250
책임저자: 정병욱, 경북 경주시 석장동 707번지
780-350, 동국대학교 의과대학 경주병원 외과 Tel: 054-770-8219, Fax: 054-770-8378
E-mail: [email protected]
접수일:2008년 1월 3일, 게재승인일:2008년 6월 23일
대장암의 근치적 절제술 후 재발과 관련된 혈청 CEA 의의
동국대학교 의과대학 경주병원 외과학교실
손동녕ㆍ문성욱ㆍ하동엽ㆍ정호근ㆍ정병욱
The Level of Serum CEA Associated with Recurrence after Potentially Curative Surgery for Colorectal Cancer
Dong Nyoung Son, M.D., Sung Wook Moon, M.D., Dong Yeup Ha, M.D., Ho Geun Jung, M.D., Byung Wook Jung, M.D.
Department of Sugery, Kyungju Hospital, College of Medicine, Dongguk University, Kyungju, Korea
Purpose: Carcinoembryonic antigen (CEA) is the most widely used tumor marker for detecting colorectal cancer.
This study was designed to evaluate the level of serum CEA that is associated with recurrence after potentially curative surgery for colorectal cancer.
Methods: We retrospectively investigated the pre- and post-operative levels of serum CEA in 246 patients with colorectal cancer and they had undergone potentially curative surgery from 1996 through 2005.
Results: The pre-operative CEA level was significantly associated with the number of metastatic lymph nodes, the tumor size and the recurrence rate. The feature that was associated with recurrent disease on multivariate analysis was the pre-operative level of serum CEA.
Conclusion: In order to detect the recurrence of colorectal cancer, we should closely follow up with frequent checks of the CEA level after surgery for those patients who had a high preoperative CEA level. (J Korean Surg Soc 2008;75:250-254)
Key Words: Colorectal cancer, CEA 중심 단어: 대장암, 암배아성항원
서 론
대장암은 현재 미국에서 암 사망률 2위로 흔한 질환군이 며,(1) 과거 서구에서 호발된다고 알려져 왔다. 우리나라의 경우 2002년 대장암은 전체 암 발생률과 암 사망률에서 모 두 4위를 차지하고 있으며, 꾸준히 증가하고 있는 추세 다.(2) 또 대장암은 근치적 절제술 후 재발률과 이로 인한 사망률이 높아, 재발의 조기발견이 관건이 되고 있다. 따라
서 근치적 절제술 후 추적관찰은 재발의 조기발견으로 이 어져, 재발의 근치적 치료를 위한 기회의 제공과 함께 생존 율의 증가를 가져올 수 있다.(3,4)
암배아성항원(carcinoembryonic antigen, CEA)은 1965년 대장암 환자의 혈액 및 태생기 조직에서 발견하여 명명하 였고 당시 대장암에 특이한 것으로 생각되었으나,(5,6) 여러 양성 질환, 즉 알코올성 간경변, 췌장염, 염증성장질환, 직 장용종, 고령 및 흡연자에서도 상승되는 등 낮은 민감도와 특이도로 현재 선별검사로서는 사용되고 있지 않다. 그러 나 조기진단 및 추적관찰, 재발의 조기발견의 중요성이 점 차 강조되면서 현재까지 널리 사용되고 있다. 대장암 환자 의 수술 전 CEA치는 절대적 수치보다는 향후 이 수치의 변 화를 확인하여 추적 조사하는 데 중요성이 있다. 또한 수술
Table 1. Relationship between preoperative CEA level and patho- clinical variables
<5 ng/ml (n=130) ≥5 ng/ml (n=116)
Variable P-value
n (%) n (%)
Tumor location 0.086
Right colon 36 (27.7) 46 (39.7) Left colon 49 (37.7) 31 (26.7)
Rectum 45 (34.6) 39 (33.6)
Differentiation 0.74
Well 48 (36.9) 32 (27.6)
Moderate 55 (42.3) 71 (61.2) Poorly 19 (14.6) 5 (4.3) Mucinous 8 (6.2) 8 (6.9)
LN* invasion <0.05
1∼3 28 (21.5) 32 (27.6)
≥4 15 (11.5) 60 (51.7)
LN region 0.56
I 20 (15.4) 42 (36.2)
II 23 (17.7) 50 (43.1)
Tumor size <0.05
<5 cm 88 (71.0) 42 (34.4)
≥5 cm 36 (29.0) 80 (65.6)
Recurrence <0.05
No 110 (84.6) 41 (35.3)
Yes 20 (15.4) 75 (64.7)
Serum CEA level at recurrence <0.01
<5 ng/ml 9 (50.0) 11 (14.3) ≥5 ng/ml 9 (50.0) 66 (85.7)
*LN = lymph node; n = number.
