ARTICLE
Int J Thyroidol 2016 November 9(2): 159-167 https://doi.org/10.11106/ijt.2016.9.2.159Received July 8, 2016 / Revised October 12, 2016 / Accepted October 15, 2016
Correspondence: Jaetae Lee, MD, PhD, Department of Nuclear Medicine, Kyungpook National University Hospital, Kyungpook National University School of Medicine, 130 Dongdeok-ro, Jung-gu, Daegu 41944, Korea
Tel: 82-53-420-5586, Fax: 82-53-200-3419, E-mail: [email protected]
Copyright ⓒ 2016, the Korean Thyroid Association. All rights reserved.
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creative- commons.org/licenses/by-nc/4.0/), which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Pathological N1b Node Metastasis Itself Can Be Still a Valid Prognostic Factor in PTC after High Dose RAI Therapy
Choon-Young Kim
1, Seung Hyun Son
1, Ji-hoon Jung
1, Chang-Hee Lee
1, Ju Hye Jeong
1, Shin Young Jeong
1, Sang-Woo Lee
1, Byeong-Cheol Ahn
1and Jaetae Lee
1,2Department of Nuclear Medicine, Kyungpook National University Hospital, Kyungpook National University School of Medicine1, and the Daegu-Gyeongbuk Medical Innovation Foundation2, Daegu, Korea
Background and Objectives: The aim of this study was to determine whether pathologically proven central or lateral lymph node (LN) metastasis (pN1a or pN1b) could affect ablation success and recurrence after high-dose radioactive iodine (RAI) ablation. We also sought to identify the risk factors for long-term recurrence in patients with papillary thyroid carcinoma (PTC). Materials and Methods: A total of 277 patients with pN1 disease who had undergone high-dose RAI ablation (5.55 GBq) between 2000 and 2006 were included in this retrospective study. We compared the ablation success rate and the recurrence rate between patients with pN1a and pN1b disease. Univariate and multivariate analyses were performed to identify the risk factors for recurrence. Results: The median duration of follow-up was 10.2 years. The overall ablation success rate was 64%, and the ablation success rate in the pN1b group (49%) was lower than in the pN1a group (74%). The overall recurrence rate was 23%, and the recurrence rate in the pN1b group (30%) was higher than in pN1a group (18%). A higher ratio of metastatic LNs, a higher level of pre-ablation thyroglobulin, and ablation failure were significant risk factors for recurrence by multivariate analysis. Conclusion: Patients with pN1b disease experienced a lower ablation success rate and a higher recurrence rate than patients with pN1a disease.
However, a higher ratio of metastatic LNs, a higher level of pre-ablation thyroglobulin, and ablation failure were stronger risk factors than the pathological N stage for long term recurrence in patients with node-positive PTC.
Key Words: Papillary thyroid carcinoma, Ablation success, Recurrence, Radioactive iodine ablation
Introduction
Papillary thyroid carcinoma (PTC) is the most com- mon type of thyroid carcinoma. Lymph node (LN) metastasis is frequently found in up to 70% of patients, and recurrence may occur in more than 30% of cas- es, although the disease-related mortality for PTC is not high.1) Previous studies have identified several risk
factors for recurrence in patients with PTC.1,2) However, the impact of the location of metastatic LNs on mortality and recurrence is controversial. A complicating factor is the difficulty encountered by surgeons and patholo- gists when trying to precisely locate metastatic LNs during surgery or in surgical specimens. The American Joint Committee on Cancer (AJCC) has subdivided patients with positive neck nodes into N1a and N1b groups. N1b status is associated with a worse re-
currence-free survival (RFS).3) However, the American Thyroid Association (ATA) guidelines classify patients with neck LN metastasis as an intermediate-risk group, regardless of the location of the metastatic LNs.4)
As suggested by the recent ATA guideline, the risk of recurrence can vary depending on the specific characteristics of the metastatic LNs, such as size, number, and extranodal extension, in patients with neck node-positive PTC.5,6) Compared with previous recommendations, recent ATA guidelines have tended to not to consider the presence of regional neck node metastasis to be an indicator of a worse prognosis.4)
Since Mazzaferri7) reported that RAI ablation was effective in reducing recurrence in patients with PTC, radioactive iodine (RAI) therapy after surgery has been a standard procedure for the ablation of remnant thy- roid tissue and for the treatment of iodine-avid meta- stasis for over 50 years. Prior to the 2009 ATA guide- lines, a dose of 5.55 GBq I-131 was commonly ap- plied to patients with neck node metastasis, regardless of the location of the involved lymph nodes.4) Although recent papers have suggested using a lower activity I-131 for remnant ablation or adjuvant therapy after total thyroidectomy, controversy still exists regarding the optimal strategy of RAI therapy according to the status of metastatic LNs in patients with node-positive PTC.8-11)
Given the controversy surrounding the impact of LN metastasis on the outcome of patients with PTC, the aim of this study was to determine whether different locations of metastatic LNs had an impact on the suc- cess of ablation therapy or the rate of recurrence.
