대한소화기학회지 2006;47:449-453
INTRODUCTION
Since the esophagus is a longitudinal tubular organ located near the central axis of the thorax, it is usually irradiated during radiotherapy for intrathoracic malignancies such as lung cancer, lymphoma or thymoma. The CyberKnife is an image-guided robotic system consisted of a compact linear accelerator, and designed for stereotactic radiosurgery. It was first developed for the treatment of both benign and malignant intracranial lesions.1,2 The CyberKnife has been used to treat unresectable primary or metastatic cancers and tumors of spine, lung, and head/neck region. Recently, many centers have started using the CyberKnife to treat primary or metas- tatic hepatic tumors. However, experience with radiosurgery for the treatment of these lesions is still limited, and only few
complications are reported yet due to its short clinical experience. Here, we report a 72-year-old man who developed localized esophageal ulcerations after CyberKnife treatment for metastatic hepatic tumor of colon cancer. To our knowledge, this is the first report of esophageal ulcerations developed after the CyberKnife treatment for metastatic hepatic tumor in Korea.
CASE REPORT
A 72-year-old man visited our hospital with complaints of abdominal pain and prolonged hematochezia for 1 month. He had anemia with a hemoglobin level of 9.9 g/dL. Gastroscopy revealed active gastric ulcer on antrum and colonoscopy revealed ulcero-fungating mass on hepatic flexure nearly
대장암의 간 전이에 대한 사이버나이프 치료 후 발생한 국소 식도궤양 1예
한양대학교 의과대학 내과학교실
정용우․한동수․백창희․김종표․최정혜․손주현․함준수
Localized Esophageal Ulcerations after CyberKnife Treatment for Metastatic Hepatic Tumor of Colon Cancer
Yong Woo Chung, M.D., Dong Soo Han, M.D., Chang Hee Paik, M.D., Jong Pyo Kim, M.D., Jung Hye Choi, M.D., Joo Hyun Sohn, M.D., and Joon Soo Hahm, M.D.
Department of Internal Medicine, Hanyang University College of Medicine, Seoul, Korea
CyberKnife is an image-guided robotic system designed for stereotactic radiosurgery. It uses the combination of robotics and image guidance to deliver concentrated and accurate beams of radiation to intracranial and extra- cranial targets. Although the frameless nature of the CyberKnife allows tumors in the chest and abdomen to be treated as well, complications associated with CyberKnife treatment have not been established yet due to its short clinical experience. We describe a case of localized esophageal ulcerations after CyberKnife treatment for metastatic hepatic tumor of colon cancer. (Korean J Gastroenterol 2006;47:449-453)
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
Key Words: Esophageal ulcer; The CyberKnife; Metastatic hepatic tumor
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ Correspondence to: Dong Soo Han, M.D.
Department of Internal Medicine, Hanyang University Guri Hos- pital, 249-1 Gyomun-dong, Guri 471-701, Korea
Tel: +82-31-560-2226, Fax: +82-31-555-2998 Email: [email protected]
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ 접수: 2005년 4월 11일, 승인: 2005년 10월 4일 연락처: 한동수, 471-701, 경기도 구리시 교문동 249-1
한양대학교 구리병원 내과
Tel: (031) 560-2226, Fax: (031) 555-2998 Email: [email protected]
450 대한소화기학회지: 제47권 제6호, 2006
obstructing the lumen (Fig. 1). Colonoscopic biopsy showed moderately well differentiated adenocarcinoma. Serum carcino- embryonic antigen (CEA) level was elevated to 110.4 ng/mL.
Abdominal CT showed ascending colon carcinoma of 5 cm in length with hepatic metastasis. He refused all the surgical treatments and was started with oral chemotherapy with XelodaⓇ (capecitabine) in a dose of 2,500 mg/m2/day at oncology department. Fourteen-days of XelodaⓇ treatment in 3 weeks interval was continued for 3 cycles until mechanical ileus was developed due to the progression of colon cancer.
