급성 또는 만성 통증이 있을 때 사용할 수 있는 약제의 종류 는 1) 단순진통제, 2) 비스테로이드성 소염진통제(nonsteroidal antiinflammatory drug, NSAID), 3) 마약성 진통제, 4) 부신피질 호르몬제와 5) 정신신경과적 약물로서 항우울제, 항경련제 등 을 거론할 수 있다. 이러한 약제들은 통증을 유발하는 원인 질 환, 환자의 임상 증상의 정도와 동반 질환에 따라 단독 또는 병합 요법으로 사용할 수 있다.
통증에 대한 단계적 치료법에 따르면 경도의 통증에는 비마약성 진통제 +/- adjuvant를 우선 사용한다. 중등도의 통증에는 약한 마약성 진통제를 사용하고 자주 비마약성 진통제를 병합한다. 심한 통증에는 강력한 마약성 진통제 와 비마약성 진통제 또는 adjuvant drug를 사용하는 것이 좋 다고 권장되고 있다.
저자는 본 논문에서 임상에서 통증 환자의 치료에 널리 사용되고 있는 비스테로이드성 소염진통제와 단순 진통제 의 장․단점 및 사용에 관하여 설명하고자 한다.
1. 단순진통제
단순한 진통제로서 가장 많이 알려진 것은 acetaminophen 이다. 주로 경증이나 중등도의 통증을 가진 환자에 우선 사 용하며, 증상에 따라 하루 4.0 g까지 사용할 수 있다. 자세한 작용 기전은 아직 잘 알려져 있지는 않으나 중추신경에 직 접 작용하는 것으로 보고되고 있고, 소염진통제를 사용할 때 동반되는 상부 위장관 출혈이나 천공과 같은 심각한 위 장관 부작용을 염려하지 않고 사용할 수 있는 장점이 있다.
그러나 간 독성을 유발하는 가장 흔한 약제가 acetamino- phen이며 10 g 이상에서 간독성이 보고되어 있고, 간의 장 애가 있는 환자나 알코올중독자는 식사를 하지 않고 과량 의 약제를 복용할 수도 있으므로 간독성의 빈도가 높아지 므로 약제의 용량을 줄여야 한다.1) 그러나 이 약제도 궤양 과 동반되지 않은 상부위장관의 부작용, 즉 non-ulcer dys- pepsia는 비슷한 빈도로 나타나므로 약제를 과량으로 투여 할 때 주의를 환기시킬 필요가 있다.2) 증상이 심한 환자는 약한 마약성 진통제인 codeine 등과 함께 사용하면 증상의 개선을 도모할 수 있다.
2. 비스테로이드성 소염진통제
NSAIDs는 현재 전 세계적으로 가장 많이 처방되는 약물 중의 하나이며, 특히 근골격계의 증상이 많은 60세 이상의 노인에서 처방되는 경우가 많다. 가장 흔한 적응증은 여러 가지 관절통과 관절염에 의한 통증이며, 기타 수술 후 통증 관리, 근육통, 암 환자의 통증, 신경통 등에 사용하기도 한 다.3)
NSAIDs의 대표적인 작용은 항염작용, 진통작용, 그리고 해열작용이다. NSAIDs는 주로 cyclooxygenase의 기능을 억
통증 환자에서 소염진통제의 선택
한양대학교 류마티스병원 류마티스내과 유 대 현
N S A ID s in the Treatm ent of Pain
Dae-Hyun Yoo, M.D.
The Hospital for Rheumatic Diseases, Hanyang University
A few classes of drugs have been utilized for the control of pain depending upon the degree or severity of pain. Non- steroidal antiinflammatory drugs (NSAIDs), simple analgesics, opioids analgesics, and adjuvant drugs are commonly pre- scribed by physicians. Here, the characteristics and clinical guideline of NSAIDs use are reviewed.