전 이 수치의 증가는 간 전이 유무의 평가에도 도움을 주며, 환자의 근치적 절제술을 포함한 적절한 치료 이후 재발에 대한 추적조사의 지표로 중요하게 사용되고 있다.(7,8) 따라 서 수술 전, 후의 혈청 CEA치가 재발과 관련된 예후 인자로 서 의의가 있는지에 대해, 본 병원에서 임상 환자들의 후향 적인 분석을 토대로 문헌고찰과 함께 보고하는 바이다.
방 법
1996년 1월부터 2005년 12월까지 대장암으로 진단받고 근치적 절제술을 시행한 환자 중 추적조사가 가능한 환자 246명의 의무기록을 참고로 후향적 조사를 실시하였다. 모 든 환자는 수술 전 혈청 CEA치를 검사하고 추적조사 시에 는 수술 후 처음 2년간은 약 3개월 간격으로, 그 후 약 6개 월 간격으로 혈청 CEA치를 측정하였다. 본 연구는 5.0 ng/ml을 정상 참고치로, 수술 전에 CEA 5.0 ng/ml 이상인 군과 그렇지 않는 군으로 분류하여, 암의 위치, 크기와 조직 학적 분화도, 전이 림프절의 수, 림프절 위치 등과의 연관성 을 비교하고, 수술 후, 추적 관찰 시 CEA의 상승과 재발률 과의 관계, 전이 병소별 차이 등의 연관성에 대해 그 의의를 분석하였다. 단변량 분석을 통해 확인된 각 인자에 대해서 는 재발과 관련된 예후 인자를 분석하기 위해 로지스틱 회 귀분석을 이용한 다변량 분석을 시행하였다. 통계처리는 SPSS 12.0 프로그램을 참고하여 상관관계 분석은 Chi-square test를 이용하였다. P값이 0.05 미만일 때 유의성이 있는 것 으로 하였다.
결 과
1) 성별 및 연령별 분포
본 연구에서의 남녀 비는 101:145로 여자가 많았고, 50 세 이상인 경우가 202명(82.1%)으로 대다수를 차지하였다.
2) 발생 부위별 증상과 빈도
암의 발생 부위별로 볼 때 우측 대장이 83예, 좌측 대장이 79예, 직장이 84예였으며, 증상은 우측 대장의 경우 주로 복 부동통, 종괴의 촉지, 장폐색 순이었고, 좌측 대장에서는 변 비, 통증이 직장에서는 혈변, 변비 등이 주증상이었다.
3) 암의 발생 부위별 수술 전 CEA치
수술 전 CEA치가 5.0 ng/ml 이상일 때 의의 있는 증가로
하여 양성률을 비교하였는데, 수술 전 116명에서 증가하여 47.2%의 양성률을 보여 수술 전 혈청 CEA치는 진단적 유용 성은 없었으며, 또한 종양의 위치에 따른 CEA치의 차이가 없었다(P=0.086)(Table 1).
4) 조직학적 분화도에 따른 수술 전 CEA치의 양성률
조직학적 분화도에 따른 수술 전 CEA치의 양성률은 고 분화형 선암에서 40%, 중등도 분화형 선암에서 56.3%, 저분 화형 선암에서 20.8%, 점액성 선암의 경우 50%로 조직학적 분화도에 따른 수술 전 CEA치의 양성률과는 연관관계가 없었다(P=0.74)(Table 1).
5) 림프절 전이 개수와 수술 전 CEA치의 양성률
림프절 전이를 기준으로 전이 음성군, 3개 이하군, 4개 이 상 림프절 전이군으로 나누었고, 각각의 수술 전 CEA치의 양성률은 21.6%, 53%, 80%로 림프절 전이가 많을수록 CEA치 의 양성률이 증가되는 양상을 보여주었다(P<0.05)(Table 1).