He underwent surgical treatment to relieve the obstruction of colon. Right hemicolectomy and right lobectomy of liver were done. He finished 7 more cycles of XelodaⓇ treatment after the operation. Serum CEA level decreased to normal level of 4.7 ng/mL. Abdominal CT taken at 10 months after the operation revealed newly developed hepatic mass of 4 cm in length at segment II (Fig. 2). Serum CEA level increased to 11.0 ng/mL. Radiofrequency thermal ablation (RFTA) for hepatic mass was attempted. However, it was failed due to poor ultrasonic windows. CyberKnife treatment was done for 3 days. Total dose of 3,600 cGy was given to the hepatic lesion. Abdominal CT taken 10 days after the CyberKnife treatment revealed decreased size of metastatic hepatic tumor (Fig. 3). After 2 weeks of the CyberKnife treatment, he complained of severe epigastric soreness and heart-burn sensation. Gastroscopy revealed localized lower esophageal ulcerations with clear margin (Fig. 4). Ulcerations were 3 cm-segment in length and well demarcated from normal eso- phageal mucosa. Damaged esophageal mucosa was coated with thick exudates and superficial hemorrhages, which was scored 3 according to the Kuwahata's score.3 Gastric mucosa was congested with multiple focal erythemas. Esophageal biopsy showed superficial ulcerations without evidence of infection or malignant invasion (Fig. 5). He is now under the treatment of high dose proton pump inhibitor (PPI), with the improvement of symptoms. Regular endoscopic follow up is planned to monitor the development of esophageal stricture.
Fig. 1. Colonoscopic view of colon cancer. It shows an ulcero- fungating mass on hepatic flexure with nearly obstructing the lumen. Its surface is friable and hemorrhagic.
Fig. 2. Abdominal CT taken at 10 months after the operation. It shows a newly developed hepatic mass of 4 cm in length at segment II. It appears as low density in portal phase scan and diffuse high density in delayed phase scan. No definite lympha- denopathy is noted.
Fig. 3. Abdominal CT taken after the CyberKnife treatment. It shows slightly decreased size of hepatic mass at segment II.
Enhancing density of hepatic mass is also decreased. Suspicious thickening of lower esophageal wall with slightly increased en- hancement is noted.
정용우 외 6인. 대장암의 간 전이에 대한 사이버나이프 치료 후 발생한 국소 식도궤양 1예 451
DISCUSSION
CyberKnife is a unique image-guided frameless stereotactic radiosurgery delivery system. This system uses a lightweight, band linear accelerator, computer-controlled robotic arm, a pair of orthogonal X-ray imagers target locating system (TLS), and a computer workstation. The CyberKnife consists of a 6-MV compact linear accelerator that is smaller and lighter than linear accelerators used in conventional radiotherapy.4-6 The smaller size allows it to be mounted on a computer-
controlled six-axis robotic manipulator that permits a much wider range of beam orientation than can be achieved with conventional radiotherapy devices.
The system can be adapted to patient's position change during the treatment by acquiring targeting images repeatedly and by adjusting the direction of the treatment beam. The treatment beam can be maneuvered and pointed nearly any- where in space. Treatment beams are not confined to isocen- tric geometry, so that they can be arranged in complex over- lapping patterns which confirm to irregularly shaped tumor volumes.7 An analysis for the accuracy of the CyberKnife radiosurgery system found that the machine has a clinically relevant accuracy of 1.1±0.3 mm, with a 1.25 mm CT slice thickness.7-10
The CyberKnife has been used to treat unresectable primary or metastatic cancers. It has been used to treat tumors of the spine, lung, and head/neck region.10-13 Recently, many centers have started using the CyberKnife to treat primary or meta- static liver cancers with early encouraging results, which are not published yet.
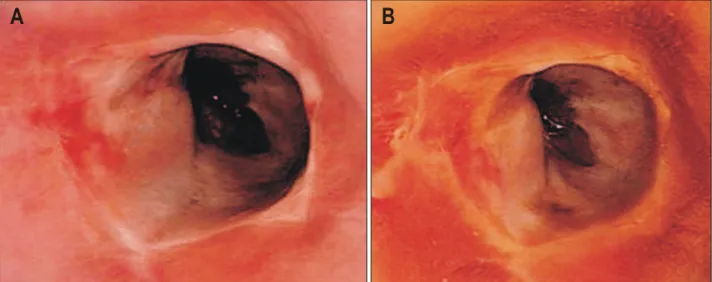
Reports about complications after the CyberKnife treatment are hard to find due to its short clinical experience. In a study of 61 patients with glioma and glioblastoma treated with the CyberKnife, only four patients showed symptomatic radiation necrosis.11 In the study of 51 patients with 72 spinal tumors (58 metastatic and 14 primary), three cases of self-limited Fig. 4. Gastroscopic view of esophageal ulcerations. (A) It shows localized lower esophageal ulcerations with clear margin. Ulcerations are 3 cm in length and well demarcated from surrounding normal esophageal mucosa. Damaged esophageal mucosa is coated with thick exudates and superficial hemorrhages. (B) Gastroscopic view of esophageal ulcerations stained with Lugol solution. It shows that damaged esophageal mucosa is not stained in contrast to the stained normal mucosa. This is more confirmative for sharp demarcation between normal mucosa and localized esophageal ulcerations.
