원고 접수일 2010년 9월 20일, 게재 확정일 2011년 1월 4일 책임저자 이종호
(110-749) 서울시 종로구 연건동 28번지, 서울대학교 치의학대학원 구강악안면외과 학교실
Tel: 02-2072-2630, Fax: 02-766-4948, E-mail: [email protected]
RECEIVED September 20, 2010, ACCEPTED January 4, 2011 Correspondence to Jong-Ho Lee
Department of Oral and Maxillofacial Surgery, School of Dentistry, Seoul National University
28, Yeongun-dong, Chongro-gu, Seoul 110-749, Korea
Tel: 82-2-2072-2630, Fax: 82-2-766-4948, E-mail: [email protected]
CC This is an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/
by-nc/3.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Dehydrothermal Treatment로 제작한 흡수성 콜라겐 골유도재생술 차단막
방강미1ㆍ정한울1ㆍ김성포2ㆍ양은경2ㆍ김기호2ㆍ김성민1ㆍ김명진1ㆍ장정원3ㆍ이종호1,3
1서울대학교 치의학대학원 구강악안면외과학교실, 2바이오랜드연구소, 3서울대학교 치의학연구소
Abstract
Absorbable Guided Bone Regeneration Membrane Fabricated from Dehydrothermal Treated Porcine Collagen
Kang-Mi Pang 1 , Han-Wool Choung 1 , Sung-Po Kim 2 , Eun-Kyung Yang 2 , Ki-Ho Kim 2 , Soung-Min Kim 1 , Myung-Jin Kim 1 , Jeong Won Jahng 3 , Jong-Ho Lee 1,3
1
Department of Oral and Maxillofacial Surgery, School of Dentistry, Seoul National University,
2Bioland,
3
Dental Research Institute, Seoul National University
Purpose: Collagen membranes are used extensively as bioabsorbable barriers in guided bone regeneration. However, collagen has different effects on tissue restoration depending on the type, structure, degree of cross-linking and chemical treatment.
The purpose of this study was to evaluate the inflammatory reaction, bone formation, and degradation of dehydrothermal treated porcine type I atelocollagen (CollaGuideⓇ) compared to of the non-crosslinked porcine typeI, III collagen (BioGideⓇ) and the glutaldehyde cross-linked bovine type I collagen (BioMendⓇ) in surgically created bone defects in rat mandible.
Methods: Bone defect model was based upon 3 mm sized full-thickness transcortical bone defects in the mandibular ramus of Sprague-Dawley rats. The defects were covered bucolingually with CollaGuideⓇ, BioMendⓇ, or BioGideⓇ (n=12). For control, the defects were not covered by any membrane. Lymphocyte, multinucleated giant cell infiltration, bone formation over the defect area and membrane absorption were evaluated at 4 weeks postimplantation. For comparison of the membrane effect over the bone augmentation, rats received a bone graft plus different covering of membrane. A 3×4 mm sized block graft was harvested from the mandibular angle and was laid and stabilized with a microscrew on the naturally existing curvature of mandibular inferior border. After 10 weeks postimplantation, same histologic analysis were done.
Results: In the defect model at 4 weeks post-implantation, the amount of new bone formed in defects was similar for all types of membrane. Bio-GideⓇ membranes induced significantly greater inflammatory response and membrane resorption than other two membranes; characterized by lymphocytes and multinucleated giant cells. At 10 weeks postoperatively, all membranes were completely resorbed.
Conclusion: Dehydrotheramal treated cross-linked collagen was safe and effective in guiding bone regeneration in alveolar ridge defects and bone augmentation in rats, similar to BioGideⓇ and BioMendⓇ, thus, could be clinically useful.
치과 임플란트가 계속 발전하면서 치조골증강술은 필수불가결 한 술식이 되었다. 골유도재생술(guided bone regeneration, GBR)은 Dahlin[1]이 외과적 골결손부를 형성하고 차폐막의 사용 여부에 따라 치유양상의 차이점을 보고하여 등장하였으며, 현재 치조골증강술을 위한 하나의 방법으로 확립되어 있다. 골유도재 생술에 이용되는 차폐막은 치조골결손부위에 치조골세포가 도달 해서 골조직의 재생을 유도할 때까지 인접 상피세포, 결체조직 세포가 도달하지 않도록 막는 역할을 한다[2]. 골유도재생술 및 조직유도재생술에 사용하기 위해 차폐막은 생체적합성, 조직 부 착능, 공간유지력, 세포폐쇄능, 조작용이성을 갖추어야 한다[3].
