Development of a New Cardiac and Torso Phantom for Verifying the Accuracy of Myocardial Perfusion SPECT
― 심근관류 SPECT 검사의 정확도 검증을 위한 새로운 심장 ․ 흉부 팬텀의 개발 ―
Tomoaki Yamamoto
1)․ Jung Min Kim
2)․ Ki Sung Lee
2)Teruhiko Takayama
3)․ Tadashi Kitahara
4)1)
Dept. of Radiological Sciences, School of Health Sciences, International University of Health and Welfare, Japan
2)
Dept. of Radiologic Science, College of health sciences, Korea University, Korea
3)
Dept. of Clinical Laboratory Science, Graduate School of Medicine, Kanazawa University, Japan
4)
Department of Radiology, Fujigaoka Hospital, Showa University, Japan
― Abstract ―
Corrections of attenuation, scatter and resolution are important in order to improve the accuracy of single photon emission computed tomography (SPECT) image reconstruction. Especially, the heart movement by respiration and beating cause the errors in the corrections. Myocardial phantom is used to verify the correction methods, but there are many different parts in the current phantoms in actual human body.
Therefore the results using a phantom are often considered apart from the clinical data. We developed a new phantom that implements the human body structure around the thorax more faithfully. The new phantom has the small mediastinum which can simulate the structure in which the lung adjoins anterior, lateral and apex of myocardium. The container was made of acrylic and water-equivalent material was used for mediastinum. In addition, solidified polyurethane foam in epoxy resin was used for lung. Five different sizes of myocardium were developed for the quantitative gated SPECT (QGS). The septa of all different cardiac phantoms were designed so that they can be located at the same position. The proposed phantom was attached with liver and gallbladder, the adjustment was respectively possible for the height of them. The volumes of five cardiac ventricles were 150.0, 137.3, 83.1, 42.7 and 38.6 ml respectively. The SPECT were performed for the new phantom, and the differences between the images were examined after the correction methods were applied. The three-dimensional tomography of myocardium was well reconstructed, and the subjective evaluations were done to show the difference among the various corrections. We developed the new cardiac and torso phantom, and the difference of various corrections was shown on SPECT images and QGS results.
Key Words : cardiac phantom, torso phantom, myocardium, SPECT
*접수일(2008년 9월 18일), 심사일(2008년 11월 21일), 채택일(2008년 12월 5일) 교신저자: Jung Min Kim, (136-703) Dept. of Radiologic Science,
College of health sciences, Korea University, Korea TEL : 82-2-940-2824, C.P. : 82-10-6744-1956 E-mail : [email protected]
Ⅰ. Introduction
The photons, which reach the detector from the radiation source in the human body, affect the reconstruction by various interactions, when the SPECT images are reconstructed. It is necessary to develop the techniques in which the correction accuracy is improved in the image reconstruction by the verification of the effect by these interactions.
Although there are three type corrections of attenuation, scatter and resolution for SPECT, they have been rarely applied to the myocardial SPECT.
In attenuation correction, Chang’s method is widely utilized, but it is unsuitable for the non-uniform absorber
1). While the triple energy windows method (TEW) had been a standard method for scatter correction
2), recently, resolution correction by frequency and distance relationship (FDR) and collimator blurring correction (CBC) were proposed for SPECT
3-4). There are two reasons for not using these corrections for myocardial SPECT. One is non-uniformity, and the other is motion caused by respiration and beating of myocardium. The image without attenuation correction causes the decrease of activity in the inferior, and the image without scatter correction causes the decrease of the contrast. In addition, the image without resolution correction leads to the defect in 10 or 11 o'clock direction of myocardium. The conventional cardiac and torso phantoms have differences in terms of structure and size for human body, which cause discrepancy in results between phantom experiments and clinical scans.
The recent computer technology remarkably advances in the field of medical image. Transmission computed tomography (TCT) provides anatomical information for conventional emission images, which improves the accuracy in the diagnostic imaging.