Additionally, we attempted to identify the risk factors for long-term recurrence in patients with PTC and patho- logically-proven neck node metastasis.
Materials and Methods
Patients
A total of 277 consecutive patients with PTC who had pathologically proven central or lateral LN meta- stasis and who underwent RAI ablation between 2000 and 2006 were retrospectively reviewed for this study.
Pathological staging was determined according to the Seventh Edition of the AJCC.3) Surgery was performed by two experienced thyroid surgeons who perform more than 300 cases of thyroid cancer surgery per year. Most patients were diagnosed with PTC by pre- operative ultrasonography (US) guided fine-needle aspiration cytology. All patients underwent total thyroi- dectomy, and prophylactic central node dissection (CND) was performed in patients who were not sus- pected of having LN metastasis. In patients who had LN metastasis, therapeutic central and/or lateral neck node dissections were performed according to the extent of the lymph node metastasis. The diagnosis of PTC was reconfirmed for all patients by surgical pathology.
All patients underwent high-dose RAI ablation after surgery, because of regional neck node involvement of the PTC. The exclusion criteria were as follows: 1) pathological N0 or Nx disease; 2) less than 3 dis- sected LNs, suggesting incomplete dissection; 3) known distant metastasis before RAI ablation; 4) pos- itive interfering anti-thyroglobulin antibodies; 5) in- sufficient patient data; and 6) loss to follow-up before the evaluation for ablation success. Clinical and pathological parameters were reviewed and retrieved, including sex, age, tumor size, extrathyroidal extension (ETE), TNM and AJCC stage, the number and ratio of metastatic LNs, pre-ablation TSH-stimulated thyro- globulin (s-Tg) levels, and the result of a post-therapy I-131 whole body scan (WBS). Data collection and analysis were approved by our Institutional Review Board, and the requirement for written informed con- sent was waived.
Radioactive Iodine Ablation Protocol
All patients underwent total thyroidectomy with cen- tral and/or lateral neck dissection for PTC followed by RAI ablation therapy. To induce a hypothyroid state, levothyroxine (T4) was discontinued for at least 4 weeks with triiodothyronine (T3) replacement for the first 2 weeks. A low-iodine diet was also prescribed for all patients at least 2 weeks before RAI ablation.
After achievement of an endogenous elevation of TSH (>30 μIU/mL), all patients were administered 5.55
GBq of I-131 according to a fixed dosage protocol that has been commonly used for several decades.
A post-therapy I-131 WBS was acquired 4 to 7 days after the administration of I-131 using a dual-head gamma camera (Prism 2000; Picker International, Cleveland, OH, USA; Infinia II, GE Healthcare, Milwaukee, WI, USA). Additional delayed images were obtained if clinically needed. SPECT imaging of the neck was not performed during this study.
Evaluation for Successful Ablation
Follow-up evaluations for successful ablation were performed during the first 6-12 months after RAI ablation. Patients underwent a physical examination, measurement of s-Tg levels, and imaging studies, in- cluding neck US, a diagnostic WBS, and/or 18-flu- oro-2-deoxyglucose positron emission tomog- raphy/computed tomography (F-18 FDG PET/CT).
The neck US was performed by an experienced radi- ologist, and fine-needle aspiration cytology was per- formed for suspicious regional LNs greater than 5-8 mm in the smallest diameter according to the ATA guidelines.4) For a diagnostic WBS and TSH stim- ulation, the same protocol for RAI ablation was applied.