Table 2. Multivariate analysis of features associated with recurrent disease
Odds ratio 95% Confidence interval P-value Preoperative CEA
4.318 1.710∼10.902 0.002
(≥5 ng/ml) Number of lymph
1.767 0.778∼4.012 0.174
nodes (≥4) Tumor size
1.995 0.840∼4.742 0.118
(≥5 cm)
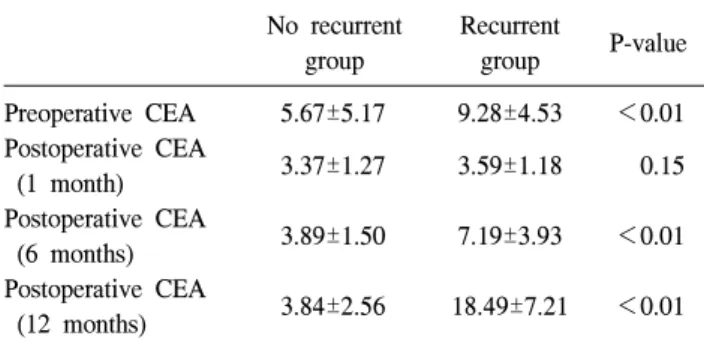
Table 3. Preoperative and postoperative CEA level (ng/ml) No recurrent Recurrent
P-value
group group
Preoperative CEA 5.67±5.17 9.28±4.53 <0.01
Postoperative CEA
3.37±1.27 3.59±1.18 0.15 (1 month)
Postoperative CEA
3.89±1.50 7.19±3.93 <0.01
(6 months) Postoperative CEA
3.84±2.56 18.49±7.21 <0.01 (12 months)
Table 4. Calculation of sensitivity, specificity and predictive value Recurrence
CEA level
Present Absent
CEA elevated 75 A (true positive)
29 B (false positive)
CEA not elevated 20 C (false negative)
122 D (true negative)
Sensitivity=A/(A+C)×100%=78.9%; Specificity=D/(B+D)×100%=
80.8%; Positive predictive value=A/(A+B)×100%=72.1%.
6) 림프절 전이의 부위에 따른 수술 전 CEA치의 상관관계
림프절 전이 부위를 대장 벽과 대장 주위 림프절을 I군으 로, 대장에 혈류를 공급하는 주 혈관 주위의 림프절을 II군 으로 나누고 비교해 보았을 때 양성률이 각각 67.7%, 68.5%
로 수술 전 CEA치는 림프절 전이의 부위에 따른 유의한 상 관관계를 보여주지 못했다(P=0.56)(Table 1).
7) 종양의 크기와 수술 전 CEA치의 상관관계
종양의 크기를 5 cm 미만과 5 cm 이상의 군으로 나누고 수술 전 혈청 CEA치와의 상관성을 분석한 결과 혈청 CEA 치의 양성률은 각각 29%, 65.6%로 의미 있는 상관관계를 보여주었다(P<0.05)(Table 1).
8) 수술 전 CEA치와 암의 재발률
암의 재발과 수술 전 혈청 CEA치의 양성률을 보면 총 재 발 환자 95명 중 수술 전 CEA치가 5 ng/ml 이상 시 재발률 은 64.7%였고 5 ng/ml 미만 시 15.4%로써 수술 전 혈청 CEA 치의 상승에 따른 재발률의 증가는 의의가 있었다(P<0.05) (Table 1).
9) 암의 재발군에 있어 수술 전 CEA치와 수술 후 재발 시 CEA치의 양성률
재발한 총 95명 중 수술 전 혈청 CEA치가 5 ng/ml 이상인 환자는 77명으로 이들 중 재발 시 5 ng/ml 이상이 66명 (85.7%)이었다. 수술 전 혈청 CEA치가 5 ng/ml 미만인 환자 18명 중 재발 시 5 ng/ml 이상인 경우가 9명(50%)으로 수술 전 혈청 CEA치가 증가했던 군에서 수술 전 혈청 CEA치가 정상인 군보다 재발 시 혈청 CEA 증가가 유의하게 많았다 (P<0.05)(Table 1).
