이하선 천엽에 발생한 상피-근상피암종의 치험례
진선미·유현호·류석환·신동윤·황희성·김철훈·김복주 동아대학교 의료원 치과 구강악안면외과
Abstract(J Korean Assoc Oral Maxillofac Surg 2011;37:505-9)
Epithelial-myoepithelial carcinoma on the superficial lobe of the parotid gland: a case report
Sun-Mi Jin, Hyun-Ho Ryu, Seok-Hwan Ryu, Dong-Yoon Shin, Hie-Sung Hwang, Chul-Hoon Kim, Bok-Joo Kim Department of Oral and Maxillofacial Surgery, Department of Dentistry, Dong-A University Medical Center, Busan, Korea
Epithelial-myoepithelial carcinoma (EMC) is a low-grade malignant salivary gland neoplasm that was first described in 1972. EMC occurs in the older age group, there is a female predilection and mainly involves the parotid gland. Most authors recommend superficial parotidectomy as a treatment for low-grade malignant tumor in the superficial lobe of parotid gland. The treatment of epithelial-myoepithelial tumors typically includes surgical excision aimed at achieving a R0 resection. This paper reports a case of EMC of the parotid gland treated only by a conservational surgical excision. The lesion was exposed by the retromandibular approach and detached. After the parotid gland envelop was exposed, the mass was observed and was easy to remove due to capsulation. The preoperative diagnosis was a pleomorphic adenoma on the left parotid gland. The tumor was removed surgically with a conservative extracapsular dissection. The postoperative diagnosis was EMC, so superficial parotidectomy or radiation therapy was considered.
Nevertheless, the patient was observed and no additional treatment was attempted because the patient was old and a successfully excision of the tumor had been achieved.
Key words: Epithelial-myoepithelial carcinoma, Parotid gland
[paper submitted 2011. 6. 2 / revised 2011. 8. 30 / accepted 2011. 10. 12]
피암종은선암종중하나의독립된종양으로분류되었고 악성도가낮은매우드문타액선의신생물로정의되었다1
.
상피
-
근상피암종을다룬거의대부분의증례에서그것 의병적인특징에초점을맞추고있다.
상피-
근상피암종에 대한진단정보를얻기위한전산화단층촬영술(computed tomography, CT)
나 자기공명영상(magnetic resonance imaging, MRI),
양전자방출단층촬영술(positron emission
tomography, PET)
의영상적특성은 아직확립되지않았으며따라서술전의방사선사진만으로는진단에한계가있 다6
.
상피
-
근상피암종의일반적인치료는잔류암이남아있지 않도록외과적으로절제하는것이다7.
이번증례는 다형선종으로오인된 이하선에발생한상 피
-
근상피암종을이하선의실질조직을보존하면서종양만 제거한증례이다.
II. 증례보고
76
세여환이좌측하악 우각부의종창을주소로동아대학병원구강외과에내원하였다
.
약2
년전부터좌측볼주 위에 덩어리가만져졌으나별다른증상이없어 특별한검I. 서 론
상피
-
근상피암종은모든타액선종양의1-5%
를차지하는매우드문종양으로
80%
가이하선에발생한다1.
상피-
근상피암종은대부분
60-70
대노년층에서발생하며주로여성에서호발한다1
.
상피-
근상피암종은동통성또는무증상 으로장기간에걸쳐서서히성장하고,
분엽화되고잘경계 된단단하고견고한하나의덩어리이며직경은2-8 cm
정 도이다2.
상피
-
근상피 암종은 조직학적으로clear cell
이 포함되 어처음에는clear cell adenoma
나adenomyoepithelioma
로 간주되었다3,4.
그러나1972
년Donath
등5이종양의근상피 세포를발견하고상피-
근상피암종으로처음명명하였다. 1991
년World Health Organization (WHO)
에서상피-
근상 김 복 주602-103 부산시 서구 동대신동 3가 1번지 동아대학교 의료원 치과 구강악안면외과 Bok-Joo Kim
Department of Oral and Maxillofacial Surgery, Department of Dentistry, Dong-A University Medical Center
Dongdaeshin-dong 3-1, Seo-gu, Busan 602-103, Korea TEL: +82-51-240-5470 FAX: +82-51-241-5475 E-mail: [email protected]
사를하지않은채로지내다가점점크기가커져안모에영 향을 미칠만큼크기가커지고주변으로퍼져나가는느낌 이들어검사및치료를위해내원하였다
.
환자는당뇨로약 물복용중이었으며다른전신질환은없었다.
가족력은특 이사항이없었다.
