212-218.
40. Coulon S, Francque S, Colle I, et al. Evaluation of inflammatory and angiogenic factors in patients with non-alcoholic fatty liver
disease. Cytokine 2012;59:442-449.
41. Tarantino G, Conca P, Pasanisi F, et al. Could inflammatory mark- ers help diagnose nonalcoholic steatohepatitis? Eur J Gastroenterol Hepatol 2009;21:504-511.
42. Yilmaz Y, Yonal O, Kurt R, et al. Circulating levels of vascular endo- thelial growth factor A and its soluble receptor in patients with bi- opsy-proven nonalcoholic fatty liver disease. Arch Med Res 2011;42:38-43.
43. Khurana R, Simons M, Martin JF, Zachary IC. Role of angio- genesis in cardiovascular disease: a critical appraisal. Circulation 2005;112:1813-1824.
44. Ylä-Herttuala S, Rissanen TT, Vajanto I, Hartikainen J. Vascular endothelial growth factors: biology and current status of clinical applications in cardiovascular medicine. J Am Coll Cardiol 2007;49:1015-1026.
45. Elsheikh E, Younoszai Z, Otgonsuren M, Hunt S, Raybuck B, Younossi ZM. Markers of endothelial dysfunction in patients with non-alcoholic fatty liver disease and coronary artery disease. J Gastroenterol Hepatol 2014;29:1528-1534.
46. Vanhoutte PM. Endothelial dysfunction: the first step toward cor- onary arteriosclerosis. Circ J 2009;73:595-601.
47. Kasumov T, Edmison JM, Dasarathy S, Bennett C, Lopez R, Kalhan SC. Plasma levels of asymmetric dimethylarginine in pa- tients with biopsy-proven nonalcoholic fatty liver disease.
Metabolism 2011;60:776-781.
48. Bruyndonckx L, Hoymans VY, Van Craenenbroeck AH, et al.
Assessment of endothelial dysfunction in childhood obesity and clinical use. Oxid Med Cell Longev 2013;2013:174782.
49. Chiang CH, Huang PH, Chung FP, et al. Decreased circulating en- dothelial progenitor cell levels and function in patients with non- alcoholic fatty liver disease. PLoS One 2012;7:e31799.
50. Vonghia L, Magrone T, Verrijken A, et al. Peripheral and hepatic vein cytokine levels in correlation with non-alcoholic fatty liver disease (NAFLD)-related metabolic, histological, and haemody- namic features. PLoS One 2015;10:e0143380.
51. Hamirani YS, Katz R, Nasir K, et al. Association between in- flammatory markers and liver fat: The Multi-Ethnic Study of Atherosclerosis. J Clin Exp Cardiolog 2014;5. pii: 1000344.
52. Wieckowska A, Papouchado BG, Li Z, Lopez R, Zein NN, Feldstein AE. Increased hepatic and circulating interleukin-6 levels in hu- man nonalcoholic steatohepatitis. Am J Gastroenterol 2008;
103:1372-1379.
53. du Plessis J, van Pelt J, Korf H, et al. Association of adipose tissue inflammation with histologic severity of nonalcoholic fatty liver disease. Gastroenterology 2015;149:635-648.e14.
54. Ganguly P, Alam SF. Role of homocysteine in the development of cardiovascular disease. Nutr J 2015;14:6.
55. Santilli F, Davi G, Patrono C. Homocysteine, methylenetetrahy- drofolate reductase, folate status and atherothrombosis: a mechanistic and clinical perspective. Vascul Pharmacol 2016;
78:1-9.
56. de Carvalho SC, Muniz MT, Siqueira MD, et al. Plasmatic higher levels of homocysteine in non-alcoholic fatty liver disease (NAFLD). Nutr J 2013;12:37.
57. Franco Brochado MJ, Domenici FA, Candolo Martinelli Ade L, Zucoloto S, de Carvalho da Cunha SF, Vannucchi H. Methylenetet-
rahydrofolate reductase gene polymorphism and serum homo- cysteine levels in nonalcoholic fatty liver disease. Ann Nutr Metab 2013;63:193-199.
58. Bravo E, Palleschi S, Aspichueta P, et al. High fat diet-induced non alcoholic fatty liver disease in rats is associated with hyper- homocysteinemia caused by down regulation of the trans- sulphuration pathway. Lipids Health Dis 2011;10:60.