NSAIDs can be classified by their chemical class, half life, and preference to COX-I/II inhibition. exert clinical effects by their analgesic, antipyretic, and antiinflammatory actions. Most of NSAIDs belong to weak acid except nabumetone, and in- hibit prostaglandin synthesis by means of inhibiting cyclo- oxygenase (COX). COX has two isoenzyme at least, and two isozymes have different time dependent activation, distribution, response to noxious stimuli. Most of the adverse reactions could be derived from inhibition of physiologic function of prostaglndins, however lately developed COX-II specific inhi- bitors could reduce side reactions including gastrointestinal toxicity even though they still have limitations in renal, car- diovascular, neurologic system. (J Korean Assoc Pain Med 2002;1:9-15)
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ Key Words: NSAID, Pain, Toxicity, Prostaglandin
접수일: 2002년 1월 15일, 게재승인일: 2002년 2월 28일 책임저자: 유대현, 서울시 성동구 행당동 17
ꂕ 133-792, 한양대학교 류마티스병원 류마티스내과 Tel: 02-2290-9202, Fax: 02-2298-8231
E-mail: [email protected]
제하여 결국 prostaglandin (PG)의 생성을 억제함으로써 항 염과 진통효과를 나타낸다고 알려져 있다.4) 아스피린이나 다른 NSAIDs와의 비교는 커다란 차이가 없으나 최근에 개 발된 NSAIDs가 최고용량에서 아스피린보다 부작용이 적 다. 거의 모든 NSAIDs는 항염작용을 나타내는 용량보다 적 은 용량에서 통증을 억제하는 효과가 있는데, 이것은 NSAIDs가 PG의 합성과 분비를 억제하여 화학적 매개물에 대한 통증 수용체의 민감성을 방해하는 것으로 추측된다.
그러나 인체에서 항상성의 유지와 관련된 PG의 합성을 억 제하면 그 결핍에 의해 여러 가지 부작용이 필연적으로 발 생하며, 예를 들면 위장관 궤양의 발생, 신장의 혈류 조절 장애와 순환장애, 그리고 혈액응고 장애 등을 거론할 수 있 다.5)
PG와 연관된 작용 기전 이외에 NSAID의 다른 작용기전 은 다음과 같다. PG억제에 충분한 양의 아스피린이 해열과 진통작용을 나타내지만 염증을 억제시키지 못하며, PG을 억제하지 못하는 sodium salicylate가 아스피린과 비슷한 항 염작용을 갖는다. 이는 PG와 무관한 소염진통제의 작용 기 전이 존재한다는 것을 암시하는 증거이다. Diclofenac과 indomethacin 등 여러 가지 NSAIDs가 arachidonic acid의 또 다른 대사진로인 lipooxygenase를 억제하여 백혈구와 활막 세포에서 leukotriene과 PG의 생산을 억제한다. 이외에도 호 중구에서 superoxide생산 억제, 단핵구에서 phospholipase C 의 억제, 호중구의 결집 억제, 호중구 세포막에서 단백질-단 백질 상호작용 억제 등이 NSAIDs의 또 다른 작용기전으로 제시되었다.5)
1) NSAIDs의 분류: NSAIDs는 화학적 구조, COX-I/II에 대한 특이성, 반감기 등에 따라 분류할 수 있다.
(1) 화학적 구조에 따른 분류; 소염진통제는 Table 1과 같
이 화학적으로 크게 carboxylic acid 계열, enolic acid 계열, nonacidic compound로 구분된다. 약제의 다양한 생화학적 특성들이 약물의 역동성에 영향을 주고, 효과와 부작용의 차이점은 이에 기인한다. 예를 들어 lipid soluble한 keto- profen, naproxen, ibuprofen 등은 뇌에 영향을 주어서 인식이 나 감정의 변화를 일으키기도 한다. 대부분의 NSAIDs는 약 산성을 나타내는 유기산이다. 이와 같은 성질은 NSAIDs가 낮은 pH를 갖는 염증성 조직에 고농도로 분포하게 하는 데 중요하다. 그러나 반드시 산성인 것이 필수적인 것은 아니 며, 비산성 화합물인 nabumetone은 항염작용을 갖는 대표적 인 비산성 NSAID이다.