병소는좌측하악우각부위의피부하방 에임상적으로크기3-4 cm
정도의유동성과경결감이있 는 덩어리이며림프절의종창이나 안면신경 손상의징후는나타나지않았다
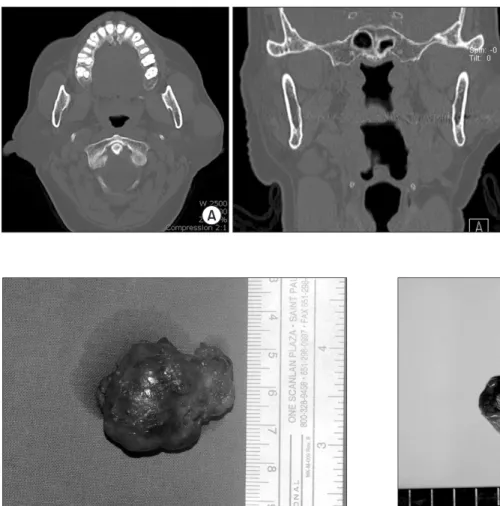
.(Fig. 1) CT
상병소는피부와이하선의천엽사이에위치하였고경계가 명확하였으며이하선실 질조직보다는 밀도가높으나비교적 균일한밀도를보였 다
.(Fig. 2)
술 전임상적
,
방사선학적으로 이하선의다형선종으로 가진단하였다.
병소는후하악접근법으로피부절개후조직 을 박리하여이하선피막을노출시켰다.
피막화된종양을 쉽게발견하였으며이하선천엽의실질조직을조심스럽게 둔박리하여피막을 손상시키지않고종양내부내용물의 누출없이종양을적출하였다.
종양은하나의덩어리로주 변조직과쉽게분리되었으며환자나이를고려하여이하선 Fig. 1. Facial view illustrating the 3-4 cm swelling on patient's leftcheek.
Sun-Mi Jin et al: Epithelial-myoepithelial carcinoma on the superficial lobe of the parotid gland: a case report. J Korean Assoc Oral Maxillofac Surg 2011
Fig. 2. Computed tomography (CT) scan. A. Transverse view of CT scan.
B. Coronal view of CT scan.
Sun-Mi Jin et al: Epithelial-myoepithelial carcinoma on the superficial lobe of the parotid gland: a case report. J Korean Assoc Oral Maxillofac Surg 2011
Fig. 3. Macroscopic view (external) shows well-circumscribed, thinly encapsulated mass with soft consistency.
Sun-Mi Jin et al: Epithelial-myoepithelial carcinoma on the superficial lobe of the parotid gland: a case report. J Korean Assoc Oral Maxillofac Surg 2011
Fig. 4. Macroscopic view (cross section) shows a relatively well defined grayish white soft tissue mass with focal cystic change on sectioning. The tumor is confined to the gland.
Sun-Mi Jin et al: Epithelial-myoepithelial carcinoma on the superficial lobe of the parotid gland: a case report. J Korean Assoc Oral Maxillofac Surg 2011
종양은두층의세포로구성된관상조직과투명세포로구 성된판상의조직소견이관찰되었고
(Fig. 5), H-E 40
배율조 직사진에서는종양의낭성변화와유두상조직이관찰되었 다.(Fig. 6)
또한
p63
면역조직화학검사에서관상조직의 바깥층이근상피세포라는것이확인되었다
.(Fig. 7)
III. 고 찰
타액선 종양은두경부 종양 중 약
3%
를 차지하고,
이중
75-88%
가 이하선에서발생한다8.
타액선의 종양은조직학적으로다양하지만흔한이하선종양은
pleomorphic adenomas, myoepitheliomas, basal cell adenomas, oncocy- tomas,
그리고Wharthin tumors
이다.
악성종양은18
가지 암종으로 분류되는데(WHO Classification, 2005) muco- epidermoid carcinoma
와acinic cell carcinoma
가가장흔하 고,
상피-
근상피암종은매우드물다.
타액선종양은전형적으로무통성으로느리게성장하며 크기가어느정도커진뒤에야임상적으로발견하게된다
.
타액선종양의진단방법으로는병력조사와촉진등의임상 검사외에 흡인생검법,
초음파검사, CT, MRI
등이있으며 이중흡인생검법은정확도가74-88%
정도에불과하여정 확한진단이어렵지만악성종양이의심되는환자에서유용 하다9.
타액선종양은방사선영상만으로는양성인지또는악성 인지감별하는것은제한이있다
.
양성종양으로감별하는 주요한형태학적특성은피막화되어있고,
초음파와MRI
상 에서균일한양상을보이고,
국소림프절병소가없는것이다10.
천엽은제거하지않았다.
층별로봉합시행후압박드레싱을시행하였다
.
수술후 평가에서감각이상이나운동이상 은나타나지않았다.