A B
Fig. 5. Microscopic finding of esophageal ulcerations. It demon- strates ulcer detritus composed of fibrinoid material and cellular debris devoid of malignant cells (H&E stain, ×200).
452 The Korean Journal of Gastroenterology: Vol. 47, No. 6, 2006
dysphagia, two cases of diarrhea, three cases of lethargy, one case of paresthesias, and one case of wound dehiscence were reported.12 In a study of 23 lung tumors (8 metastatic and 15 primary), only four complications were related to fiducial placement.13 Besides the CyberKnife treatment, a study of conventional stereotactic radiosurgery for primary or metastatic cancers of lung and liver showed that it is locally effective treatment with local control rates of 76% after 1 year and 61-76% after 2 years without relevant acute toxicity.14 Chro- nic esophageal ulceration occurred in one patient 3 months after the treatment. As the mechanisms of the conventional stereo- tactic radiosurgery and CyberKnife are similar, esophageal ulceration can be a complication of the CyberKnife treatment for metastatic or primary lung and liver tumors. In presenting case, esophageal ulcerations occurred shortly after the CyberKnife treatment, when the patient was not in XelodaⓇ treatment. In addition, there was neither evidence of infection nor malignant invasion in esophageal biopsy. Most impor- tantly, sharply demarcated margin of esophageal ulcerations from normal mucosa strongly suggests that radiation would be the cause.
Radiation esophagitis remains the primary dose-limiting acute toxicity in the radiotherapeutic management of thoracic neoplasms. After 2 to 3 weeks of conventional fractionated radiotherapy, patients often complain of dysphagia and/or odynophagia. This acute reaction can cause significant morbi- dity from dehydration and weight loss that can lead to treat- ment interruptions. In rare instances, patients may experience perforation or obstruction. The late reactions of the esophagus to radiation usually involve fibrosis which can lead to stric- ture. However, radiation esophagitis would not be an obstacle in radiotherapy since these are less symptomatic and easily reversible. Patients who scored as endoscopic grade 2 accor- ding to the Kuwahata's score3 usually recovered within a few weeks of conservative treatment, but prolongation of injury healing may develop in patients with grade 3 or more.15 There are case reports of esophageal stricture after long latent inter- vals.16-18
Although accurate volumetric parameters have yet to be defined, minimizing the amount of esophagus irradiation is an obvious mean of preventing radiation esophagitis. Unfortuna- tely, this is often impossible for the treatment of thoracic malignancies due to the anatomic distribution of the great vessels and clinical target volume. A number of conservative therapeutic interventions have been tried with variable success
for the resolution of symptomatic radiation esophagitis, including antacids or solutions containing equal parts of viscous xylo- caine, oral liquid morphine sulfate and acetaminophen.19 Recently, several randomized trials have studied the role of amifostine, a radioprotector, in the setting of lung cancer, but its efficacy has not been established yet.20 In presenting case, we started PPI treatment due to severe symptom and high endoscopic score of the patient, although efficacy of PPI in radiation esophagitis is not confirmed yet. Anyway, symptoms are improving slowly after PPI treatment, and further studies would be necessary to clarify the efficacy of PPI on radiation esophagitis.
In conclusion, the CyberKnife is a promising treatment mo- dality for unresectable cancers, especially for the cancers of spine, lung, and liver. Esophageal ulcerations can occur shortly after the treatment, especially when the treatment targets are in close proximity to the mediastinum. If patients who have underwent the CyberKnife treatment for lung and liver tumors complain of epigastric pain, endoscopy should be performed to find any esophageal mucosal injury, and long-term follow up endoscopic surveillance is needed to monitor the develop- ment of esophageal stricture. Additional work remains to be performed before biological modifiers, such as radioprotectors, become a more integral part of the therapy.