(2) COX에 대한 특이성에 따른 분류; Cyclooxygenase (COX)는 2가지 아형이 있고, COX-1은 어느 조직에서나 항 상 발현하는 반면, COX-II는 각종 성장 인자, 사이토카인 등에 의해서 monocyte, macrophage, endothelial cell, chond- rocyte, synovial cell, osteoblast 등에서 발현이 유도되므로, 주로 염증성 조직에서 발현이 증가한다.6,7) 그러나 COX-II 는 일부 뇌 세포(cortical neuron, hippocampus),8) pancreas islet cell,9) 신장의 juxtaglomerular apparatus의 macular densa나 tubular epithelial cell 등과 같은 조직에도 정상적으로 존재 한다. 동물 실험에서는 rat alveolar macrophage, peritoneal macrophage, bovine pulmonary artery endothelial cell 등에서 COX-I의 발현이 cytokine에 의해 영향을 받는다고 하였다.6) NSAIDs에 의한 부작용의 대부분은 항상성의 유지와 관 련이 있는 COX-I의 억제에 기인하며, 약제에 따라 COX-I/
COX-II 억제의 정도가 조금씩 다르다. 그러나 전통적인 NSAID는 생리적인 농도, 즉 COX-II를 억제하는 어떠한 농 도에서도 항상성의 유지와 연관된 COX-I을 반드시 억제하 게 되어 있으므로 이론적으론 부작용의 발생은 피할 수 없 다. 그러나 최근에는 치료 농도에서도 COX-I을 거의 억제 하지 않는 specific COX-II inhibitor가 개발되어 임상에서 사 용 중이다.
NSAID는 COX specificity에 따라 COX non-selective NSAID 로서 COX-I preferential, COX-I/II equivalent, COX-II prefer- ential로 구분할 수 있고, 최근에 개발된 COX-II specific NSAID로 분류할 수 있다. COX-I preferential한 약제는 indo- methacin, naproxen, piroxicam, aspirin, ibuprofen을 들 수 있 으며, COX-I/II equivalent한 약제는 diclofenac이 대표적이다.
COX-II preferential한 약제는 meloxicam, nimesulide, etodolac 을 거론할 수 있으며, 현재 시판 중인 specific COX-II inhib- itor는 celecoxib와 rofecoxib가 있다.
실제 임상에서 COX-II specific inhibitor를 사용하는 적응 증은 각종 관절염과 급성 통증 등이지만, 실제 임상에서 사 용할 때는 제약을 받는다. 현재 사용 중인 COX-II specific inhibitor는 위장관의 부작용은 현저하게 감소시킬 수 있으 Table 1. Classification of NSAIDs by Chemical Class
ꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧ
Enolic acid:
Pyrazolone: Phenylbutazone
Oxicam: Piroxicam, Tenoxicam, Meloxicam Nonacidic compound: Nabumetone
Carboxylic acid:
Salicylic acid & esters:
ASA, diflunisal, Salsalate, Na salicylate
Acetic acid: Phenylacetic acid: diclofenac, aceclofenac Carbo- and heterocyclic acid:
etodolac, indomethacin, sulindac, tolmetin, ketorolac Proprionic acid: ibuprofen, ketoprofen, oxaprozin,
naproxen, fenoprofen Fenamic acid: flufenamic, mefenamic
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
나, non-ulcer dyspepsia는 감소하기는 하지만 여전히 발생한 다. 아울러 이 약제도 궁극적으로는 소염진통제이기 때문 에 다른 소염진통제에서 나타나는 신장에 대한 효과,10) 중 추신경 효과, 고혈압 및 심혈관계에 대한 효과11,12) 등은 여 전히 존재한다는 사실을 기억해야 하겠다.
(3) 약제의 반감기에 따른 분류(Table 2); NSAIDs는 화학 구조식에 따라 분류할 수 있지만, 이들의 반감기에 따른 분 류를 이해하는 것이 도움이 될 수 있다. 반감기가 긴 약물은 하루에 한번 또는 두 번, 반감기가 짧은 약물은 4∼6시간마 다 투여하면 최대한의 효과를 얻을 수 있다.
① 반감기가 긴 약물: 반감기가 12시간 이상 되는 약물은 일일 1회 또는 2회 투여한다. 안정된 농도에 도달하기 위해 서는 반감기의 5배 정도의 시간이 소요되므로 대체로 3일 내지 수주 후에 일정한 농도에 도달하여 약물을 복용하는 중간에도 약물의 농도가 안정된다.