10) 대장암과 관련된 재발 인자의 다변량 분석
수술 전과 후 혈청 CEA 수치와 단변량 분석에서 통계학 적으로 유의하였던 림프절 전이 개수와 종양의 크기에 대 해 다변량 분석을 시행하였다. 그 결과로 수술 전과 후, 혈 청 CEA 수치(5 ng/ml 이상)가 의미 있는 P-value를 보였으 며, 교차비가 각각 4.318, 5.002이었다(Table 2).
11) 재발군 및 비재발군의 수술 전, 후 혈청 CEA 수치
비재발군 환자의 수술 전 혈청 CEA 수치는 5.67±5.17 ng/ml이고 수술 후 1개월째 혈청 CEA 수치는 3.37±1.27 ng/ml였다. 수술 후 6개월째의 혈청 CEA 수치는 3.89±1.50 ng/ml였으며, 12개월째의 혈청 CEA 수치는 3.84±2.56 ng/ml 였다. 한편, 재발군의 환자의 수술 전 혈청 CEA 수치는 9.28±4.53 ng/ml이고 수술 후 1, 6, 12개월의 혈청 CEA 수치 는 각각 3.59±1.18 ng/ml, 7.19±3.93 ng/ml, 18.49±7.21 ng/ml 였다. 따라서, 수술 후 1개월째의 두 그룹 간의 혈청 CEA 수치는 음성치로서, 유의한 차이를 보이고 있지 않았다 (Table 3). 수술 후 재발 시의 혈청 CEA수치는 32.24±23.26 ng/ml였으며, 이 때 무병생존기간은 18.00±5.68개월이었다.
한편, 재발군에서 수술 전 혈청 CEA 음성치(5 ng/ml 미만)
인 환자는 20명으로 무병생존기간은 22.91±4.54개월이었 고, 수술 전 혈청 CEA 양성치(5 ng/ml 이상)인 환자는 75명 으로 무병생존기간은 16.70±5.23개월로 유의한 차이를 보 였다(P<0.01).
12) 암의 재발에 있어 CEA치 측정의 민감도, 특이도, 양 성 예측치
암의 재발에 있어 혈청 CEA치 측정의 민감도, 특이도, 양 성 예측치를 계산해 보았을 때, 민감도 78.9%, 특이도 80.8%, 양성 예측치 72.1%로 비교적 높은 비율을 보였다(Table 4).
고 찰
CEA는 180,000 dalton 정도의 당단백질로, 대개 장세포의 당의(glycocalyx)표면에서 혈중으로 유리되며, 반감기는 1.2 일에서 88.1일 사이로 평균 4.4일로 보고되고 있으며, 대장 암 환자에서는 60∼90%에서 CEA치가 5 ng/ml 이상으로 증 가되는 것으로 보고되고 있다.(9-11) 1965년 처음으로 발견 된 이후, 대장암 환자의 관리에 있어서 혈청 CEA는 암의 병기와 예후를 예측하고 수술 후의 정기적인 추적관찰로서 재발 및 전이의 조기 예측 등을 위한 검사로 보편적으로 활발히 이용되고 있다. 혈청 CEA치의 양성치는 검사실 기 준에 따라 혈중 농도 2.5 ng/ml에서 5.0 ng/ml 사이의 값에서 정하고 있으며,(9) 대부분은 2.5 ng/ml 혹은 5.0 ng/ml 이상을 양성이라고 판정하고 있어, 저자들의 연구에서 검사실에서 는 5.0 ng/ml를 기준치로 설정하고 있다. 보통 근치적 절제 술 후 혈청 CEA 수치가 1개월에 정상치로 돌아오며 늦어도 3개월내에 정상 범위가 된다고 한다. 그래서 근치적 절제술 후 정상치로 돌아오는 것은 암종괴의 완전 제거를 의미한 다고 하였으며,(12) 절제술 후 하강이 안되는 경우는 종괴 가 남아 있거나 전이성 병변의 출현을 의미한다고 하였 다.(13)
본 연구의 결과에 따르면, 발생부위에 따른 수술 전 혈청 CEA치의 양성률은 차이가 없었다. 조직학적 분화도와 수 술 전 혈청 CEA치도 상관관계가 없는 것으로 나타났다. 조 직학적 분화도에 따른 수술 전 혈청 CEA치의 양성률은 많 은 연구에서 연관성이 없는 것으로 보고되고 있다.(14-17) 한편으로 다른 저자들은 고분화암에 혈청 CEA치 생산이 많고, 저분화암에 생산이 적다고 하였고, 한편으로는 공격 적인 고분화암은 종괴가 적어 혈청 CEA 상승이 없고, 진행 성 저분화암은 심한 조직침투와 큰 종괴로 말미암아 혈중