요 약
사이버나이프는 정위 방사선 수술을 위하여 고안된 영상에 의해 유도되는 일종의 로봇 시스템이다. 사이버나이프는 초 기에는 주로 두개 내 양성 또는 악성 병소를 치료하기 위하 여 개발되었으나 방사선 조사 때 틀이 필요없다는 이점으로 인해 최근에는 흉부와 복부의 종괴 치료에 도입되었다. 하 지만 이에 대한 임상 경험은 아직까지 제한적이어서 이러한 치료에 의한 합병증 보고 또한 많지 않다. 저자들은 대장암 의 간 전이에 대한 사이버나이프 치료 후 발생한 국소 식도 궤양 1예를 경험하여 보고한다.
REFERENCES
1. Adler JR Jr, Chang SD, Murphy MJ, Doty JR, Geis P, Hancock SL. The CyberKnife: a frameless robotic system for radiosurgery. Stereotact Funct Neurosurg 1997;69:124-128.
2. Adler JR Jr, Murphy MJ, Chang SD, Hancock SL. Image- guided robotic radiosurgery. Neurosurgery 1999;44:1299-1307.
3. Kuwahata N. The clinical investigation of radiaton esopha-
Chung YW, et al. Localized Esophageal Ulcerations after CyberKnife Treatment 453
gitis. Kagoshima Daigaku Igaku Zasshi 1980;32:281-307.
4. Adler JR, Cox RS, Kaplan I, Martin DP. Stereotactic radio- surgical treatment of brain metastases. J Neurosurg 1992;76:
444-449.
5. Guthrie BL, Adler JR Jr. Computer-assisted preoperative plan- ning, interactive surgery, and frameless stereotaxy. Clin Neu- rosurg 1992;38:112-131.
6. Murphy MJ, Cox RS. The accuracy of dose localization for an image-guided frameless radiosurgery system. Med Phys 1996;23:2043-2049.
7. Ryu SI, Chang SD, Kim DH, et al. Image-guided hypo- fractionated stereotactic radiosurgery to spinal lesions. Neuro- surgery 2001;49:838-846.
8. Chang SD, Adler JR. Current status and optimal use of radio- surgery. Oncology 2001;15:209-221.
9. Chang SD, Main W, Martin DP, Gibbs IC, Heilbrun MP. An analysis of the accuracy of the CyberKnife: a robotic frame- less stereotactic radiosurgical system. Neurosurgery 2003;52:
140-147.
10. Gerszten PC, Ozhasoglu C, Burton SA, et al. CyberKnife frameless stereotactic radiosurgery for spinal lesions: clinical experience in 125 cases. Neurosurgery 2004;55:89-98.
11. Sato K, Baba Y, Inoue M, Omori R. Radiation necrosis and brain edema association with CyberKnife treatment. Acta Neurochir 2003;86(suppl):513S-517S.
12. Degen JW, Gagnon GJ, Voyadzis JM, et al. CyberKnife stereotactic radiosurgical treatment of spinal tumors for pain
control and quality of life. J Neurosurg Spine 2005;2:540- 549.
13. Whyte RI, Crownover R, Murphy MJ, et al. Stereotactic radiosurgery for lung tumors: preliminary report of a phase I trial. Ann Thorac Surg 2003;75:1097-1101.
14. Wulf J, Hadinger U, Oppitz U, Thiele W, Ness-Dourdoumas R, Flentje M. Stereotactic radiotherapy of targets in the lung and liver. Strahlenther Onkol 2001;177:645-655.
15. Hirota S, Tsujino K, Hishikawa Y, et al. Endoscopic findings of radiation esophagitis in concurrent chemoradiotherapy for intrathoracic malignancies. Radiother Oncol 2001;58:273-278.
16. Choy H, Akerley W, Safran H, et al. Multiinstitutional phase II trial of paclitaxel, carboplatin, and concurrent radiation therapy for locally advanced non-small-cell lung cancer. J Clin Oncol 1998;16:3316-3322.
17. Mahboubi S, Silber JH. Radiation-induced esophageal stric- tures in children with cancer. Eur Radiol 1997;7:119-122.
18. Vanagunas A, Jacob P, Olinger E. Radiation-induced esopha- geal injury: a spectrum from esophagitis to cancer. Am J Gastroenterol 1990;85:808-812.
19. Trowers E, Thomas C Jr, Silverstein FE. Chemical- and radia- tion-induced esophageal injury. Gastrointest Endosc Clin N Am 1994;4:657-675.
20. Bradley J, Movsas B. Radiation esophagitis: predictive factors and preventive strategies. Semin Radiat Oncol 2004;14:280- 286.