② 반감기가 짧은 약물: 6시간 이내의 반감기를 갖는 약 물들로 하루 3회 내지 4회 복용해야 하며, 일정한 농도에 24∼36시간 내에 도달하지만 투여 사이의 농도가 심하게 변동되는 단점이 있다. 그러나 현재는 많은 약제가 서방형 제제로 개발되어 있어서 약제의 투여를 자주 할 필요성은 적 어졌다.
2) 부작용: NSAIDs의 광범위한 사용과 이들의 약리작용으 로 인해 부작용의 발생은 불가피하다. 특정 부작용의 발생 은 약물에 따라 차이가 있지만 대체로 유사한 범주의 부작 용을 나타낸다. 대개 필요한 약리작용과 부작용은 약물의 농도에 따라 나타나므로 손익을 따져 처방하여야 한다. 중 요한 부작용은 위장관, 중추신경계, 조혈계, 신장, 피부, 그
리고 간 장애를 거론할 수 있다.
(1) 위장관; NSAIDs를 복용하는 환자들에서 가장 흔한 부 작용은 위장관 증상이다. 그러나, 많은 환자가 경험하는 소 화불량의 정도와 궤양의 발생 사이에는 연관성이 없으므로 문제가 임상적으로 심각한 것인지 판단하기 어렵다. 만성 적으로 NSAIDs를 사용하는 환자에서 궤양의 발생빈도는 15∼30%이다.13) NSAIDs사용에 의해 궤양 등의 합병증이 발생할 위험인자로는 Table 3과 같이 여성, 65세 이상의 고 령, 이전에 궤양이나 합병증의 병력이 있는 경우, 고농도 또 는 여러 가지의 NSAIDs를 사용한 경우, 부신피질 호르몬을 같이 사용하는 경우, 심한 전신 질환이 있는 환자, 항응고제 를 사용하는 환자 등이다. NSAIDs에 의한 위장관의 부작용 은 위나 십이지장에 국한되지 않으며, 소장이나 결장에서 도 발견할 수 있다.14)
약물치료에 의한 위장관 궤양의 이상적인 치료는 약물을 중단하는 것이나 급․만성 통증을 호소하는 환자에서는 어 려운 일이다. 따라서 궤양의 발생을 예방하는 데에 주력해 야 하는데 proton pump inhibitor인 omeprazole, PGE 유사체 인 misoprostol 등이 효과가 있다.15) 고용량의 famotidine이 효과가 있다는 보고도 있으나 비경제적이다. 최근에는 새 로이 개발된 COX-II inhibitor인 celecoxib, rofecoxib를 사용 하면 이런 약제를 병용할 필요가 없고 적어도 심각한 위장 관 부작용은 걱정하지 않고 사용할 수 있다.16)
(2) 간질환; 거의 모든 NSAIDs가 간 손상을 일으킬 수 있 는데, acetaminophen, diclofenac, sulindac의 경우 위험도가 높고, ibuprofen과 ketoprofen의 경우 위험도가 낮은 것으로 알려져 있다. 약물을 중단하거나 감량하면 일반적으로 transaminase의 수치가 정상화된다. 고령, 신 기능 장애, 다 량의 약물사용, 고농도의 NSAID 사용, 장기간의 치료 기간, 연소형 류마티스 관절염, 전신성 홍반성 루푸스 등이 간 독 성의 고위험군으로 여겨진다. 그러므로 NSAIDs를 처방하 거나 변경한 경우 4 내지 6주 동안 transaminase를 관찰하는 것이 안전하다.