Corrections are indispensable for the image accuracy of cerebral blood flow SPECT or the detection sensitivity improvement of tumor scintigraphy. The high-performance computer provides much infor
mation for some corrections, and contributes to the
diagnostic improvement. Therefore, it is possible to apply the more accurate corrections in the myocardial SPECT image.
There is always the movement by respiration and heartbeat on the myocardium unlike other organs.
The distribution of the linear attenuation coefficient of myocardium and other organs around cardiac portion is much different, these organs are adhered structure, for example, myocardium, lung, mediastinum and liver.
The quantitative gated SPECT (QGS) is widely utilized for the clinic for the functional analysis of the myocardial SPECT
5). As for the pumping the radioactive solution in the balloon, currently available myocardial dynamic phase phantom in the market is based on the contraction of the pump.
This method, however, allows the movement of the cardiac ventricle only, and about 20% of the ejection fraction (EF). In addition, the anatomical structure was not sufficiently considered in the existing method
6-7).
The purpose of this study is to develop a new type of cardiac and torso phantom that simulates the structure of the human body as accurately as possible, and evaluate its performance with the reconstructed images and the results of QGS.
Ⅱ. Materials and Methods
1. Development of the new cardiac and torso phantom
Materials of the container and partition were the
acrylic. Water-equivalent material was used for
mediastinum, and solidified polyurethane foam in
epoxy resin was used for lung. Different sizes of
five cardiac phantoms were made for QGS. Those
five sizes of cardiac phantoms will be called A, B,
C, D and E in descending order. The water-
equivalent material was made from SZ-204 (Kyoto
Kagaku Corp., Kyoto, Japan). The liver was made
in two-layer structures in order to change the
height, and gallbladder was made to be the structure in which the height is varied by rotating the screw.
The gallbladder phantom was spherical and its diameter was 20 mm. The inside of two-layer structure of liver is a cavity, and two screw caps for flowing liquid solution into each layer were installed to one by one in the base of phantom. For example, radioactive solution is filled in the lower layer and water is filled in upper layer, the diaphragm is at low position, also radioactive solution is filled in the both layer, the position of diaphragm is at high position. Then high-radioactive solution was filled in it so that the streak artifact could be reproduced. The different sizes of cardiac phantoms were unitized with the parts around it so that it can be easily disassembled. The drawing of the torso phantom and five cardiac phantoms are shown in Figs. 1 and 2. The bases of five cardiac phantoms were produced so that they are located at the same position at all times. It is not possible to input the radioactive solution in cardiac ventricle, because it was made from the acrylic core. The portion of myocardium is a cavity, and the screw caps were installed in the base of myocardium for an inlet, radioactive solution can be filled into the portion of myocardium through the inlet. Mediastinum and lung were solid with each material. The volume of each portion of cardiac phantom was shown in Table 1.
Fig. 1. Illustration of the outline of the new cardiac and torso phantom.
Fig. 2. Illustration of the outline of the five cardiac phantoms. The each phantom was marked A, B, C, D and E respectively from left.
Table 1. The volume data was shown in the design of the myocardial portion.
A B C D E mean SD
Volume of
ventricle portion 150.0 137.3 83.1 47.2 38.6 91.2 50.9 Volume of
myocardial potion 238.8 238.6 238.0 237.4 232.8 237.1 2.5 Thickness of
myocardial potion 13.0 13.0 16.0 19.5 20.0 16.3 3.38
The thickness of each myocardial portion was different, because myocardial volumes of five cardiac phantoms were all same. The other myocardial phantoms do not contain such structure, thus we believe that the proposed design is more similar to the human body. The general view and the aspect of desorption of the new phantom were shown in Fig. 3. The time required of the desorption is about 1 minute, and then the main body is fixed, the base portion of each cardiac phantom was always on equal position.
2. Examinations for the phantom
We used PRISM 3000XP (Shimadzu Medical Systems
Co. Ltd., Kyoto, Japan) SPECT system which has
three detector units. Low energy high-resolution
cardiac exclusive fan-beam collimator (Cardio-Fan
Collimator) was attached to the detector heads. The collection protocol was shown at Table 2. Emission and transmission source for attenuation correction were Tl-201 and Tc-99m (700 MBq) respectively.