59. Kalhan SC, Edmison J, Marczewski S, et al. Methionine and pro- tein metabolism in non-alcoholic steatohepatitis: evidence for lower rate of transmethylation of methionine. Clin Sci (Lond) 2011;121:179-189.
60. Pacana T, Cazanave S, Verdianelli A, et al. Dysregulated hepatic methionine metabolism drives homocysteine elevation in di- et-induced nonalcoholic fatty liver disease. PLoS One 2015;
10:e0136822.
61. Distrutti E, Mencarelli A, Santucci L, et al. The methionine con- nection: homocysteine and hydrogen sulfide exert opposite ef- fects on hepatic microcirculation in rats. Hepatology 2008;47:
659-667.
62. Stefan N, Häring HU. The role of hepatokines in metabolism. Nat Rev Endocrinol 2013;9:144-152.
63. Hennige AM, Staiger H, Wicke C, et al. Fetuin-A induces cytokine expression and suppresses adiponectin production. PLoS One 2008;3:e1765.
64. Sato M, Kamada Y, Takeda Y, et al. Fetuin-A negatively correlates with liver and vascular fibrosis in nonalcoholic fatty liver disease subjects. Liver Int 2015;35:925-935.
65. Jensen MK, Bartz TM, Mukamal KJ, et al. Fetuin-A, type 2 dia- betes, and risk of cardiovascular disease in older adults: the car- diovascular health study. Diabetes Care 2013;36:1222-1228.
66. Domouzoglou EM, Naka KK, Vlahos AP, et al. Fibroblast growth factors in cardiovascular disease: the emerging role of FGF21.
Am J Physiol Heart Circ Physiol 2015;309:H1029-H1038.
67. Dushay J, Chui PC, Gopalakrishnan GS, et al. Increased fibroblast growth factor 21 in obesity and nonalcoholic fatty liver disease.
Gastroenterology 2010;139:456-463.
68. Li H, Fang Q, Gao F, et al. Fibroblast growth factor 21 levels are increased in nonalcoholic fatty liver disease patients and are cor- related with hepatic triglyceride. J Hepatol 2010;53:934-940.
69. Choi HY, Hwang SY, Lee CH, et al. Increased selenoprotein p levels in subjects with visceral obesity and nonalcoholic fatty liver disease. Diabetes Metab J 2013;37:63-71.
70. Yang SJ, Hwang SY, Choi HY, et al. Serum selenoprotein P levels in patients with type 2 diabetes and prediabetes: implications for insulin resistance, inflammation, and atherosclerosis. J Clin Endocrinol Metab 2011;96:E1325-E1329.
71. Lim J, Park HS, Lee SK, Jang YJ, Lee YJ, Heo Y. Longitudinal changes in serum levels of angiopoietin-like protein 6 and sele- noprotein P after gastric bypass surgery. Obes Surg 2016;26:
825-832.
72. Alkhouri N, Tamimi TA, Yerian L, Lopez R, Zein NN, Feldstein AE.
The inflamed liver and atherosclerosis: a link between histologic severity of nonalcoholic fatty liver disease and increased car- diovascular risk. Dig Dis Sci 2010;55:2644-2650.
73. Sonmez A, Nikolic D, Dogru T, et al. Low- and high-density lip- oprotein subclasses in subjects with nonalcoholic fatty liver
disease. J Clin Lipidol 2015;9:576-582.
74. Cassader M, Gambino R, Musso G, et al. Postprandial trigly- ceride-rich lipoprotein metabolism and insulin sensitivity in non- alcoholic steatohepatitis patients. Lipids 2001;36:1117-1124.
75. Roche HM, Gibney MJ. The impact of postprandial lipemia in ac- celerating atherothrombosis. J Cardiovasc Risk 2000;7:317- 324.
76. Siddiqui MS, Fuchs M, Idowu MO, et al. Severity of nonalcoholic fatty liver disease and progression to cirrhosis are associated with atherogenic lipoprotein profile. Clin Gastroenterol Hepatol 2015;13:1000-1008.e3.
77. Musso G, Gambino R, De Michieli F, et al. Association of liver dis- ease with postprandial large intestinal triglyceride-rich lipoprotein accumulation and pro/antioxidant imbalance in normolipidemic non-alcoholic steatohepatitis. Ann Med 2008;40:383-394.
