Introduction
High tibial osteotomy (HTO) is an established surgical treat
ment option for younger patients with medial compartment knee
osteoarthritis (OA) with varus deformity that shifts the load on the knee joint by changing lower limb alignment
1). Optimal limb alignment is a paramount factor for satisfactory surgical results of HTO
2)because poorly corrected alignment has been reported as one of the important causes of unsatisfactory clinical outcome after HTO
35).
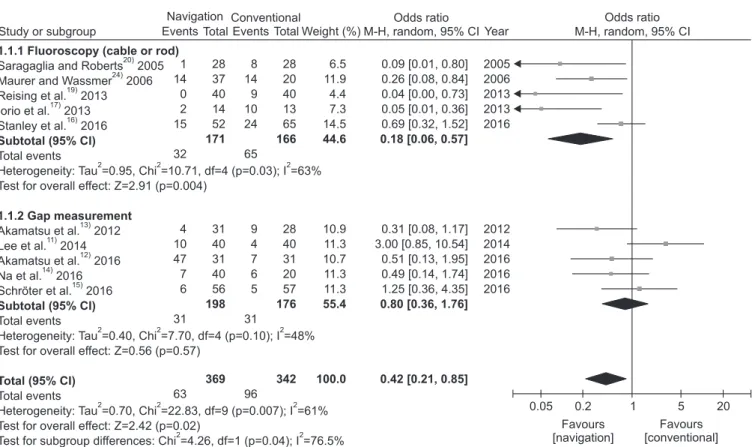
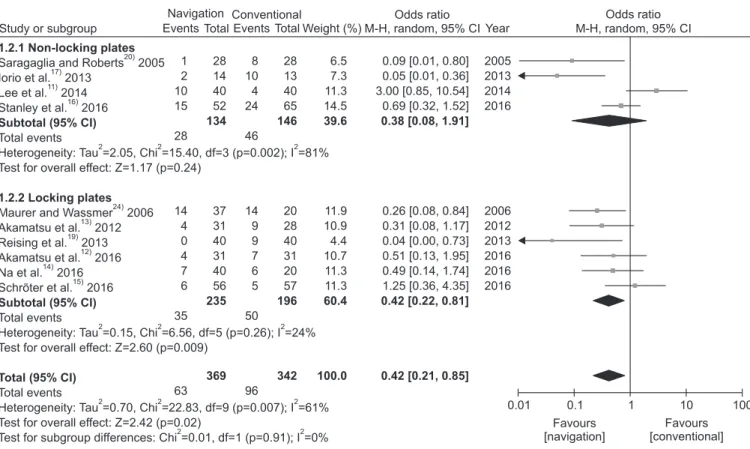
Navigation was introduced in HTO to improve the accuracy of alignment correction
6,7), but it is still unclear whether navigated HTO is superior to the conventional technique regarding the achievement of the target coronal alignment. Recent systematic reviews or metaanalyses reported that the use of navigation in HTO could improve the precision of coronal alignment correc
tion
810). However, there is conflicting evidence showing less outli
er in the conventional HTO using the weight bearing scanogram technique
11)or comparable accuracy in coronal alignment
1216). Conventional HTO can be divided into different categories based on the detailed surgical technique, particularly by the method for
Navigated versus Conventional Technique in
High Tibial Osteotomy: A MetaAnalysis Focusing on Weight Bearing Effect
Kyung Wook Nha, MD, PhD 1, *, YoungSoo Shin, MD, PhD 2, *, Hyuk Min Kwon, MD 3 , Jae Ang Sim, MD, PhD 3 , and Young Gon Na, MD 3
1