Multi-detector row computed tomographic arthrogra- phy (MDCTA) and magnetic resonance arthrography (MRA) are superior to computed tomography (CT) or magnetic resonance imaging (MRI) for evaluating shoul- der instability (1, 2). Previous reports have indicated
that MRA is more accurate for evaluating the capsu- loligamentous complex, the glenoid labrum, the intra- capsular portion of the long head of the biceps tendon, and the rotator cuff than CT arthrography (1, 2).
Therefore, MRA has been a useful technique for diag- nosing labral lesions that induce shoulder instability (1- 5).
CT shows high accuracy for detecting cortical defect and calcification of tendon and ligament. MDCTA al- lows multiplanar images of the lesion, and these images
Comparison of MDCTA (16-Slice Multi-Detector Row Computed Tomography Arthrography) and MRA (Magnetic Resonance Arthrography) for Detecting Labral Lesions of the Shoulder
1Seung A Choi, M.D., Jang Gyu Cha, M.D., Hyun Sook Hong, M.D., Deuk Lin Choi, M.D., Jai Soung Park, M.D., Hae Kyung Lee, M.D., Dae Ho Kim, M.D.
1Department of Radiology, Soonchunhyang University Bucheon Hospital Received May 31, 2007 ; Accepted September 10, 2007
Address reprint requests to : Jang Gyu Cha, M.D., Department of Radiology, Soonchunhyang University Bucheon Hospital, 1174, Jung- dong, Wonmi-gu, Gyeonggi-do 420-021, Republic of Korea.
Tel. 82-32-621-5851 Fax. 82-32-621-5874 E-mail: [email protected]
Purpose: To compare the accuracy of 16-slice multi-detector row computed tomo- graphic arthrography (MDCTA) and magnetic resonance arthrography (MRA) for mak- ing the diagnosis and classification of labroligamentous injuries.
Materials and Methods: This study is a prospective series that used MRA and MDCTA to examine 23 patients who complained of shoulder instability. Two radiologists inde- pendently analyzed the MRA and MDCTA. The sensitivity, specificity, accuracy, posi- tive and negative predictive values were calculated from the arthrograms and the arthroscopic findings. The images of MDCTA and MRA corresponded with the find- ings on arthroscopy.
Results: Both imaging modalities had the same sensitivity for detecting Bankart le- sions (n=10, 90%) and posterior labral tears (n=2, 50%) on McNemar test (p=1.00).
For superior labrum anterior-to-posterior (SLAP) lesions, 6 MRA cases and 4 MDCTA cases corresponded with the arthroscopic findings. The difference between the sensi- tivities of MDCTA (66.7%) and MRA (100%) was not significant (p=0.09).
Conclusion: We suggest that the sensitivity of diagnosing labral lesions that induce shoulder instability is similar for MDCTA and MRA. MDCTA is effective for diagnos- ing and evaluating shoulder instability.
Index words :Shoulder
Magnetic resonance (MR) Arthrography
Tomography X- Ray Computed
are comparable to MRA. Moreover, MDCTA allows re- construction images with 1 mm or thinner sectioning in any direction in the target lesion, whereas MRA can show only images with a fixed section thickness. The ca- pability of MDCTA for isotropic data acquisition with high spatial resolution is a precondition for accurate imaging in the anatomically complex shoulder region (1, 3). Waldt et al. (3) have already demonstrated that MD- CTA is as effective as MRA for detecting variants of the superior labrum and labro-bicipital complex.
Because the ability of MDCTA to identify pathologic labral lesions has not yet been demonstrated, we prospectively compared the accuracy of MDCTA and MRA for making the diagnosis and classification of labroligamentous injuries, and we used the arthroscopic findings as the reference standard.
Materials and Methods
Patients
Twenty-three shoulder joints (21 men and 2 women, mean age: 28 years, age range: 17-52 years) were evalu- ated between August 2005 and January 2006 for shoul- der instability. This study was approved by the ethical committee at our institution.
A contrast agent consisting of a 1:5 mixture of iome- prol (Iomeron 300; Ilsung, Seoul, Korea) and gadopente- tate dimeglumine (Magnevist; Schering, Berlin, Germany) diluted 1:250 in 20 ml of saline solution was prepared for a total volume of 24 mL (1). The patients underwent fluoroscopic-guided arthrography in the neu- tral position with using the previously mixed iodinated and paramagnetic contrast agents prior to MDCT and MRI. On fluoroscopy, the anterior approaching intra-ar- ticular position of the needle (21 gauge spinal needle;
Hakko, Nagano-ken, Japan) was confirmed with visual- ization of the iodinated contrast agent (Iomeron 300) in the joint space. The volume of injected solution ranged from 10 to 24 mL. No side effects were observed. The patients were examined using MRA followed by MDC- TA, after obtaining their informed consent for perform- ing one-shot CT-MR arthrography.