The diagnostic WBS was performed 1 day after I-123 (18.5 MBq) or 2 days after I-131 (11.1 MBq) ad- ministration.
Based on the results of these evaluations, success- ful ablation was defined as a s-Tg level less than 2 ng/mL, negative or only negligible faint bed uptake on diagnostic WBS, and a negative neck US.10,12) Disease recurrence was defined if LN metastasis or recurrent disease was proven histologically or if newly identified distant metastasis were evident on imaging studies, along with an elevated s-Tg level of more than 2 ng/mL.
Clinical Endpoints and Follow-Up
To evaluate the prognostic value of clinical and pathologic parameters, recurrence was chosen as an endpoint. RFS was calculated from the date of RAI ablation to the date of recurrence or the last follow-up.
Statistical Analysis
Statistical analysis was performed using MedCalc for Windows, version 13.3.0.0 (MedCalc Software, Maria- kerke, Belgium). All patients were divided into 2 groups, the pN1a group and the pN1b group.
Comparison of categorical variables between the two groups was performed with a chi-square test, and continuous variables were compared by Student t-test. The Kaplan-Meier method and the log-rank test were used in the survival analysis for RFS be- tween the two groups. The Cox proportional hazards model with forward method was used to assess the potential independent effects of clinicopathologic pa- rameters for RFS. A p value <0.05 was considered to be statistically significant.
Results
Clinical and Pathologic Characteristics
The clinical and pathologic characteristics of 277 patients with PTC are shown in Table 1. The median duration of follow-up was 10.2 years (range, 0.8- 15.2 years). Among the 277 patients, 167 (60%) pa- tients were classified as the pN1a group, and 110 (40%) patients were classified as the pN1b group. Age was not significantly different between the two groups.
The mean number of dissected LNs was 15±13.
More LNs were dissected (27±14 vs. 7±4, p<
0.001) and a higher number of metastatic LNs were identified (8±6 vs. 3±2, p<0.001) in the pN1b group than in the pN1a group. The ratio of metastasis per dissected LN was higher in the pN1a group. The proportion of male patients and the pre-ablation s-Tg levels were higher in the pN1b group. The proportion of patients who showed I-131 uptake outside of the thyroid bed (LN or distant organ) on post-therapy I-131 WBS was also higher in pN1b group.
Ablation Success Rate and Recurrence Rate
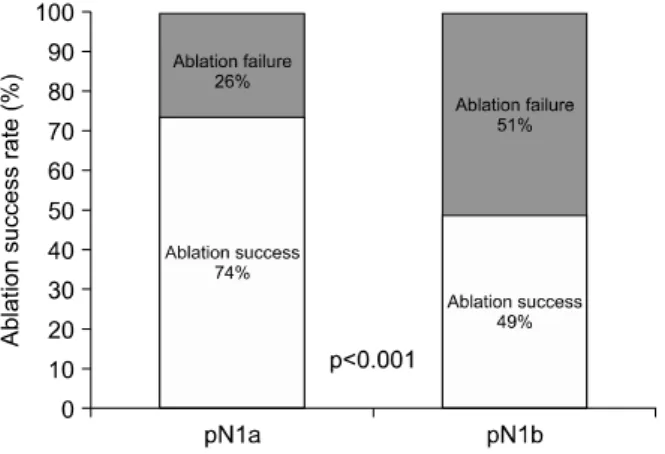
The overall ablation success rate was 64% (n=
177/277) and was higher in the pN1a group than in the pN1b group (74% vs. 49% p<0.001, Fig. 1). The
Table 1. Patient characteristics
Characteristics All patients (n=277)
pN1a (n=167)
pN1b
(n=110) p value
Sex
Female 239 (86%) 153 (92%) 86 (78%) 0.003
Male 38 (14%) 14 (8%) 24 (22%)
Age (year)
<45 158 (57%) 101 (61%) 57 (52%) 0.193