(3) 신장; NSAIDs의 신장에 대한 영향은 신장 PG의 억제 Table 2. Classification of NSAIDs by Half-Life
ꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧ
NSAID Half-file (h) NSAID Half-file (h) ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
Aspirin 0.25 Azapropazone 15.0
Diclofenac 1.1 Carprofen 12.0
Etodolac 6.0 Diflunisal 13.0
Fenoprofe 2.5 Fenbufenn 11.0
Flufenamic aci 1.4 Meloxicamd 20.0
Flubiprofe 3.8 Nabumetonen 26.0
Ibuprofen 2.1 Naproxen 14.0
Indomethacin 4.6 Oxaprozin 58.0
Ketoprofe 1.8 Phenybutazonen 68.0
Mefenamic aci 2.0 Piroxicamd 57.0
Pirprofen 3.8 Salicylate 2.0∼15.0
Suprofen 2.5 Sulindac 14.0
Tolmetin 1.0 Tenoxicam 60.0
Tiaprofenic acid 3.0
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
Table 3. Risk Factors for NSAID Induced Mucosal Injury
ꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧ
Older age Female sex High NSAID dose Prolonged NSAID use
Combined use of NSAID and glucocorticoid Severe intercurrent illness
Unproven: H pylori infection, smoking, caffeine, alcohol ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
와 연관된다. 정상적인 신장기능을 가지고 있는 건강한 사 람에서는 PGE2 와 PGI2는 신 기능을 조절하는 데 별 영향을 미치지 않는다. 그러나 intravascualr volume이 감소하여 angiotensin II와 catecholamine이 증가된 혈역학적 긴장상태 가 되면 국소적으로 생산된 혈관확장성 PG가 적절한 신 기 능을 유지하는 데 중요한 역할을 하게 된다. NSAIDs의 복 용은 이와 같은 보상성의 PG의 생산을 억제하여 신장의 혈 액순환과 사구체 여과율을 감소시켜 수분정체와 부종, 그 리고 creatinine의 상승을 일으킨다. 또한 고칼륨혈증을 유발 할 수 있는데, 특히 당뇨병 환자나 경중등도의 신부전이 있 는 경우, 수용체 차단제나 ACE 억제제, 칼륨보존 이뇨제를 복용하고 있는 경우에 특히 주의를 요한다.
(4) 피부; 여러 종류의 피부 부작용이 발생할 수 있는데, 특히 piroxicam, sulindac, meclofenamate sodium 등에서 많이 발생하는 것으로 보고된다. 양성 홍역형 발진, 고정약진, 광 민감성 반응, 수포성 발진, 혈청병, 그리고 박탈 홍피증 (exfoliative erythroderma) 등이 발생하는 것으로 알려져 있 다. 거의 모든 NSAIDs가 다형 홍반, Stevens-Johnson 증후군, 독성표피융해증을 일으킬 수 있다.
(5) 과민반응; 기관지 천식이 있는 환자에서 아스피린과 NSAIDs는 기관지 확장성의 PG를 억제하여 천식발작을 일 으킬 수 있다. 천식에서 COX-II inhibitor의 역할에 대한 정 보는 확실하지 않으며, 이와 같은 부작용의 가능성은 상존 한다.
(6) 혈액; 재생불량성 빈혈, 과립구감소증, 혈소판감소증 등이 드물게 발생할 수 있다. 이와 같이 발생빈도가 아주 낮고 예측이 불가능한 상태에서 발생하므로 혈액검사를 주 기적으로 실시하는 것은 필요치 않다. NSAIDs에 의한 가역 적인 혈소판의 기능 장애, 예를 들어 수술 전후에 출혈 가능 성을 배제하기 위해서는 COX-II inhibitor를 사용하면 예방 할 수 있다.
(7) 중추신경계; 두통과 어지럼증이 생길 수 있으며, 그 외에도 혼란, 우울증, 졸림, 환청, 경련, 그리고 기절 등이 보고되고 있다. 특히 노인에서는 인지기능의 장애, 기억감 퇴, 집중력감소, 인격변화, 우울증, 불면, 과민, 그리고 몽롱 함 등이 발생할 수 있으므로 주의하여야 한다.
(8) 고혈압; NSAID는 고혈압을 유발할 수 있기도 하지만, 고혈압이 있는 환자에서는 혈압의 조절이 쉽지 않게 되는 경우가 많다. 혈압에 영향을 미치지 않는 약제는 prosta- glandin합성을 억제하지 않는 약제로서 salicyl salicylate가 여기에 속한다.
3) 소염진통제의 사용 원칙: 소염진통제 사용의 원칙은 1) 소염 진통제를 병합 투여하는 것은 부작용의 빈도를 증 가시키므로 의미가 없다. 2) 약물이 선택되면 2주간의 충분 한 기간 사용하여 효과가 없을 때 다른 계열의 약물로 교환
하여야 한다. 3) 약물의 효과와 부작용은 개인에 따라 다르 므로 선택은 개인에 따라 조정하여야 한다.