제거된종양은직경이
3-4 cm
로나타났으며경계가명확하고얇은피막으로둘러싸여있었다
.(Figs. 3, 4)
조직은
haematoxilin-eosin (H&E)
으로염색후40
배율및100
배율로각각관찰하였다. H&E 100
배율 조직사진에서Fig. 5. Microscopic view (H&E staining, ×100). The parotid gland mass is composed of double layered tubules and solid area of clear cells (short arrows). The tubules are lined by inner cuboidal cells with eosinophilic cytoplasm and outer layer of clear, myoepithelial type cells (long arrow).
Sun-Mi Jin et al: Epithelial-myoepithelial carcinoma on the superficial lobe of the parotid gland: a case report. J Korean Assoc Oral Maxillofac Surg 2011
Fig. 6. Microscopic view (H&E staining, ×40). The tumor also shows cystic area with papillary fronds (arrows).
Sun-Mi Jin et al: Epithelial-myoepithelial carcinoma on the superficial lobe of the parotid gland: a case report. J Korean Assoc Oral Maxillofac Surg 2011
Fig. 7. The immunohistochemical stain confirms the outer layer of tubules are lined by p63 positive myoepithelial cells (arrows) (anti-p63 immunohistochemistry, ×100).
Sun-Mi Jin et al: Epithelial-myoepithelial carcinoma on the superficial lobe of the parotid gland: a case report. J Korean Assoc Oral Maxillofac Surg 2011
에 국한되고안면신경과연관되지 않은저등급의 암종인 경우 보존적이하선절제술을시행한후에방사선치료를 병행하는것이합병증을최소화하고
,
재발률을줄일수있 는치료방법이라고추천하였다.
그러나이하선의종양에대한치료방법에는아직명확한 지침이없으며종양의형태나악성도에따라 다양한것으 로알려져있다
.
이번증례에서는조직검사에서종양세포 가피막내부로국한되어있으며,
수술시종양이한덩어리 로잘제거되었고,
환자의전신상태와고령임을고려하여 추가적인수술이나치료는시행하지않고경과관찰하기로 하였다.
또한상피
-
근상피 암종의경우일반적으로 외과적으로R0 margin
으로절제하는것이일반적인치료법이며7,
이번증례에서는피막화된종양외부로종양세포가누출되지않 은점을고려하면
,
안면신경손상등의합병증을유발할수 있는이하선의천엽절제술을추가적으로시행하지않는것 이가장보존적인치료방법이라판단되었다.
수술전임상검사및방사선검사로다형선종등의양성 종양으로가진단하여종양의외과적절제술만시행한뒤
,
조직검사를통해악성종양인상피-
근상피암종으로 최종 진단한이번증례를통해이하선종양의수술전세침흡인 생검(fine needle aspiration biopsy)
등의다양한진단방법을 이용하여신중하게가진단하는것이중요하며,
수술시에 는피막화된종양의세포가주위 조직으로누출되지않도 록세심한절제가필요하다고생각된다.
이번증례는악성종양으로진단후에도추가적으로이하 선천엽절제술이나방사선치료를시행하지않고보존적으 로치료를마친경우로
, 5
개월이지난 현재까지별다른합 병증과재발의징후는보이지않고있다.
References
1. Seifert G, Sobin LH. Epithelial-myoepithelial carcinoma. In:
WHO. World Health Organization International Classification of Tumors: Histological Typing of Salivary Gland Tumors. 2nd ed.
Berlin: Spring-Verlag; 1991:23-4.
2. Dorothy MP. Surgical Pathology and Fine Needle Aspiration Cytopathology. In: John EN, Mark MG, eds. Color Atlas and Text of the Salivary Glands. 1st ed. Barcelona: Mosby-Wolfe; 1995:78.
3. Suksela E, Tarkkanen J, Wartiovaara J. Parotid clear cell adenoma of possible myoepithelial origin. Cancer 1972;30:742-8.
4. Bauer WH, Fox RA. Adenomyoepithelioma (Cylindroma) of palatal mucous glands. Arch Pathol 1945;39:96-102.
5. Donath K, Seifert G, Schmitz R. Diagnosis and ultrastructure of the tubular carcinoma of salivary gland ducts. Epithelial-myoepithelial carcinoma of the intercalated ducts. Virchows Arch 1972;356:16- 31.
6. Yamada H, Kawaguchi K, Yagi M, Morita Y, Mishima K, Uno K, et al. Epithelial-myoepithelial carcinoma of the submandibular gland with a high uptake of 18F-FDG: a case report and image diagnosis. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2007;104:243-8.
7. Kokemueller H, Swennen G, Brueggemann N, Brachvogel P, 석회화되어있는것도양성종양의또다른특성이다10
.
악성종양의양상은일정하지않은데많은 악성타액선종양이 위막을가지고
,
불규칙한형태와주변으로침투하는경향이있다10
.