≥45 119 (43%) 66 (39%) 53 (48%)
Tumor size (cm)
Mean±SD 2.2±1.3 2.3±1.3 2.0±1.3 0.139
Median (range) 2.0 (0.1-7.0) 2.0 (0.2-7.0) 1.8 (0.1-6.0)
ETE
Intrathyroidal 80 (29%) 54 (33%) 26 (24%) 0.119
Microscopic ETE 83 (30%) 49 (29%) 34 (31%)
Macroscopic ETE 114 (41%) 64 (38%) 50 (45%)
Pathological T stage
T1 56 (20%) 34 (20%) 22 (20%) 0.184
T2 21 (8%) 18 (11%) 3 (3%)
T3 154 (55%) 92 (55%) 62 (56%)
T4 46 (17%) 23 (14%) 23 (21%)
Number of dissected LNs
Mean±SD 15±13 7±4 27±14 <0.001
Median (range) 9 (3-76) 6 (3-22) 27 (3-76)
Number of metastatic LNs
Mean±SD 5±5 3±2 8±6 <0.001
Median (range) 4 (1-30) 3 (1-12) 7 (1-30)
Ratio of metastatic LNs
Mean±SD 0.4±0.3 0.5±0.3 0.3±0.2 <0.001
Median (range) 0.3 (0.02-1.0) 0.4 (0.06-1.0) 0.3 (0.02-1.0) Pre-ablation s-Tg (ng/mL)
Mean±SD 26.4±65.6 19.6±58.3 36.8±74.5 0.043
Median (range) 5.4 (0.1-470.0) 3.4 (0.1-470.0) 8.6 (0.1-433.9) Post-therapy I-131 WBS
Thyroid bed 219 (79%) 140 (83%) 79 (72%) 0.011
LN metastasis 54 (20%) 26 (16%) 28 (25%)
Distant metastasis 4 (1%) 1 (1%) 3 (3%)
ETE: extrathyroidal extension, LN: lymph node, s-Tg: TSH-stimulated thyroglobulin, SD: standard deviation, WBS: whole body scan
Fig. 1. Comparison of ablation success rate between patients with papillary thyroid carcinoma who had pathological N1a and N1b disease.
mean cumulative number of RAI therapy was 1.5±
0.8, and the mean cumulative dose of I-131 was 8.6±5.3 GBq. The mean cumulative number of RAI therapy was higher in the pN1b than in the pN1a group (1.7 vs. 1.4, p=0.007).
There were 63 subjects who developed recurrence during the follow-up period. The overall recurrence rate was 22.7%. The most common recurrence site was the lateral neck LN (51/63, 81%), followed by the central neck LN (6/63, 10%), distant organs (lung and/or bone, 4/63, 6%) and the thyroid bed (2/63, 3%). The patients were classified by the sites of re-
Fig. 2. Comparison of recurrence rate between patients with papillary thyroid carcinoma who had pathological N1a and N1b disease.
Fig. 3. Kaplan-Meier survival analysis according to patholo- gical N1a and N1b disease in patients with papillary thyroid carcinoma.
currence, such as local (thyroid bed), regional (central or lateral neck LN), and distant metastasis. There was no significant difference in recurrence site between the pN1a group and pN1b group (p=0.645).
The recurrence rate in the pN1b group (30%, 33/110) was much higher than that in the pN1a group (18%, 30/167, p=0.028, Fig. 2). The time to re- currence was longer in the pN1a group than that in the pN1b group (mean 33.7 months vs. 26.7 months), although there was no statistically significant difference (p=0.357). Accordingly, the RFS was shorter in the pN1b group than in the pN1a group (mean 129 months vs. 153 months, p=0.013, Fig. 3). Thyroid cancer-related death was observed in 2 patients (1.2%) in the pN1a group and 5 patients (4.5%) in the pN1b group (p=0.178).