4) 겸용약물, 질병, 노령환자에 대한 영향
(1) 약물과 질병 간의 상호작용(Table 4); NSAIDs는 혈청 알부민과 90% 이상에서 결합하고 있기 때문에, 혈청 알부 민이 감소하거나 NSAIDs의 단백질결합을 감소시키는 조 건, 또는 간이나 신장에 의해 약물의 대사나 배설과정이 장 애를 받는 조건에서는 주어진 용량의 NSAIDs에 대한 반응 이 변화될 수 있다. 간경변증은 혈청 알부민의 감소와 간에 의한 약물의 대사에도 영향을 준다. Sulindac의 경우 간경변 증에 의해 AUC (area under the curve)가 4배 정도 증가한다.
따라서 이 경우에는 정상용량의 4분의 1만을 투여하여야 한다. 신기능이 저하된 환자에서는 diclofenac, fenoprofen, ibuprofen, indomethacin, meclofenamate, tolmetin, piroxicam, etodolac 등은 감량이 필요치 않다. 그러나 naproxen과 oxaprozin은 신기능저하 환자에서 결합되지 않은 약물의 농 도가 배가되므로 2분의 1로 감량해야 한다.
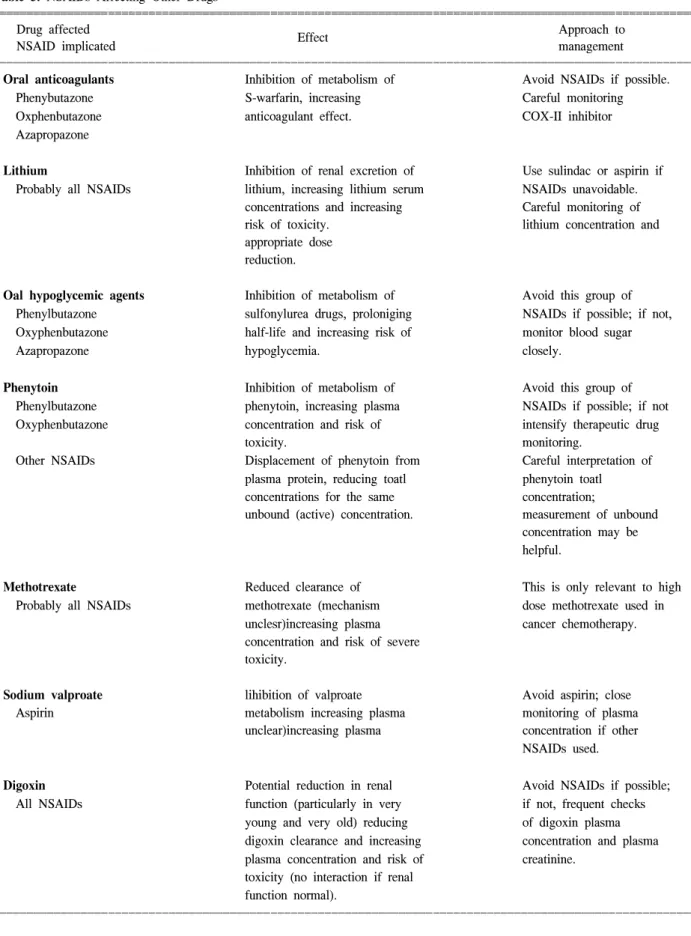
(2) 겸용약물과의 상호작용(Table 5); NSAIDs를 필요로 하는 환자들은 대개 만성적인 질환을 가지고 있는 경우가 많으므로 여러 가지 약물을 동시에 사용해야 하는 상황에 놓이게 된다. 그러므로 약물 상호간의 영향을 이해하는 것 은 중요하다.