78. Kotronen A, Joutsi-Korhonen L, Sevastianova K, et al. Increased coagulation factor VIII, IX, XI and XII activities in non-alcoholic fat- ty liver disease. Liver Int 2011;31:176-183.
79. Barbato A, Iacone R, Tarantino G, et al. Relationships of PAI-1 lev- els to central obesity and liver steatosis in a sample of adult male population in southern Italy. Intern Emerg Med 2009;4:315-323.
80. Verrijken A, Francque S, Mertens I, et al. Prothrombotic factors in histologically proven nonalcoholic fatty liver disease and non- alcoholic steatohepatitis. Hepatology 2014;59:121-129.
81. Tripodi A, Fracanzani AL, Primignani M, et al. Procoagulant im- balance in patients with non-alcoholic fatty liver disease. J Hepatol 2014;61:148-154.
82. Abu-Shanab A, Quigley EM. The role of the gut microbiota in non- alcoholic fatty liver disease. Nat Rev Gastroenterol Hepatol 2010;7:691-701.
83. Aron-Wisnewsky J, Clément K. The gut microbiome, diet, and links to cardiometabolic and chronic disorders. Nat Rev Nephrol 2016;12:169-181.
84. Wong VW, Tse CH, Lam TT, et al. Molecular characterization of the fecal microbiota in patients with nonalcoholic steatohepatitis--a longitudinal study. PLoS One 2013;8:e62885.
85. Zhu L, Baker SS, Gill C, et al. Characterization of gut microbiomes in nonalcoholic steatohepatitis (NASH) patients: a connection between endogenous alcohol and NASH. Hepatology 2013;57:
601-609.
86. Hui ST, Parks BW, Org E, et al. The genetic architecture of NAFLD among inbred strains of mice. Elife 2015;4:e05607.
87. Hebbard L, George J. Animal models of nonalcoholic fatty liver disease. Nat Rev Gastroenterol Hepatol 2011;8:35-44.
88. Bernsmeier C, Meyer-Gerspach AC, Blaser LS, et al. Glucose-in- duced glucagon-like peptide 1 secretion is deficient in patients with non-alcoholic fatty liver disease. PLoS One 2014;9:e87488.
89. Wang Y, Parlevliet ET, Geerling JJ, et al. Exendin-4 decreases liver inflammation and atherosclerosis development simultaneously by reducing macrophage infiltration. Br J Pharmacol 2014;171:
723-734.
90. Romeo S, Kozlitina J, Xing C, et al. Genetic variation in PNPLA3 confers susceptibility to nonalcoholic fatty liver disease. Nat Genet 2008;40:1461-1465.
91. Liu YL, Patman GL, Leathart JB, et al. Carriage of the PNPLA3 rs738409 C >G polymorphism confers an increased risk of non-alcoholic fatty liver disease associated hepatocellular carcinoma. J Hepatol 2014;61:75-81.
92. Liu YL, Reeves HL, Burt AD, et al. TM6SF2 rs58542926 influen- ces hepatic fibrosis progression in patients with non-alcoholic fatty liver disease. Nat Commun 2014;5:4309.
93. Kozlitina J, Smagris E, Stender S, et al. Exome-wide association study identifies a TM6SF2 variant that confers susceptibility to nonalcoholic fatty liver disease. Nat Genet 2014;46:352-356.
94. Kahali B, Liu YL, Daly AK, Day CP, Anstee QM, Speliotes EK.
TM6SF2: catch-22 in the fight against nonalcoholic fatty liver dis- ease and cardiovascular disease? Gastroenterology 2015;148:
679-684.
95. Anstee QM, Day CP. The genetics of nonalcoholic fatty liver dis- ease: spotlight on PNPLA3 and TM6SF2. Semin Liver Dis 2015;
35:270-290.
96. Tarnoki AD, Tarnoki DL, Bata P, et al. Heritability of non-alcoholic fatty liver disease and association with abnormal vascular pa- rameters: a twin study. Liver Int 2012;32:1287-1293.
97. Loomba R, Schork N, Chen CH, et al. Heritability of hepatic fib- rosis and steatosis based on a prospective twin study.
Gastroenterology 2015;149:1784-1793.