원저1 원저2
원저4 원저3
원저5
원저8 원저9 증례1 증례2 증례3 증례4 증례5 증례6 증례7
J Korean Skull Base Society 11권 2호 : 48~52, 2016
Department of Neurosurgery, St. Vincent’s Hospital, College of Medicine, The Catholic University of Korea, Suwon, Korea
Stephen Ahn, M.D., Seung Ho Yang, M.D., Jae Hoon Sung, M.D., Sang Won Lee, M.D.
The middle fossa approach has undergone several modifications to expand its exposure along the cerebellopontine angle, petrous apex, tentorium and clivus. The middle fossa anterior transpetrosal approach, so called Kawase’s approach, is designed for the anterior cerebellopontine angle, the ventral surface of pons, and the upper clivus. The purpose of the study is to summarize the surgical experiences of anterior petrosal approach for the treatment of skull base tumor performed by a neurosurgeon.
Eight patients (6 women and 2 men) underwent frontotemporal craniotomy and anterior petrosal approach for skull base tumor resection. They included 3 trigeminal schwannomas, 3 meningiomas, 1 chondroma, and 1 metastasis. The median age was 57.5 years (range, 43-72). Three patients with trigeminal schwannomas and 1 patient with chondroma achieved total resection using the classic anterior petrosectomy without dura opening. For petroclival meningioma, opening of posterior fossa dura and coagulation of petrosal sinus was additionally performed. However, surgical corridor was limited anteriorly by mandibular nerve, laterally by internal auditory canal, and posteriorly by tentorium. Neurological deterioration developed postoperatively in 2 patients with petroclival meningioma.
It is suggested that anterior petrosal approach is suited for accessing middle fossa lesions with smaller petroclival components.
Surgical experiences of anterior petrosal approach for skull base tumor resection in a single institution
논문 접수일 : 2016년 8월 5일 논문 완료일 : 2016년 8월 30일
주소 : Department of Neurosurgery, St. Vincent’s Hospital, College of Medicine, The Catholic University of Korea, 93-6 Chi-dong, Paldal-gu, Suwon, 442-723, Korea Tel : +82.31-249-8303
Fax : +82.31-245-5208 E-mail : [email protected]
Seung Ho Yang, MD.
교신저자
skull base, middle fossa, meningioma, petrosal Key Words
원저7 원저6 종설1
▒ INTRODUCTION
The middle fossa approach and its various extended modification have developed for accessing vascular and neoplastic lesions of the petrous apex, upper petroclival regions, petrous internal carotid artery, and internal acoustic canal.4, 5, 8) Using the middle fossa corridor, Kawase and colleagues expanded its indications to include an extradural anterior petrosectomy with subsequent opening of the middle fossa dura mater and division of the superior petrosal sinus and the tentorium to access petroclival meningiomas and basilar artery aneurysm.9, 10) Previously, we reported the case series with middle cranial fossa tumors via transzygomatic approach with intraoperative neuromonitoring.12) A simple transzygomatic approach provides a wide surgical corridor for accessing the cavernous sinus, petrous apex, and subtemporal regions. Although an osteotomy of the zygoma makes a flat trajectory to the skull base, the most important issue is to understand the anatomical orientation and manipulate neurovascular structure meticulously.
In this article, we report our surgical experiences and clinical outcomes of 8 patients with skull base tumor treated with anterior petrosal approach at a single institution.
▒ MATERIALS AND METHODS
Eight patients underwent frontotemporal craniotomy and anterior petrosal approach for skull base tumors from 2007 to 2012 by a neurosurgeon (SH Yang). They included 3 trigeminal schwannomas, 3 meningiomas, 1 chondroma, and 1 metastasis. They all underwent frontotemporal craniotomy with anterior petrosectomy for resection of skull base tumors. We collected the clinical information in the retrospective manner.
Our surgical techniques included subfascial dissection of temporalis muscle, frontotemporal craniotomy. Several structures of the middle skull base are sequentially unroofed to untether and retract the temporal lobe extradurally to expose the middle fossa and posterior petroclival region.
After that the superior orbital fissure and foramen rotundum are seen. The middle meningeal artery is identified in the foramen spinosum and can be ligated. The second and third division of trigeminal nerve and greater superficial petrosal nerve (GSPN) are identified. After drilling petrous ridge off, petrous internal carotid artery and posterior fossa dura are visualized(Fig. 1).
Fig. 1 A
C
B
A. Anterior clinoidectomy after frontotemporal craniotomy and ligation of middle meningeal artery (MMA).
B. Identification of the second and third division of trigeminal nerve through foramen rotundum and ovale. Anterior petrous portion accessed.