The collection method was simultaneous transmission emission protocol (STEP). The concentrations (78.5
±0.8 kBq/ml) of Tl-201 were 78.0, 78.0, 78.2, 78.5 and 80.0 kBq/ml respectively for five cardiac phantoms, A, B, C, D and E. The concentration of 26.0 kBq/ml was filled in hepatic portion, and ratio of concen
tration of heart and liver was 3 : 1. The ratio of concentration of heart and liver was estimated from the average of clinical data. A type of cardiac phantom corresponds to the end of diastole (ED), and E type was correspondent to the end of systole (ES). The other type, B, C and D were made in order to become middle volume of myocardial of A and B. After the cardiac phantoms of A to B were fixed to the torso phantom, five sets of SPECT projection data were obtained. The selection of ED and ES are controllable with the adequate myocardial phantoms.
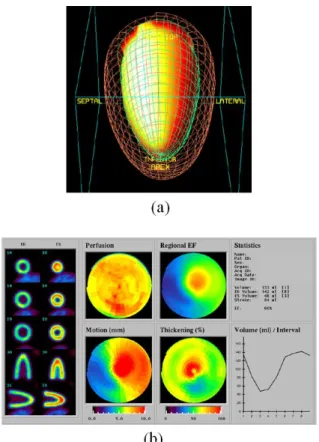
Fig. 3. The general view of the new cardiac and torso phantom was shown. The whole images were shown in (a), attached the cardiac phantom unit was performed in (b), and a phantom was set on the bed of SPECT system in (c).
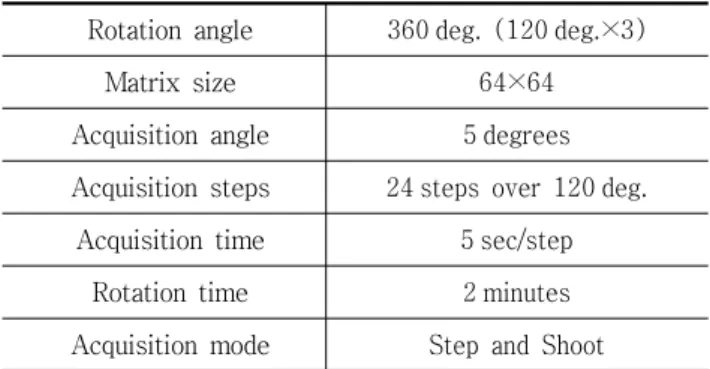
Table 2. Acquisition protocols.
Rotation angle 360 deg. (120 deg.×3)
Matrix size 64×64
Acquisition angle 5 degrees Acquisition steps 24 steps over 120 deg.
Acquisition time 5 sec/step Rotation time 2 minutes Acquisition mode Step and Shoot
3. Reconstruction and correction
Ordered subset expectation maximization (OSEM) was conducted for STEP with six iterations and eight subsets
8-9). The STEP was a method that performs simultaneously attenuation correction and scatter correction in the image reconstruction. The attenuation and scatter correction was based on transmission dependent convolution subtraction (TDCS)
10)main energy window (73 keV±15%), two energy windows (58 keV±2.5%, 87 keV±2.5%) for scatter correction and the energy window (140 keV
±7.5%) for attenuation correction were set in the protocol. FDR, which corrects the projection data, was used for resolution correction. The algorithm of FDR was written in C language, and it was processed on the workstation of PRISM. The resolution correction was conducted to projection data. The corrected projection data, scatter and transmission data were used for reconstruction by STEP using a Butterworth filter with an order of 8 and a critical frequency of 0.36 cycles/cm. The image reconstructions were divided into two cases, one with attenuation and scatter, and the other with only resolution corrections.