(3) 고령환자에서의 NSAIDs 사용; 나이가 듦에 따라 여 러 가지 생리학적, 약물역동학적, 약물역학적 변화가 발생 한다. 약물의 흡수는 변화하지 않지만, 신체의 총 수분량이 감소하고 체지방이 증가하므로 약물의 분포에 변화가 온 다. 또한 간의 실질, 혈류, 효소의 활성 등이 감소하고, 신장 의 혈류감소, 사구체 여과율감소, 사구체 기능감소로 약물 의 배설이 지연된다. 노인 환자에서 naproxen, ketoprofen, 그 리고 oxaprozin은 반으로 줄여야 하지만, ibuprofen과 eto- dolac은 용량의 조절이 필요치 않다고 한다.
Table 4. The Effects of Disease States and Aging on the Elimina- tion of NSAIDs
ꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧ
Renal failure Hepaticfailure Old age ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
Azapropazone ↓ ↓ ↓
Indomethacin - ↓ ↔
Sulindac - ↓ ↓
Naproxen ↓ ↓ ↓
Ketoprofen ↓ - ↓
Tiaprofenic acid ↓ - ↓↔
Piroxicam ↔ - ↓↔
Salicylate - - ↓
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
Table 5. NSAIDs Affecting Other Drugs
ꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧ
Drug affected Approach to
Effect
NSAID implicated management
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ Oral anticoagulants Inhibition of metabolism of Avoid NSAIDs if possible.
Phenybutazone S-warfarin, increasing Careful monitoring
Oxphenbutazone anticoagulant effect. COX-II inhibitor
Azapropazone
Lithium Inhibition of renal excretion of Use sulindac or aspirin if
Probably all NSAIDs lithium, increasing lithium serum NSAIDs unavoidable.
concentrations and increasing Careful monitoring of
risk of toxicity. lithium concentration and
appropriate dose reduction.
Oal hypoglycemic agents Inhibition of metabolism of Avoid this group of Phenylbutazone sulfonylurea drugs, proloniging NSAIDs if possible; if not, Oxyphenbutazone half-life and increasing risk of monitor blood sugar
Azapropazone hypoglycemia. closely.
Phenytoin Inhibition of metabolism of Avoid this group of
Phenylbutazone phenytoin, increasing plasma NSAIDs if possible; if not Oxyphenbutazone concentration and risk of intensify therapeutic drug
toxicity. monitoring.
Other NSAIDs Displacement of phenytoin from Careful interpretation of plasma protein, reducing toatl phenytoin toatl concentrations for the same concentration;
unbound (active) concentration. measurement of unbound concentration may be helpful.
Methotrexate Reduced clearance of This is only relevant to high
Probably all NSAIDs methotrexate (mechanism dose methotrexate used in unclesr)increasing plasma cancer chemotherapy.
concentration and risk of severe toxicity.
Sodium valproate lihibition of valproate Avoid aspirin; close
Aspirin metabolism increasing plasma monitoring of plasma
unclear)increasing plasma concentration if other NSAIDs used.
Digoxin Potential reduction in renal Avoid NSAIDs if possible;
All NSAIDs function (particularly in very if not, frequent checks young and very old) reducing of digoxin plasma digoxin clearance and increasing concentration and plasma plasma concentration and risk of creatinine.
toxicity (no interaction if renal function normal).
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
(4) NSAIDs에 대한 반응의 개인차; NSAIDs에 대한 반응 은 개인에 따라 아주 커다란 차이를 보인다. 예를 들어 혈장 반감기의 경우 4∼5배의 차이를 보이고, 효능을 보는 연구 에서는 현저한 향상을 보이는 경우부터 전혀 반응이 없는 경우, 심지어 임상적으로 악화되는 경우까지 다양한 결과 를 보인다. 그러나 인간의 다양한 유전적, 식이적, 환경적 다양성으로 인해 이와 같은 다양한 반응은 전혀 예측할 수 없다.
참 고 문 헌
1. Whitcomb DA, Block GD. Association of acetaminophen with fasting and ethanol use. JAMA 1994;272:1845-50.
2. Lee SH, Kim SI, Yoo WH, Suh CH, Lee SK, Kim JS, et al.
The comparison of the efficacy and gastrointestinal side effects of tylenol-ER (Extended Relief) and naproxen in the treatment
of osteoarthritis of knee: Multicenter trial. J Korean Rheum Assoc 1998;5:211-20.