C. Identification of petrous segment of internal carotid artery (ICA) follwoing anterior petrosectomy.
▒ RESULTS
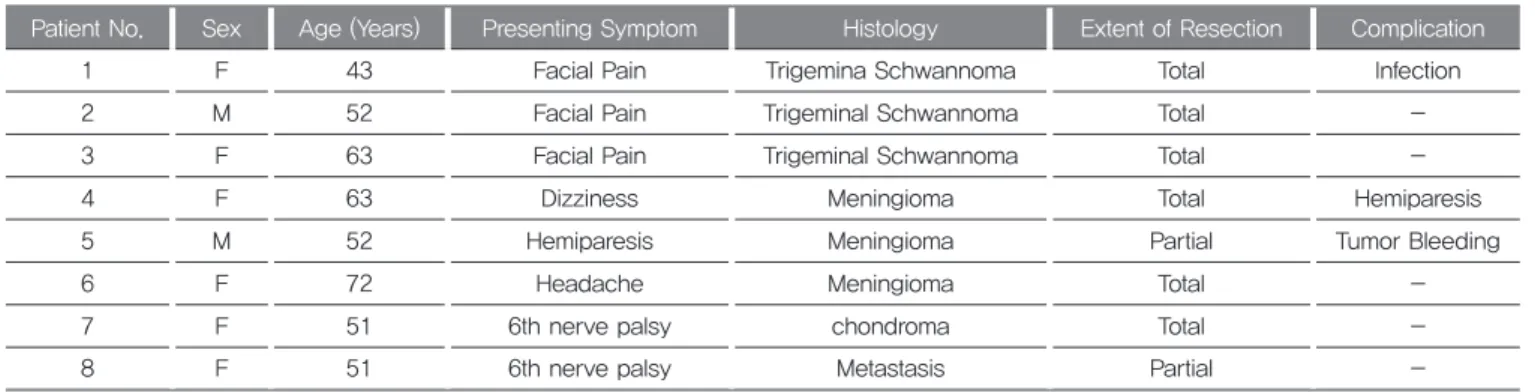
Eight patients who underwent surgery via the anterior petrosal approach for the treatment of tumors at petroclival regions were enrolled in this study. There were 2 males and 6 females, and their ages ranged from 43-72 years (mean age, 57.5 years). The patients mainly presented with facial pain (37.5%), 6th nerve palsy (25.0%), hemiparesis (12.5%), headache (12.5%) and dizziness (12.5%). The underlying pathologies included 3 trigeminal schwannomas, 3 meningiomas, 1 chondroma and 1 metastasis. The characteristics of the patients are summarized in Table 1. The diameters of schwannomas and meningiomas are 24~52mm and 20~46mm, respectively. Total and partial resections were achieved in 6 and 2 patients, respectively.
The following surgical complications occurred: wound infection (case no.1), hemiparesis (case no.4); and postoperative tumor bleeding (case no.5). Hemiparesis was caused by venous infarction after tumor removal.
Two patients with trigeminal schwannoma developed facial dysesthesia postoperatively.
Illustrated case
A 51-year-old woman was referred for lateral gaze palsy of the right eye. Preoperative magnetic resonance images (MRI) showed a space-occupying lesion in the right Meckel’s cave. Skull base computed tomography (CT) showed bony erosive change in the anterior petrous portion.
The patient underwent tumor excision using an anterior
petrosal approach. A postoperative MRI revealed total removal of the lesion. The histopathologic findings were consistent with a chondroma. There was no neurological complication postoperatively(Fig. 2).
▒ DISCUSSION
Many cranial base approaches have been described for treating lesions of the petroclival region.3, 6, 7, 11, 16) Anterior petrosal approach is ideally suited to addressing lesions that involve the middle fossa near trigeminal nerve.
Kawase's approach is limited by the petrous ridge, GSPN, mandibular nerve, and nerves inside the internal auditory canal. The region is devoid of vascular or nerve branches.
This approach requires retraction of the temporal lobe and draining veins. The vein of Labbe is of particular importance in the dominant hemisphere. This procedure is time consuming because a portion of the petrous apex shoud be resected. Alternatively, the retrosigmoid approach can be used in isolation to address lesions of the posterior fossa, provided that exposure of trigeminal nerve at Meckel's cave or of midline brainstem structures is not required. Removing the suprameatal tubercle provides additional exposure.13)
Lesions ideally suited for anterior petrosal approach involve considerably more of the middle fossa than the posterior fossa (e.g., trigeminal schwannomas, Meckel's cave meningiomas, or chondrosarcomas). Lesions with significant mass in the posterior fossa are better served
Table 1. Clinical Summary of 8 Patients underwent anterior petrosal approach
Patient No. Sex Age (Years) Presenting Symptom Histology Extent of Resection Complication
1 F 43 Facial Pain Trigemina Schwannoma Total Infection
2 M 52 Facial Pain Trigeminal Schwannoma Total -
3 F 63 Facial Pain Trigeminal Schwannoma Total -
4 F 63 Dizziness Meningioma Total Hemiparesis
5 M 52 Hemiparesis Meningioma Partial Tumor Bleeding
6 F 72 Headache Meningioma Total -
7 F 51 6th nerve palsy chondroma Total -
8 F 51 6th nerve palsy Metastasis Partial -
from a retrosigmoid approach.2)
We have performed the anterior petrosal approach for the resection of tumors involving both the middle and posterior fossa. Trigeminal schwannomas have been accessed and removed safely via anterior petrosal approach even though a considerable portion of the tumor is located in the posterior fossa. However, meningiomas involving both the middle and posterior fossa have different consistencies and tight adhesion to surrounding structures than schwannomas have. The surgical morbidities occurred in patients with petroclival meningioma which are supplied by many arterial feeders from skull base dura. Surgical fields provided by anterior petrosal approach are not sufficient to manipulate the neurovascular structures surrounding the tumor with surgical freedom. The consistency and degree of neurovascular involvement of any particular lesion play more significant roles in influencing the extent of resection than the choice of surgical approach.14, 15) Cranial nerve paresis is an almost obligatory byproduct of treating large
and complex vascular and neoplastic lesions of the central cranial base.1) The oculomotor and trochlear nerves are the most vulnerable to this complication, owing to the trajectory through the tentorial incisura. In our series, two patients experienced trigeminal hypesthesia following surgery of trigeminal schwannomas.