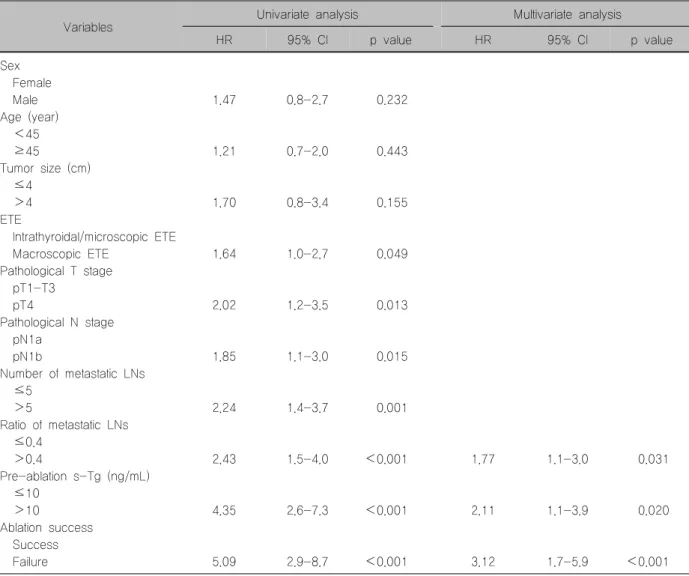
Univariate and Multivariate Analyses for Recur- rence-Free Survival
Univariate and multivariate analyses for RFS were performed using various clinical and pathologic pa- rameters (Table 2). In univariate analysis, a higher pathological N stage (pN1b, hazard ratio [HR]=1.85;
95% confidence interval [CI]=1.1-3.0; p=0.015) and ablation failure (HR=5.09; 95% CI=2.9-8.7; p<
0.001) were significant risk factors for recurrence.
Moreover, macroscopic ETE (HR=1.64; 95% CI=
1.0-2.7; p=0.049), a higher pathological T stage (T4 stage; HR=2.02; 95% CI=1.2-3.5; p=0.013), a high- er number of metastatic LNs (>5; HR=2.24; 95%
CI=1.4-3.7; p=0.001), a higher ratio of metastatic LNs (>0.4; HR=2.43; 95% CI=1.5-4.0; p<0.001), and a higher level of pre-ablation s-Tg (>10 ng/mL;
HR=4.35; 95% CI=2.6-7.3; p<0.001) were also sig- nificant risk factors for recurrence in patients with node-positive PTC.
In multivariate analysis, a higher ratio of metastatic LNs (>0.4; HR=1.77; 95% CI=1.1-3.0; p=0.031), a higher level of pre-ablation s-Tg levels (>10 ng/mL;
HR=2.11; 95% CI=1.1-3.9; p=0.020), and ablation failure (HR=3.12; 95% CI=1.7-5.9, p<0.001) were significant risk factors for recurrence in patients with node-positive PTC. A higher pathological N stage was a significant risk factor in univariate analysis, but not in multivariate analysis.
Discussion
In our series of 277 subjects who underwent sur- gery followed by RAI ablation using high dose (5.55 GBq) I-131, successful ablation and long-term re- currence of PTC varied depending on the location of metastatic LNs in the neck. There have been numer- ous controversies regarding dosage options of I-131 for post-surgical RAI ablation or therapy for differ- entiated thyroid cancer patients with neck node metastasis. In line with ATA guidelines but contrary to
Table 2. Univariate and multivariate analyses of clinicopathologic variables for recurrence-free survival in patients with node-positive papillary thyroid carcinoma
Variables Univariate analysis Multivariate analysis
HR 95% CI p value HR 95% CI p value
Sex Female
Male 1.47 0.8-2.7 0.232
Age (year) <45
≥45 1.21 0.7-2.0 0.443
Tumor size (cm) ≤4
>4 1.70 0.8-3.4 0.155
ETE
Intrathyroidal/microscopic ETE
Macroscopic ETE 1.64 1.0-2.7 0.049
Pathological T stage pT1-T3
pT4 2.02 1.2-3.5 0.013
Pathological N stage pN1a
pN1b 1.85 1.1-3.0 0.015
Number of metastatic LNs ≤5
>5 2.24 1.4-3.7 0.001
Ratio of metastatic LNs ≤0.4
>0.4 2.43 1.5-4.0 <0.001 1.77 1.1-3.0 0.031
Pre-ablation s-Tg (ng/mL) ≤10
>10 4.35 2.6-7.3 <0.001 2.11 1.1-3.9 0.020
Ablation success Success
Failure 5.09 2.9-8.7 <0.001 3.12 1.7-5.9 <0.001
CI: confidence interval, ETE: extrathyroidal extension, HR: hazard ratio, LN: lymph node, s-Tg: TSH-stimulated thyroglobulin
the results from other studies, a recent publication suggested using a lower dosage of I-131.5) Castagna et al.8) recently reported that low (1.11-1.85 GBq) and high (≥3.7 GBq) RAI activity resulted in similar out- comes for patients with PTC who were considered to have an intermediate risk of recurrence, even those with neck LN metastasis. The authors suggested that both low- and intermediate-risk patients could be safely ablated using low RAI activity. However, de Meer et al.9) reported that the presence of lateral metastatic LNs was correlated with a higher re- currence rate and lower disease-free survival than central metastatic LNs. Some other studies have also reported that PTC patients with pN1b disease had
poorer RFS than pN0/Nx and pN1a patients.13,14) In the current study, recurrence occurred in a significant proportion of patients, including 30% in the pN1b group (30%) and 18% in the pN1a group (18%), al- though they received high-dose (5.55 GBq) RAI therapy. Furthermore, the ablation success rate was lower and the cumulative number of RAI therapy and recurrence rates were higher in patients with pN1b than in those with pN1a disease. Therefore, applica- tion of lower dose such as 1.1 GBq I-131 in patients with N1b does not seem to be reasonable approach.