치주조직 재생을 위한 조직유도재생술에서는 4∼6주 정도의 짧은 기간동안만 차단기능을 유지하면 되지만, 골유도재생술에는 보다 긴 기간이 필요하다[2]. 처음에 사용되었던 비흡수성 차단막은 긴 시간에 걸쳐 조직을 분리시키는 능력을 유지하고, 막이 노출되 지 않으면 차단막은 수개월에서 수년간 남아있어 골재생에 영향을 준다. 그러나, 차단막 제거를 위한 부가적인 수술이 필요하며, 일단 노출되면 자발적인 치유가 일어나지 않고, 구강 내 세균에 의해 오염되어, 시술부위를 감염시키고 결국은 골흡수를 일으킨 다. 따라서 노출된 막을 제거해야 하는데, 차단막의 조기 제거는 충분한 골생성을 어렵게 한다. 이에, 최근에는 흡수성 차단막의 사용에 대한 관심이 증가되고 잇다. Wallace 등은 상악동 거상술 식에서 골 창을 피개함에 있어서 비흡수성 차단막과 흡수성 차단 막 사이의 생활골 형성과 임플란트 생존에 유의할 만한 차이는 없다고 보고하였다[4]. 흡수성 차단막은 collagen, dura mater, polylactic/polyglycolic acid, calcium sulfate, chitosan 등을 재료로 하여 개발되었으며, 현재 치과 임상에서의 사용빈도가 증가하고 있다[5]. 그 중 collagen은 중성구와 섬유모세포를 활성 화시키고 혈병형성에 관여하며, 항원성이 적어 많이 사용되어 왔으며, 양호한 임상적 결과를 보였다[6]. 그러나 자연 collagen의 주요한 단점은 거대세포와 다핵세포에 의해 빠르게 분해되어 차단 막이 조기에 결손부위로 붕괴할 수 있어 가공과정을 필요로 한다.
최근에는 collagen fiber의 교차결합 정도를 변화시킴으로써 기 계적 특성을 변화시키고 있다. 교차결합은 collagen 분자 사이에 있는 아미노산의 side chain의 결합으로, stress에 대해 collagen fiber가 서로 sliding되는 것을 방지하여 stiffness를 증가시켜주 고, 분해를 지연시켜주어, 교차결합을 이용하지 않은 차단막에 비해 우수한 결과를 보였다[7].
본 연구는 돼지 진피 collagen을 이용, dehydrothermal treat-
지 않은 콜라겐인 BioGide
Ⓡ(Geistlich Biomaterials, Wolhu- sen, Switzerland)와 송아지 콜라겐을 glutaraldehyde로 교차결 합시킨 BioMend
Ⓡ(Sulzer Medica, Colla-Tec Inc., Plainsboro, NJ, USA)과 비교하였다.
연구방법
1. 차단막
실험에 사용된 collagen 멤브레인(CollaGuide
Ⓡ, ㈜바이오랜 드, Cheonan, Korea)은 돼지의 진피에서 추출 및 정제된 타입I atelocollagen이 주성분으로 이루어져 있으며, 필름층과 다공성 스폰지층의 이중 구조로 이루어져 있다(Fig. 1). 차단막의 필름층 은 상처 주변부위의 연조직이 상처부위로 유입되지 못하도록 하는 차폐막의 역할을 하며, 다공성 스폰지층은 뼈조직의 재생을 돕는 역할을 하도록 설계되었다. 진공상태에서 collagen을 고온에서 (>90
oC) 수분을 제거함으로써 에스터화(esterification)나 아마 이드 형성(amide formation)을 통한 응축을 야기시켜 분자간 교차결합을 형성하는 dehydrothermal treatment (DHT) 기법 을 이용하였다[8]. 비교 차단막으로는 돼지 dermis 유래의 non-cross-linked type I & III collagen인 BioGide
Ⓡ와 gluta- raldehyde cross-linked bovine type I collagen인 BioMend
Ⓡ를 사용하였다.