It is suggested that anterior petrosal approach is suited for accessing middle cranial fossa lesions with smaller petroclival lesions. It is mandatory to build the knowledge of tumor pathology as well as to learn the surgical technique for skull base surgery.
Fig. 2 A
C D E
B
A. Lateral gaze palsy of the right eye.
B. Preoperative MR images showing a round mass in the right Meckel’s cave. High signal intensity on T2-weighted image, iso signal on FLAIR image, heterogeneously enhanced on T1-weighted image with gadolium and low signal on T1-weighted image without gadolium noted (clockwise direction).
C, D. Intraoperative pictures indicating anterior petrous ridge and the exposure of tumor portion without dura opening.
E. Postoperative T2 axial (left) and T1-weighted image with gadolium (right) demonstrating total tumor removal.
References
1. Al-Mefty O, Ayoubi S, Smith RR: The petrosal approach: indications, technique, and results. Acta Neurochir Suppl (Wien) 53:166-170, 1991 2. Chang SW, Wu A, Gore P, Beres E, Porter RW, Preul MC, Spetzler RF, et al.
Quantitative comparison of Kawase's approach versus the retrosigmoid approach: implications for tumors involving both middle and posterior fossae.
Neurosurgery 64: ons44-52, 2009
3. Hakuba A, Nishimura S, Jang BJ. A combined retroauricular and preauricular transpetrosal-transtentorial approach to clivus meningiomas. Surg Neurol 30:
108-116, 1988
4. Harsh GR, Sekhar LN. The subtemporal transcavernous, anterior transpetrosal approach to the upper brainstem and clivus. J Neurosurg 77: 709-717, 1992 5. Horgan MA, Anderson GJ, Schwartz MS, Schwartz MS, Spektor S,
McMenomey SO, et al. Classification and quantification of the petrosal approach. J Neurosurgery 93:108-112, 2000
6. House WF, De la Cruz A, Hitselberger WE. Surgery of the skull base:
Transcochlear approach to the petrous apex and clivus. Otolaryngology 86:
orl770-779, 1978
7. House WF, Hitselberger WE. The transcochlear approach to the skull base.
Arch Otolaryngol 102: 334-342, 1976
8. Kanzaki J, Kawase T, Sano K, Shiobara R, Toya S. A modified extended middle cranial fossa approach for acoustic tumors. Arch Oto-Rhino-Laryngol 217: 119-121, 1977
9. Kawase T, Shiobara R, Toya S. Anterior transpetrosal-transtentorial approach for sphenopetroclival meningiomas: surgical method and results in 10 patients. Neurosurgery 28: 869-876, 1991
10. Kawase T, Toya S, Shiobara R, Mine T. Transpetrosal approach for aneurysms of the lower basilar artery. J Neurosurg 63: 857-861, 1985
11. Samii M, Ammirati M. The combined supra-infratentorial pre-sigmoid sinus avenue to the petro-clival region. Surgical technique and clinical applications.
Acta Neurochir (Wien) 95: 6-12, 1988
12. Son BC, Lee SW, Kim S, Hong JT, Sung JH, Yang SH. Transzygomatic approach with intraoperative neuromonitoring for resection of middle cranial fossa tumors. J Neurol Surg B Skull Base 73: 28-35, 2012
13. Song Y, Moon SM, Rhee JJ, Kim CJ, Kim JH, Lee JK. Suboccipital Suprameatal Approach for Petrosal Meningiomas Extended into Meckel’s Cave. J Korean Neurosurg Soc 33: 132-136, 2003
14. Tanriover N1, Sanus GZ, Ulu MO, Tanriverdi T, Akar Z, Rubino PA, et al. Middle fossa approach: microsurgical anatomy and surgical technique from the neurosurgical perspective. Surg Neurol 71: 586-596, 2009
15. Terasaka S, Sawamura Y, Goto S, Fukushima T. A lateral transzygomatic- transtemporal approach to the infratemporal fossa: technical note for mobilization of the second and third branches of the trigeminal nerve. Skull Base Surg 9: 277-287, 1999
16. Quinones-Hinojosa A, Chang EF, Lawton MT.: The extended retrosigmoid approach: An alternative to radical cranial base approaches for posterior fossa lesions. Neurosurgery 58: ons208-214, 2006