In the current study, patients who were administered only 5.55 GBq of I-131 regardless of their pN1a or pN1b disease status were enrolled to eliminate I-131
dose as a confounding factor. Although there has been a recent trend toward using a lower dose of I-131 to minimize the adverse effects of RAI ther- apy,10,11) before 2000, a typical RAI dose recom- mendation was 3.7 GBq for remnant ablation, 5.55 GBq for neck LN metastasis regardless of location of the metastatic LNs,15) and 6.475-7.4 GBq for distant metastasis.
Although, confirmation is required from larger com- parative and prospective studies to evaluate the im- pact of lower-dose I-131 on outcomes in patients with pN1b PTC, our results suggest that more ag- gressive therapy with higher doses of RAI ablation may be needed in patients with pN1b disease.
According to the AJCC staging system,3) age is an important factor in PTC staging. Younger node-pos- itive patients (age<45) are classified as having stage I disease, whereas older node-positive patients (age
≥45) are classified as either stage III or stage IV disease. Smith et al.2) reported that disease specific survival was worse for older patients with pN1b PTC.
Furthermore, the presence of node metastasis did not significantly affect survival for younger patients, re- gardless of the location. Sabra et al.11) reported that RAI ablation using more than 3.7 GBq of I-131 was unlikely to improve therapeutic response in younger patients with pN1b disease. In the current study, bina- ry classification by age (older than 45 years) was not a significant risk factor for recurrence in node-positive PTC patients. In a subgroup analysis, however, the lo- cation of metastatic LNs was a significant risk factor for recurrence in the older age group (p=0.044), but not in the younger age group (p=0.175).
The pathological N stage was a significant risk fac- tor for recurrence in univariate analysis, but not in multivariate analysis. Instead, a higher ratio of meta- static LNs and a higher level of pre-ablation s-Tg levels were stronger risk factors for recurrence in pa- tients with node-positive PTC. In the current study, the ratio of metastatic LNs was higher in the pN1a group than in the pN1b group. One possible reason for this finding may be that the number of dissected LNs and the proportion of negative LNs were higher in central and lateral neck dissections than in central neck dis-
section alone. Schneider et al.16) reported that a higher metastatic LN ratio and a metastatic central LN ratio were strongly associated with recurrence of PTC after initial surgery. Furtado Mde et al.17) reported that the overall rate of persistent disease or tumor recurrence after RAI ablation was only approximately 3%, even in patients with PTC who had clinically apparent LN metastasis, provided that they did not have poor prognostic factors, such as size, number, and extra- nodal extension of metastatic LNs. However, in our subjects, patients who had higher level of pre-ablation s-Tg had a significantly high frequency (28.5%) of persistent disease or tumor recurrence. Therefore, in addition to the AJCC staging system based on age and location of metastatic LNs, consideration should be given to incorporating more specific risk factors, such as the ratio of metastatic LNs and pre-ablation s-Tg levels. Although these factors are not integrated in the previous staging system, they are important for developing an optimal therapeutic strategy for patients with node-positive PTC.