2. Bone defect model
실험동물은 24마리의 6주령 Sprague-Dawley 백서를 이용하
였으며 실험 및 사육은 서울대학교 치의학대학원 실험동물위원회
의 지침 및 동물실험 관련 법규를 준수하였다. Sodium pento-
barbital 복강 내 주사(50 mg/kg)를 통한 전신마취 후, 부가적으
로 출혈감소와 국소 마취를 위해 1:100,000 epinephrine을
함유한 2% lidocaine HCl을 수술 부위에 피하주사하였다. 백서
의 하악골 부위를 제모하고 베타딘으로 소독한 후 무균적 조건하
에서 하악골 하연부위를 #15 수술도를 이용하여 절개하고 협
설측 모두 전층 판막을 거상하여, 하악골 하악지 협측 면의 하악각
을 노출시켰다. 직경 3 mm의 trephine bur를 이용해, 3 mm
bilateral transcortical defect를 양측 하악지에 형성 후, 차단막
을 9 mm로 다듬어 주변골에 3 mm씩 겹치도록 하며 골 결손부의
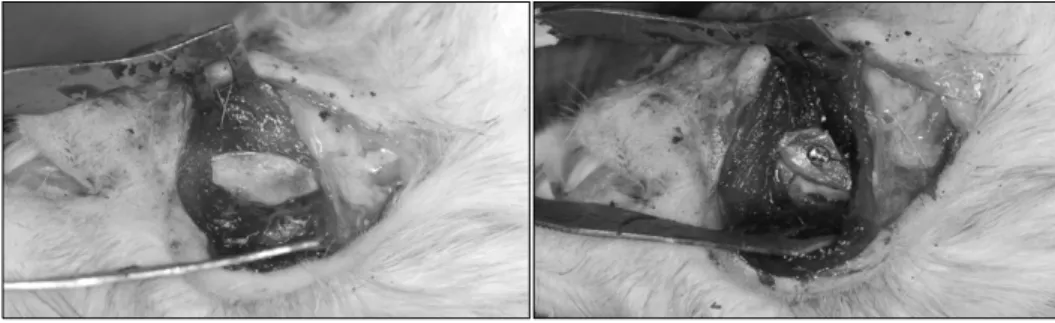
협 설측을 덮어주었다(Fig. 2). 12마리는 우측에 Bio-Mend
Ⓡ,
Fig. 1. (A) Scanning electron micro-
scope figure of test membrane (CollaGuideTM) (crosssectional view), (B) Photograph of test membrane.Fig. 2. Bone exposure, defect crea-
tion, membrane placement of lin- gual side, membrane placement of buccal side in bone defect model.좌측에 실험막(CollaGuide
Ⓡ)을 이식하였으며, 나머지 12마리는 우측에 Bio-Gide
Ⓡ를 좌측에는 차단막을 덮지 않았다. 실험막은 이식하기 전 40초간 물에 담근 후 적용하였다. 차단막 이식 후 판막을 원래 위치에 고정시킨 후, 층별 봉합하였다. 4주 후에 동물을 희생하여 하악골을 적출한 후 수술부위의 조직절편을 채취 하였다. 채취한 조직절편은 10% neutral formalin으로 고정하고, 5% 질산용액에 탈회를 거쳐 파라핀에 포매한 다음, 최종적으로 하악골에 수직(vertical section) 방향으로 4∼6 um 두께로 잘라 서, hematoxilin and eosin (H&E) stain과 Masson's trichrome (MT) stain을 하였다. 슬라이드 이미지는 RT
TM-KE color mosaic (Diagnostic Instruments, Inc, Michigan, USA)를 이용하여 촬영하였고 SPOT software ver. 4.6 (Diagnostic Instruments, Inc, Michigan, USA)를 이용하여 디지털화하였다. 염증반응을 평가하기 위해 H&E stain 절편에서 반정량화방법(semiquanti- tive method)으로 림프구(lymphocyte)와 다핵거대세포 (multinucleated giant cell)의 수를 점수화하였다(0=no cells, 1=few cells, 2=mild inflatrate, 3=moderate infiltrate, 4=se- vere infiltrate).