그러나low-grade
의악성종양의경우 때때로술전에양성종양으로오진되어부적절한수술기법이이용될 수있고결과적으로국소적인재발이나나쁜예후를가져 올수있다1
.
CT
는특히종양의진단에효과적이며내인성과외인성 종양의감별 및인접조직으로의침투 양상을평가하는데 매우유용하다10.
타액선의양성종양은대개병소의경계 가명확하고정상타액선조직보다밀도가높게나타나며 일반적으로균일한밀도를보이는데악성도가낮은악성종 양도동일한소견을보일수있다10.
반면에 악성도가높은 악성종양이나재발한악성종양은정상타액선조직보다밀 도가높게 나타나지만대개 병소의경계가불명확하며병 소의밀도도균일하지않다10.
그러나이러한감별지침은예외적인경우가많기때문 에방사선적형태만보고타액선종양을감별하는것은매 우제한적이다
.
따라서타액선종양의진단에는조직생검 이절대적이라고할수있다.
상피
-
근상피암종의 조직 발생은 타액선의 개재도관 에서유래된다11.
조직학적으로 전형적인상피-
근상피암 종은inner ductal cells
의double-cell lining
과outer clear myoepithelial cells
이다12.
면역조직학적으로는 정상적인 개재도관과 증식된개재도관의clear myoepithelial cell
이smooth muscle specific actin
과S-100 protein,
그리고cytokeratin
에면역반응성을나타낸다13.
이번증례에서는수술전임상적으로나방사선학적으로 다형선종을가장우선으로가진단하였고수술도양성종양 에준하여가장보존적인방법으로
extracapsular dissection
을이용하여피막화된종양만제거하고이하선천엽 절제 술을시행하지않았다.
그러나조직생검을통하여상피-
근 상피암종으로최종진단되었다.
Deere
등14은타액선에발생한상피-
근상피암종의국소재발률이
42%
이고다른부위로의전이도10%
관찰된다고하였다
.
이하선종양이재발하는원인은종양의제거과정중피 막이파괴되어종양세포가인접조직으로 파급되는경우
,
이하선심층엽에발생한종양이후하악부위까지확산되어 있는경우,
외과적적출술이부적절한경우등이있다9,15.
상피
-
근상피암종은상대적으로 악성도가낮고,
분화도 가높아저등급의악성종양으로분류되며예후가좋다.
악성도가낮고크기가
4 cm
이하이며종양이이하선천엽에위치하는것을 고려하였을때
, Harish
에의해추천되는치 료는이하선천엽의절제술이다16.
추가적인방사선치료나 항암화학요법은필요하지않다16.
2005
년Lim
등17의연구에서는이하선의암종이천층엽Neck 1995;17:437-44.
13. Di Palna S. Epithelial/myoepithelial carcinoma with co-existing multifocal intercalated duct hyperplasia of the parotid gland.
Histopathology 1994;25:494-6.
14. Deere H, Hore I, McDermott N, Levine T. Epithelial-myoepithelial carcinoma of the parotid gland: a case report and review of the cytological and histological features. J Laryngol Otol 2001;115:434-6.
15. Spiro RH, Huvos AG, Strong EW. Cancer of the parotid gland.
A clinicopathologic study of 288 primary cases. Am J Surg 1975;130:452-9.
16. Harish K. Management of primary malignant epithelial parotid tumors. Surgical Oncol 2004;13:7-16.
17. Lim YC, Lee SY, Kim KB, Lee JS, Koo BS, Shin HA, et al.
Conservative parotidectomy for the treatment of parotid cancers.
Oral Oncol 2005;41:1021-7.
Eckardt A, Hausamen JE. Epithelial malignancies of the salivary glands: clinical experience of a single institution-a review. Int J Oral Maxillofac Surg 2004;33:423-32.
8. Baek S, Ha JW, Oh HK, Ryu SY, Kim WJ. A clinical study on the parotid gland tumors. J Korean Assoc Maxillofac Plastic Reconstructive Surg 2002;24:398-405.
9. Woods JE, Chong GC, Beahrs OH. Experience with 1,360 primary parotid tumors. Am J Surg 1975;130:460-2.
10. Park TW, Lee SL, Kim JD, Park CS, Choi SC, Ko KJ, et al. Oral and Maxillofacial Radiology. 3rd ed. Seoul: Narae Publishing;
2001:476-7.
11. Colio RL, Sciubba JJ, Brannon RB, Batsakis JG. Epithelial/myo- epithelial carcinoma of intercalated duct origin. A clinicopathologic and ultrastructural assessment of sixteen cases. Oral Surg Oral Med Oral Pathol 1982;53:280-7.
12. Cheung FM, Hioe F, Kong JH. Histologic variant of the epithelial/
myoepithelial carcinoma of the salivary gland: a case report. Head