4. Convert to dynamic data from planar data for QGS
Gated myocardial SPECT data of 8 to 32 phases
were necessary for analysis of QGS. The new
phantom was not dynamic phase phantom. Therefore,
data sets from the five cardiac phantoms were individually collected and eight phases were made by the use of five data sets, and eight planar data were converted to eight dynamic phase data. Fig. 4 shows an example of the converted model. In this particular example the list of the phantoms is A-C-E-D-C-B-B-A. The conversion of the data could be simplified on the workstation.
0 40 80 120 160
1 2 3 4 5 6 7 8
Cardiac phase
Volume of cardiac ventricle(ml)
Fig. 4. The example of dynamic phase with the eight phases using five cardiac phantoms in order to A-C-E- D-C-B-B-A was shown in a figure.
5. Displays and Analysis
Attenuation correction, scatter correction, resolution correction and non-correction were marked AC, SC, RC and NC respectively. The short axis images were shown in all reconstructions. The effect on each image by the some corrections was evaluated with subjective measurement. The profile of each image for x-axis and full width at half maximum (FWHM) were produced to evaluate the contrast by the corrections. QGS was performed from dynamic phase short axis image of the eight divisions, and each ejection fraction (EF) with some corrections was compared with the true value.
Ⅲ. Results
The short axial images of ED and ES with AC and SC, also with and without RC are shown in Fig. 5. The images on the left side mean end of diastole, and those on the right side mean end of systole. Upper part of the figure shows the images with RC, and lower part shows the images without RC. The images of ES have uniformly been recon
stituted in spite of the existence of RC, though there was the decrease of concentration in septum and lateral of ED. The difference in size was found in apex of ES according to the effect of RC. The short axial images of ED and ES with AC, also with and without RC are shown in Fig. 6. The configu
ration of the images is equal to Fig. 5. There is no visual difference by the effect of RC, though the uniformity in the portion of myocardium was improved than the images with ACSC. The short axial images of ED and ES with SC, also with and
Fig. 5. Reconstructed images with ACSC on the existence of RC were shown. Upper side and lower side images were shown images with RC and without RC respectively.
Left side and right side images were shown in end of
diastole and systole respectively.
Fig. 6. Reconstructed images with AC on the existence of RC were shown in similar.
Fig. 7. Reconstructed images with SC on the existence of RC were shown in similar.
Fig. 8. Reconstructed images with NC on the existence of RC were shown in similar.
without RC are shown in Fig. 7. The configuration of the images was equal to the other short axial images. The decreasing of the inferior is observed in all images, when AC was not conducted. There was no visual difference by the effect of RC. The short axial images of ED and ES with and without RC are displayed in Fig. 8. Generally by utilizing these images in the clinic, the decreasing of the inferior is observed, too.
The profile curves of x-axis of short axial images
with and without RC are shown in Figs. 9, 10. In
comparison with and without AC, there was the
increase on the concentration of the myocardial
portion with AC. The concentration of septum was
increased than lateral. Though the radioactivity was
not in the cardiac ventricle in the phantom, the
concentrations were shown in all reconstructed
images. When RC was applied, the concentration in
the cardiac ventricle decreased, and the contrast
was improved in the images. The FWHM of Figs. 9
and 10 were shown in Table 3. In the case of
ACSC, AC, SC and NC with RC, the mean values of
FWHM were 19.8, 25.9, 20.2 and 31.7 mm respec
tively. And in the case of ACSC, AC, SC and NC without RC, the mean values of FWHM were 23.4, 25.2, 23.8 and 35.6 mm respectively. Expect for the correction only of AC, FWHM was decrease by RC.
In the case of AC, the value of FWHM without RC was less than without RC.
0 20 40 60 80 100
20 25 30 35 40 45
pixel number
Septal --> cardiac ventricle --> Lateral
%MAX
ACSC AC SC NC
Fig. 9. Profile curves of non-gated x-axial for short axial image with RC.
0 20 40 60 80 100
20 25 30 35 40 45
pixel number
Septal --> cardiac ventricle --> Lateral
%MAX ACSC
AC SC NC