3. Paulus HE. FDA arthritis advisory committee meeting: Post- marketing surveillance of nonsteroidal anti-inflammatory drugs.
Arthritis Rheum 1985;28:1168-9.
4. Vane JR. Inhibition of prostaglandin synthesis as a mechanism of action for aspirin-like drugs. Nature 1971;231:2.
5. Santana-Sabaga E, Weisman MH. Nonsteroidal antiinflamma- tory drugs. In: Ruddy S, Harris ED, Sledge CB, editors.
Kelly's textbook of rheumatology. 6th ed. Philadelphia: Saun- ders Co; 2001. p. 799-822.
6. Crofford IJ. COX-1 and COX-2 tissue expression: Implications and predictions. J Rheumatol 1997;24(suppl 49):S15-9.
7. Maciel FM, Sarrazin P, Morisset S, Lora M, Patry C, Dumais R, Brum-Fernandes AJ. Induction of cyclooxygenase-2 by parathyroid hormone in human osteoblasts in culture. J Rheu- matol 1997;24:2429-35.
Table 5. Continued
ꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧ
Drug affected Approach to
Effect
NSAID implicated management
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
Aminoglycosides Reduction in renal function in Close plasma
All NSAIDs susceptible individuals, reducing concentration monitoring aminoglycoside clearnace and and dose adjustment.
increasing plasma concentration.
Antihypertensive Reduction in hypotensive effect, Avoid all NSAIDs in treated agents β-blockers, probably related to inhibition of hypertensive patients if
diuretics, renal prostaglandin synthesis possible; if not monitor
ACE inhibitors (producing salt and water carefully.
vasodilators retention)and vascular May need additional
Indomethacin prostaglandin synthesis antihypertensive therapy.
Other NSAIDs vasoconstriction).
Diuretics Reduction in natriuretic and Avoid NSAIDs in patients
Incomethacin diuretic effects; may exacerbate with cardiac failure;
Other NSAIDs congestive cardiac failure. monitor clinical signs of fluid retention.
Anticoagulants Gastrointestinal tract mucosal Avoid all NSAIDs if
All NSAIDs damage, together with inhibition possible.
of platelet aggregation,
increasing risk of GI bleeding in patients on anticoagulants,
Hypoglycemic agents Potentiation of hypoglycemic Monitor blood sugar level.
Salicylate(high dose) effects(mechanism unknown.)
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
8. Breder CD, Dewitt DL, Kraig RP. Characterization of inducible cyclooxygenase in rat brain. J Comp Neurol 1995;355:296- 315.
9. O'Neill GP, Ford-Hutchinson AW. Expression of mRNA for cyclooxygenase-1 and cyclooxygenase-2 in human tissues.
FEBS Lett 1993;330:156-60.
10 Appel GB. COX-2 inhibitors and kidney. Clin Exp Rheumatol 2001;19(suppl 25):S37-40.
11. FitzGerald GA, Cheng Y, Austin S. COX-2 inhibitors and the cardiovascular systems. Clin Exp Rheumatol 2001;19(suppl 25):S31-6.
12. Garcia Rodriguez LA. The effect of NSAID on the risk of coronary heart disease: fusion of clinical pharmacology and pharmacoepidemiologic data. Clin Exp Rheumatol 2001;19 (suppl 25):S41-4.
13. Fries JF. The epidemiology of NSAID gastropathy. The ARAMIS experience. J Clin Rheumatol 1998;4(Supp1):S11.
14. Friedman LS, Peterson WL. Peptic ulcer and related diseases.
In: Fauci AS, Braunwald E, Isselbacher KJ, et al, editors.
Harrison's principle of internal medicine 14th. ed. New York McGraw Hill; 2001. p. 1610.
15. Silverstein FE, Graham DY, Senior JR, Davies HW, Struthers B, Bittman RM, Geis GS. Misoprostol reduces serious gas- trointestinal complications in patients with rheumatoid arthritis receiving nonsterodal anti-inflammatory drugs. Ann Intern Med 1995;123:241-9.
16. Patrono C. Measurement of cyclooxygenaseisozyme inhibition in humans: exploring the clinical relevance of biochemical selectivity. Clin Exp Rheumatol 2001;19(suppl 25):S45-50.