CEA치의 상승이 있을 수 있다고도 하였다.(18,19) 수술 전 혈청 CEA 수치와 림프절 전이와의 관계를 보면, 다른 저자에 의하면 혈청 CEA치 양성인 경우 림프절 전이 가 1∼3개 52.3%, 4∼9개 33.3%, 10개 이상 13.3%, 혈청 CEA치 음성인 경우 62.5%, 12.5%, 25%로 두 관계는 차이가 없는 것으로 보고하고 있다.(20) 저자의 경우는 혈청 CEA 치가 양성인 경우 1∼3개 27.6%, 4개 이상이 51.7%, 혈청 CEA치가 음성인 경우 1∼3개 21.5%, 4개 이상이 11.5%로 양성과 음성인 군 간에 유의한 차이를 보이고 있다. 하지만, 재발과 관련하여 다변량 분석에서 림프절 전이 4개 이상 시 재발 인자로서 유의한 인자는 아닌 것으로 나타났다.
수술 전 혈청 CEA 수치와 종양의 크기의 관계를 보면, 다른 저자에 의하면 종양의 크기가 클수록 혈청 CEA 수치 의 양성률이 증가한다고 보고하고 있고,(21) 본 연구에서의 결과와 일치했다. 하지만, 종양의 크기(5 cm 이상)는 재발 인자로서는 유의한 인자가 아닌 것으로 나타났다.
수술 후 재발과 관련된 예후 인자를 위한 다변량 분석에 서는 수술 전 CEA (5 ng/ml 이상)가 통계적으로 유의한 결 과를 보였다. 수술 전 혈청 CEA치에 따른 재발률을 비교하 면 수술 전 혈청 CEA치가 5 ng/ml 미만인 경우 재발률이 15.4%이고 반면에 수술 전 혈청 CEA치가 5 ng/ml 이상인 경우 재발률이 64.7%였다. 수술 후 혈청 CEA 수치의 변화 에 따른 재발과의 관계도 상관관계가 있는 것으로 분석되 었다. 수술 후 1, 6, 12개월째의 CEA 수치를 비교했을 때 재발군이 비재발군보다 평균 CEA 수치 변동 폭이 큰 것으 로 보아 임상적으로 혈청 CEA의 양성치만큼 절대 수치의 증가 양상에 대해서도 의의가 있는 것으로 판단된다.
한편, 수술 전 혈청 CEA치의 양성 유무에 따라 무병생존 기간도 영향을 미치는 것으로 분석되었다. 수술 전 혈청 CEA 음성치(5 ng/ml 미만)인 환자는 무병생존기간이 22.91±
4.54개월이었고, 수술 전 혈청 CEA 양성치(5 ng/ml 이상)인 환자는 무병생존기간이 16.70±5.23개월로 유의한 차이를 보였다(P<0.01). 이는 수술 전 혈청 CEA치가 높으면, 수술 후 재발 가능성이 높아질 것으로 예측할 수 있다고 본 다.(22)
결 론
수술 전 혈청 CEA 수치가 높다면, 수술 후 재발 가능성이 많으므로, 수술 후 혈청 CEA치를 정기적으로 자주 검사하 여야 하며, 검사치의 상승이 있을 경우 반복하여 검사 수치
상승을 확인하고 복합적인 임상적 평가를 시행하여 대장암 의 재발을 조기에 진단할 수 있을 것으로 생각한다.
REFERENCES
1) Merrie AE, van Rij AM, Dennett ER, Phillips LV, Yun K, McCall JL. Prognostic significance of occult metastases in co- lon cancer. Dis Colon Rectum 2003;46:221-31.
2) Ministry of Health and Welfare. Journal of Korean Cancer Research Association. 2003
3) Safi F, Link KH, Beger HG. Is follow-up of colorectal cancer patients worthwhile? Dis Colon Rectum 1993;36:636-43.