MT stain 절편에서는 결손부위에서 신생골로 채워진 면적을
이미지분석소프트웨어(Optimas ver. 6.5, Image Processing Solutions, Inc., North Reading, Massachusetts, USA)를 이용 하여 계산하였다. Lamella bone과 non-lamella bone과의 구분 은 통상적인 조직학적 기준을 이용하였으며, 신생골 형성은 신생 골 면적을 막으로 둘러싸여 있는 곳에서 신생골이 차지하고 있는 부분과 그 주변의 골결손 부위의 넓이의 합으로 나눈 후 백분율로 표시하였다. 차단막의 흡수 정도는 반정량화방법을 이용해 점수 화 하였다(0: 차단막 흡수 없음, 1: 표층에만 혈관형성, 2: 차단막 의 1/2 두께까지 혈관형성, 3: 차단막 전체 두께에 혈관형성, 4: 차단막의 완전한 분해).
3. Bone augmentation model
24마리의 6주령 Sprague-Dawley rats을 이용하여 man- dibular angle에서 골을 채취하여, 3×4 mm size로 다듬었다.
채취한 골을 하악골 하연의 곡면에 위치시키고 microscrew를
이용해 고정한 후, 차단막으로 피개하였다(Fig. 3). 12마리는 우
측에 Bio-Mend
Ⓡ, 좌측에 실험막을 이식하였으며, 나머지 12마
리는 우측에 Bio-Gide
Ⓡ를 좌측에는 차단막을 덮지 않았다. 백서
는 10주 후에 희생하여 동일한 방법으로 절편 형성 후, 염증정도,
Fig. 3. Bone exposure, harvested
bone fixation with microscrew at bone augmentation model.Table 1. Score of lymphocyte, multinucleated giant cell infiltration, membrane absorption of bone defect model at 4 weeks post-oper-
ativelyScore of Lymphocyte Giant cell Resorption of membrane
0 1 2 3 4 0 1 2 3 4 0 1 2 3 4
Number of specimen BG 0 1 1 2 1 0 0 3 2 0 0 0 3 2 0
BM 0 2 2 1 0 0 0 3 2 0 0 4 1 0 0
Test 0 3 2 0 0 0 4 1 0 0 1 3 0 0 0
BG, BioGide; BM, BioMend; Test, CollaGuide.
Score of lymphocyte, multinucleated giant cell infiltration: 0=no cells, 1=few cells, 2=mild inflatrate, 3=moderate infiltrate, 4=severe infiltrate. Score of membrane absorption: 0=no membrane resorption, 1=superficial vascularization, 2=half of the membrane body vascularized, 3=nearly complete vascularization of the membrane body, 4=complete degradation of membrane.
차단막 흡수 정도, 골흡수 여부를 확인하였다.
4. 통계분석
차단막의 종류와 림프구 점수, 다핵거대세포 점수, 차단막 흡수 점수와의 관계는 Fisher's exact test를 이용하여 분석하였고, 차단막의 종류와 신생골형성의 관계는 Kruskal-Wallis분석을 시 행하였다. P 값이 0.05보다 작을 때 통계적으로 유의한 것으로 판정하였다.
결 과
1. Bone defect model
4주 후, 10마리의 백서가 생존하였다(Biomend
Ⓡ/실험막 5마 리, BioGide
Ⓡ/no membrane 5마리). 염증세포 침윤정도를 반 정량화 한 분석에서 실험막은 BioGide
Ⓡ와 BioMend
Ⓡ에 비해 적은 다핵거대세포 침윤을 보여주어( P =0.048), 이물반응이 낮았 다. 림프구의 침윤정도, 신생골 형성(Mean±SD: BioGide
Ⓡ0.48±0.15, BioMend
Ⓡ0.42±0.17, Test 0.53±0.14)은 유의 한 차이를 보이지는 않았다(각각 P =0.729, P =0.465). 차단막 흡수는 BioGide
Ⓡ가 실험막과 Biomend
Ⓡ에 비해 유의하게 많았 다( P =0.016) (Table 1, Fig. 4∼6).
2. Bone augmentation model
10주 후, 7마리의 BioMend
Ⓡ/실험막 군과 2마리의 BioGide
Ⓡ/
no membrane군이 생존하였다. 실험막 1개가 치유기간 중 노출, 감염되었으며, 다른 차단막은 모두 양호한 치유양상을 보였다.