The overall ablation success rate of 64% in the present study group was lower than those of recent randomized trials, where success rates ranged from 90-94%.10,18) Several factors affecting ablation suc- cess rates have been previously reported such as surgical completeness, the characteristics of the en- rolled patient population, the definition of ablation suc- cess and the differences in iodine diet conditions.
However, our differing results may also be due to the application of different criteria for remnant ablation success used in this study. One study evaluated the success of remnant ablation based on neck US and s-Tg levels or diagnostic WBS in patients with detect- able Tg-Ab.18) In the present study, successful abla- tion was defined as a s-Tg level less than 2 ng/mL, negative or only negligible faint bed uptake on diag- nostic WBS, and negative neck US at first evaluation, these more stringent criteria may explain the lower ablation success rate. Furthermore, this study was performed in a high-iodine intake area, and excessive dietary intake of iodine can also result in poor ablation outcomes. Sohn et al.19) reported that the ablation rate significantly decreased as the urinary iodine excretion
increased in patients with low-risk thyroid cancer treated with 1.1 GBq of I-131. Considering the higher amount of iodine intake in east Asia including Korea, iodine intake may not be as low as that reported in Western countries, although we recommend strict control of iodine intake. Indeed, Ha et al.20) reported ablation rates similar to our findings.
This study had several limitations. First, this was a retrospective study. Although, randomized and pro- spective studies are not easy to perform for relatively benign cancers such as differentiated thyroid cancer, large numbers of patients with long follow-up periods should be included for further clarification. Second, al- though Randolph et al.6) reported that the size of metastatic foci and extra-nodal extension of metastatic LNs can be excellent prognostic factor in PTC, we were unable to analyze these factors because the sizes of the metastatic lesions in dissected LNs were not recorded in our pathologic reports. Additionally, patients underwent central neck dissection according to the pre-surgical evaluation for neck node metastasis.
Thus, the results may differ from those of patients who underwent prophylactic central neck dissection.
In summary, our results suggest that more ag- gressive therapy, such as RAI ablation, using a higher dose of I-131 may be needed in PTC patients with pN1b disease than in those with pN1a disease.
Consideration should not only be given to the patho- logical N stage but also to the ratio of metastatic LNs and pre-ablation s-Tg levels when determining the optimal therapeutic strategy.
In conclusion, patients with pN1b PTC experienced a lower ablation success rate, a higher recurrence rate and shorter RFS than patients with pN1a PTC.
However, a higher ratio of metastatic LNs and a higher level of pre-ablation s-Tg were stronger risk factors than the pathological N stage for long-term re- currence in patients with node-positive PTC.
Acknowledgments
A grant of the Kyungpook National University Rese- arch Fund, 2012.
References
1) Leboulleux S, Rubino C, Baudin E, Caillou B, Hartl DM, Bidart JM, et al. Prognostic factors for persistent or recurrent disease of papillary thyroid carcinoma with neck lymph node metastases and/or tumor extension beyond the thyroid capsule at initial diagnosis. J Clin Endocrinol Metab 2005;90(10):5723-9.
2) Smith VA, Sessions RB, Lentsch EJ. Cervical lymph node metastasis and papillary thyroid carcinoma: does the com- partment involved affect survival? Experience from the SEER database. J Surg Oncol 2012;106(4):357-62.
3) The American Joint Committee on Cancer. Thyroid. In: Edge SB, Byrd DR, Compton CC, Fritz AG, Greene FL, Trotti A, editors. AJCC cancer staging manual. 7th ed. New York, NY:
Springer; 2010. p.87-96.
4) American Thyroid Association Guidelines Taskforce on Thyroid Nodules and Differentiated Thyroid Cancer, Cooper DS, Doherty GM, Haugen BR, Kloos RT, Lee SL, et al.
Revised American Thyroid Association management guidelines for patients with thyroid nodules and differentiated thyroid cancer. Thyroid 2009;19(11):1167-214.
5) Haugen BR, Alexander EK, Bible KC, Doherty GM, Mandel SJ, Nikiforov YE, et al. 2015 American Thyroid Association management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer: the American Thyroid Association Guidelines Task Force on thyroid nodules and differentiated thyroid cancer. Thyroid 2016;26(1):1-133.