4) Tornqvist A, Ekelund G, Leandoer L. The value of intensive follow-up after curative resection for colorectal carcinoma. Br J Surg 1982;69:725-8.
5) Gold P, Freedman SO. Demonstrations of tumor specific anti- gens in human colonic carcinomata by immunological toler- ance and absorption techniques. J Exp Med 1965;121:439-62.
6) Gold P, Freedman SO. Specific carcinoembryonic antigens of the human digestive system. J Exp Med 1965;122:467-81.
7) Bakalakos EA, Burak WE Jr, Young DC, Martin EW Jr. Is carcino-embryonic antigen useful in the follow-up manage- ment of patients with colorectal liver metastases? Am J Surg 1999;177:2-6.
8) Bast RC Jr, Ravdin P, Hayes DF, Bates S, Fritsche H Jr, Jessup JM, et al. 2000 update of recommendations for the use of tumor markers in breast and colorectal cancer: clinical prac- tice guidelines of the American Society of Clinical Oncology.
J Clin Oncol 2001;19:1865-78.
9) Won WJ, Yoo TM, Kim HJ, Seo IT. Consideration about the normal range of carcinoembryonic antigen. Korean Soc Nucl Med Tech 1999;4:69-72.
10) Belluco C, Nitti D, Frantz M, Toppan P, Basso D, Plebani M, et al. Interleukin-6 blood level is associated with circulat- ing carcinoembryonic antigen and prognosis in patients with colorectal cancer. Ann Surg Oncol 2000;7:133-8.
11) Choi JS, Min JS. Significance of postoperative serum level of caricinoembryonic antigen (CEA) and actual half life of CEA in colorectal cancer patients. Yonsei Med J 1997;38:1-7.
12) Lo gerfo P, Herter FP. Carcinoembryonic antigen and prog- nosis in patients with colon cancer. Ann Surg 1975;181:81.
13) Herrea MA, Chu TM, Hylyoke ED. Carcinoembryonic antigen (CEA) as a prognostic and monitoring test in clinically com- plete resection of colorectal carcinoma. Ann Surg 1976;183:
5-9.
14) Laurence DJ, Stevens U, Bettelheim R, Darcy D, Leese C, Turberville C, et al. Role of plasma carcinoembryonic antigen in diagnosis of gastrointestinal, mammary and bronchial carci- noma. Br Med J 1972;3:605-9.
15) Livingstone AS, Hampson LG, Shuster J, Gold P, Hinchey EJ.
Carcinoembryonic antigen in diagnosis and management of colorectal carcinoma. Arch Surg 1974;109:259-64.
16) Surgarbaker PH, Skarin AT, Zamcheck N. Pattern of serial CEA assays and their clinical use in management of colorectal cancer. J Surg Oncol 1976;8:523-37.
17) Yun YW, Yu HC, Kim JH, Hwang Y. Clinical value of pre-and post-operative serum carcinoembryonic antigen in col- orectal cancer. J Korean Soc Coloproctol 1997;13:573-82.
18) Livingstone AS, Hampson LG, Shuster J, Gold P, Hinchey F.
Carcinoembryonic antigen in the diagnosis and management of colorectal carcinoma. Current status. Arch Surg 1974;109:259- 64.
19) Martin EW, Mintion JP, Carey LC. CEA-directed second-look surgery in the asymptomatic patient after primary resection of colorectal carcinoma. Ann Surg 1985;202:310-7.
20) Lee BH, Jang YC, Woo JH, Lee CY, Lee JS. The significance of preoperative carcinoembryonic antigen levels in prognosis and second look operation of colorectal cancer. J Korean Surg Soc 1986;31:64.
21) Moertel TL, O'Fallon JR, Go VL, O'Connell MJ, Thynne GS.
The preoperative carcinoembryonic antigen test in the diag- nosis, staging, and prognosis of colorectal cancer. Cancer 1986;58:603-10.
22) Wolmark N, Fisher B, Wiend S, Henry RS, Lerner H, Legault- Poisson S, et al. The prognostic significance of preoperative carcinoembryonic antigen levels in colorectal cancer. Results from NSABP (National Surgical Adjuvant Breast and Bowel Project) clinical trials. Ann Surg 1984;199:375-84.