조직학적 분석에서 모든 차단막은 완전히 흡수되었으며, 림프구와 다핵거대세포가 관찰되지는 않았다. 이식한 골편의 부분적 생착 및 remodelling으로 흡수율을 계산하지는 못하였다(Fig. 7).
고 찰
GBR을 사용할 경우, 골이식의 성공은 외부 세포유입을 차단하 고 충분한 기간 동안 공간을 유지시켜 주는 차단막의 능력에 달려 있다. 특히 넓은 골 결손 부위에서 차단막의 조기 흡수는 좋은 결과를 주지 못한다. 이러한 면에서 비흡수성 차단막의 장점 이 있으나, 빈번히 일어나는 연조직 열개 및 막의 노출, 그에 따른 감염 역시 골형성을 방해하므로, 적정 기간 지속되는 차단막 의 개발이 필요하다. 흡수성 차단막으로 많이 사용되는 collagen 은 type, 구조, 교차결합 정도, 처리 방법 등에 따라 조직의 수복에 다른 영향을 미친다. Collagen membrane은 뛰어난 세포 친화성 과 생체 적합성을 가지고 있지만, 대식세포와 다형핵 백혈구 작용 에 의한 빠른 biodegradation은 흡수성 차단막에서 중요한 문제 점으로 인식되고 있다[9]. 일반적으로 교차결합이 없는 collagen 인 Bio-Gide
Ⓡ는 성견 구강내에 이식하였을 때, 4주 후에 약간∼
중간정도의 흡수가 보이고, 4개월 후에는 거의 완전히 흡수된다고
알려져 있다[10]. Collagen의 분해를 감소시켜 차단막으로서의
기능을 연장시키기 위해 자외선 조사, glutaraldehyde 등의 교차
결합 방법이 개발되었으며[11], 그 이후의 연구에 의해, 몇몇 교차
Fig. 4. Histologic observation of
BioGide (arrow) at 4 weeks in bone defect model (H&E stain) (Magnifi- cation A: ×12, B: ×40, C: ×100, D:×400). Nearly complete vasculariza- tion of the membrane and severe in- filtration of infiammatory cells were observed.
Fig. 5. Histologic observation of BioMend (black arrow) at 4 weeks in bone defect
model (H&E stain) (Magnification A: ×40, B: ×100, C: ×400). Some blood vessels started to invade the membrane from the adjacent connective tissue. Moderate infiltration of multinucleated giant cells were observed (white arrow).결합 기술은 부분적으로 세포독성을 가지게 되어, 골모세포의 부착과 증식을 억제하고, 혈관화와 조직 부착을 저해하기도 한다 고 보고되었다[12].
본 연구에서도 교차결합시키지 않은 collagen membrane인 BioGide
Ⓡ가 다른 두 차단막에 비해 흡수가 빠르고 lymphocyte
의 많은 침투를 보인 반면, 교차결합을 시킨 collagen membrane
은 교차결합시키지 않은 차단막에 비해 명맥히 느린 혈관화와
분해를 보였다. 다른 논문에서도 glutaraldehyde cross-linked
mineralized polyanionic collagen membrane을 백서 피하에
이식 후 흡수율과 생체적합성을 교차결합시키지 않은 collagen
Fig. 7. Histologic observation at 10 weeks in bone augmentation model (H&E stain) (Magnification x40). The membrane has been
completely resorbed and the augmented bone is well maintained in place.Fig. 6. Histologic observation of collaguide membrane (arrow) at 4 weeks in bone
defect model (H&E stain) (Magnification A: ×40, B: ×100, C: ×400). The membrane was well maintained and showed minimal to non inflammartory response.membrane과 비교했을 때, 교차결합시키지 않은 차단막은 염증 반응과 다핵거대세포에 의한 phagocytosis가 있었고 이를 차단 막의 빠른 분해 때문인 것으로 보았다[13]. 창상 열개로 차단막이 조기에 노출되어도 교차결합된 collagen membrane은 상방의 연조직 치유가 진행되는 동안 박테리아에 의한 콜라겐용해작용을 견딜 수 있기에 더욱 안정적인 골재생을 유도할 수 있다[14].
교차결합에 의해 collagen membrane의 강도가 증가한다는 장 점도 있다[13].