6) Randolph GW, Duh QY, Heller KS, LiVolsi VA, Mandel SJ, Steward DL, et al. The prognostic significance of nodal metastases from papillary thyroid carcinoma can be stratified based on the size and number of metastatic lymph nodes, as well as the presence of extranodal extension. Thyroid 2012;22(11):
1144-52.
7) Mazzaferri EL. Thyroid remnant 131I ablation for papillary and follicular thyroid carcinoma. Thyroid 1997;7(2):265-71.
8) Castagna MG, Cevenini G, Theodoropoulou A, Maino F, Memmo S, Claudia C, et al. Post-surgical thyroid ablation with low or high radioiodine activities results in similar outcomes in intermediate risk differentiated thyroid cancer patients. Eur J Endocrinol 2013;169(1):23-9.
9) de Meer SG, Dauwan M, de Keizer B, Valk GD, Borel Rinkes IH, Vriens MR. Not the number but the location of lymph nodes matters for recurrence rate and disease-free survival in patients with differentiated thyroid cancer. World J Surg 2012;36(6):1262-7.
10) Mallick U, Harmer C, Yap B, Wadsley J, Clarke S, Moss L, et al. Ablation with low-dose radioiodine and thyrotropin alfa in thyroid cancer. N Engl J Med 2012;366(18):1674-85.
11) Sabra MM, Grewal RK, Ghossein RA, Tuttle RM. Higher administered activities of radioactive iodine are associated with less structural persistent response in older, but not younger, papillary thyroid cancer patients with lateral neck lymph node metastases. Thyroid 2014;24(7):1088-95.
12) Pacini F, Ladenson PW, Schlumberger M, Driedger A, Luster M, Kloos RT, et al. Radioiodine ablation of thyroid remnants after preparation with recombinant human thyrotropin in
differentiated thyroid carcinoma: results of an international, randomized, controlled study. J Clin Endocrinol Metab 2006;
91(3):926-32.
13) Jeon MJ, Kim TY, Kim WG, Han JM, Jang EK, Choi YM, et al. Differentiating the location of cervical lymph node metastasis is very useful for estimating the risk of distant metastases in papillary thyroid carcinoma. Clin Endocrinol (Oxf) 2014;81(4):593-9.
14) Nixon IJ, Wang LY, Palmer FL, Tuttle RM, Shaha AR, Shah JP, et al. The impact of nodal status on outcome in older patients with papillary thyroid cancer. Surgery 2014;156(1):137-46.
15) Beierwaltes WH, Rabbani R, Dmuchowski C, Lloyd RV, Eyre P, Mallette S. An analysis of "ablation of thyroid remnants" with I-131 in 511 patients from 1947-1984: experience at University of Michigan. J Nucl Med 1984;25(12):1287-93.
16) Schneider DF, Mazeh H, Chen H, Sippel RS. Lymph node ratio predicts recurrence in papillary thyroid cancer. Oncologist 2013;18(2):157-62.
17) Furtado Mde S, Rosario PW, Calsolari MR. Persistent and recurrent disease in patients with papillary thyroid carcinoma with clinically apparent (cN1), but not extensive, lymph node involvement and without other factors for poor prognosis. Arch Endocrinol Metab 2015;59(4):285-91.
18) Schlumberger M, Catargi B, Borget I, Deandreis D, Zerdoud S, Bridji B, et al. Strategies of radioiodine ablation in patients with low-risk thyroid cancer. N Engl J Med 2012;366(18):
1663-73.
19) Sohn SY, Choi JY, Jang HW, Kim HJ, Jin SM, Kim SW, et al. Association between excessive urinary iodine excretion and failure of radioactive iodine thyroid ablation in patients with papillary thyroid cancer. Thyroid 2013;23(6):741-7.
20) Ha S, Oh SW, Kim YK, Koo do H, Jung YH, Yi KH, et al. Clinical outcome of remnant thyroid ablation with low dose radioiodine in Korean patients with low to intermediate- risk thyroid cancer. J Korean Med Sci 2015;30(7):876-81.