BioMend
Ⓡ는 문헌에 언급된 대로 조직과의 결합에 제한이 있어 조직 검사 시 인접 결합조직과 분리되는 경향이 있었다.
이와 같은 glutaraldehyde를 이용한 교차결합은 세포독성이 있 어 차단막의 생체적합성을 떨어뜨릴 수 있다[15]. 이에 교차결합 을 하면서도, 독성이 적게 하기 위해 glutaldehyde의 농도를
낮춘 실험이 보고되기도 했다[13]. 이번 연구에서 사용된 dehy-
drotheramal treatment는 다른 교차결합 방법에 비해 세포독성
이 있는 반응물질을 사용하지 않고, 고온에 노출시키는 과정을
통해 멸균이 된다는 장점이 있다. 교차결합은 인접 콜라겐분자의
carboxyl과 amino group 사이에서 이루어지며, 온도 및 노출
시간이 증가함에 따라 collagen 섬유의 기계적 특성이 개선된다
[8]. DHT는 교차결합을 형성할 뿐 아니라, collagen을 변성시켜
collagen의 삼중나선구조가 random-chain 배열로 변화된다. 이
로 인해, 삼중나선구조에 의지하고 있는 fibroblast integrin
binding sites (α1β1과 α2β1)가 변형된다. Fibroblast의
collagen에 대한 친화성이 matrix의 견고함때문인지 혹은 콜라겐
의 표면구조의 변화때문인지 밝혀지지는 않았지만, DHT에 의해
떨어진다[16-18]. 실험막이 교차결합시키지 않은 막에 비해 느린
흡수를 보이는 것은 DHT의 이러한 물리적 성질 증가로 인한 침투성의 어려움과 세포부착성의 감소때문인 것으로 생각된다.
한편, 교차결합을 증가시키는 것은 친수성을 감소시키고, 차단막 의 stiffness를 증가사켜, 임상적으로 조작성을 떨어뜨린다고 보고 되었다[19]. 실험막은 증가된 교차결합으로 인해 적용하기 전 40 초 간의 수화시간이 필요하였으며, 수화 후 조작성이 다른 차단막 과 비교하여 떨어지지는 않았다.
실험막의 구성 성분인 atelocollagen은 collagen의 주요 anti- genic site인 telopeptide를 제거한 것으로 안전하며, 생리학적 조건이 형성되면 서로 모여 natural collagen과 같은 fiber를 형성한다. 이는 생체 내에 atelocollagen을 주입했을 때, 쉽게 용해되는 것이 아니라 오랜 기간 존재함을 의미하며, endoge- nous collagen과 같은 대사작용에 의해 분해되고 흡수되기에 sustained release carrier로 사용되고 있다[20,21].
이 실험은 DHT를 이용하여 교차결합시킨 collagen mem- brane을 임상에서 효과적으로 사용되는 collagen membrane과 비교하여 안전성, 염증반응 정도, 골재생 정도, 흡수 정도를 비교 하였다. 비록 백서의 하악골하연 골결손, 골이식 모델을 사용한 것으로 임상적으로 행해지는 GBR을 그대로 재현하지는 못했고 많은 개체의 사망으로 개체수가 부족하다는 한계가 있으나, 대조 군으로 사용한 차단막에 비해 열등하지 않음을 보여주었다.
결 론
DHT에 의하여 교차결합시킨 porcine type I atelocollagen 차단막(CollaGuide
Ⓡ)은 non cross-linked collagen 차단막인 BioGide
Ⓡ와 glutaldehyde cross-linked collagen 차단막인 BioMend
Ⓡ와 비교하여 염증반응 및 이물반응, 분해, 골형성 정도 를 비교하였을 때, 실험막은 4주 후 조직학적 소견에서, BioGide
Ⓡ
및 BioMend
Ⓡ에 비해 낮은 이물반응을 보였다. 흡수정도는 BioGide
Ⓡ에 비해 연장되었으며, BioMend
Ⓡ와 같이 10주 후에 는 완전히 흡수되었다.
CollaGuide
Ⓡ은 백서 골결손, 골이식 모델에서 Bio-Guide
Ⓡ, BioMend
Ⓡ와 유사하게 안전하고 효율적으로 골재생을 촉진시키 며, GBR에서 효과적으로 적용될 수 있을 것으로 생각된다.
References