The joint was explored, and the superior labrum and labor-bicipital complex were inspected macroscopically as the reference standard. All 23 patients underwent shoulder arthroscopy by one orthopedic surgeon who had 8 years experience. The result for each modality was compared with the intraoperative arthroscopic as- sessment.
Patients with Bankart variants seen on arthroscopy were excluded (n=8). Because of their chronic clinical history, their arthroscopic findings may not correspond to the pathologic findings. So, fifteen patients (14 men and 1 women, mean age: 26 years, age range: 17-52 years) formed the final study group for statistical analy- sis.
Imaging protocol
MRA was performed on a Signa 1.5-T system (GE Medical Systems, Milwaukee, WI, USA). The shoulder joint in the neutral position, was in a dedicated, phased- array, shoulder coil (Quadrature coil; GE Medical Systems). The T1-weighted spin-echo images (T1WSE) were taken in the transverse and oblique coronal planes [500/10 (repetition time msec/echo time msec, mesuar- ing 4-mm-thick sections, with 140-140 mm field of view (FOV), 1 mm intersection gap, 256-192 pixel ma- trix, and averaging of two signals]. The three-dimension- al fat-suppressed spoiled gradient-echo images (3D FSP- GR) were obtained in the transverse plane (25/4, 25°flip angle, 3-mm-thick sections, 140×140 mm FOV, no in- tersection gap, 256×192 pixel matrix, two signals aver- aged). The gradient-recalled-echo T2* images (GRE T2*) were obtained in the transverse plane (22/600, 20°flip angle, 4-mm-thick sections, 140-140 mm FOV, 1 mm intersection gap, 256×192 pixel matrix, three signals av- eraged). The fast spin-echo proton density-weighted im- ages (FSEPD) in the oblique coronal and oblique sagittal planes were used (30/3000, 10 echo train length, 4-mm- thick sections, 140×140 mm FOV, 1 mm intersection gap, 256×256 pixel matrix, two signals averaged). Fat- suppressed T2-weighted fast spin-echo images (T2W FS- FSE) were also taken in the oblique coronal plane (85/4000, 14 echo train length, 3-mm-thick sections, 140
×140 mm FOV, 1 mm intersection gap, 256×224 pixel matrix, three signals averaged).
MSCTA was performed on a 16-row multislice CT unit (Sensation 16; Siemens Medical Solutions, Erlangen, Germany). The scan parameters used were a tube voltage of 120 kV, a tube current of 150 mA, feed/rotation 9 mm, collimation beam 0.75 mm, effec- tive pitch 0.75, and the FOV at acquisition of 150 mm in the transverse plane. The image data were reconstruct- ed with a 360°interpolation algorithm and a high-reso- lution kernel (B60s sharp) at a slice thickness of 1 mm, a 0.7 mm reconstruction increment, and a matrix of 512×
512 pixels. Oblique coronal and oblique sagittal re- constructions were generated on a 3D workstation, with
3-mm-thick sections and a 3-mm reconstruction inter- val.
Image analysis
The MRA and MDCTA were analyzed independently by two musculoskeletal radiologists with 5 and 4 years of specialty experience, respectively. They had access to only the clinical history. The images were interpreted separately with 1 week between the reading sessions.
The MRA in the first session and MDCTA in the second session were evaluated individually. Two radiologists analyzed the type of labral lesion that induced the shoul-
der instability. The types included classic and bony Bankart lesions, Bankart variants (anterior labroliga- mentous periosteal sleeve avulsion (ALPSA), Perthes le- sion), posterior labral tears, superior labrum anterior-to- posterior (SLAP) lesions, anterosuperior labral tears and sublabral recesses. Consensus was finally obtained in the case of initial disagreement.
The criteria for a classic Bankart lesion were a frag- ment of labrum attached to the anterior band of the infe- rior glenohumeral ligament with a ruptured scapular pe- riosteum that was “floating” in the anteroinferior aspect of the glenohumeral joint (6). Combined evidence of an
A B C
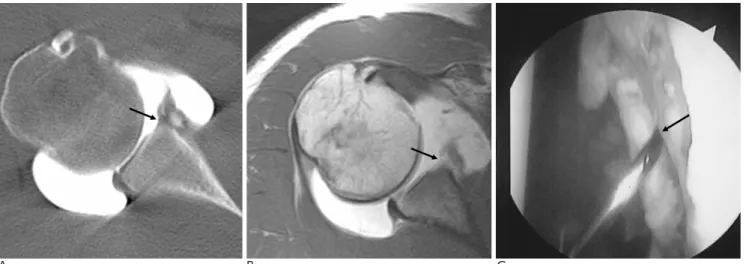
Fig. 1. Right shoulder of a 19-year-old man who suffered with recurrent shoulder dislocations for 3 years.
A. MDCTA in the transverse plane shows contrast medium interposition (arrow) between the glenoid rim and the detached capsu- lolabral complex.
B. T1WSE (TR/TE, 500/10) of MRA in the transverse plane shows a detached anterior labrum (arrow).
C. Arthroscopy confirmed the Bankart lesion (arrows).
A B C
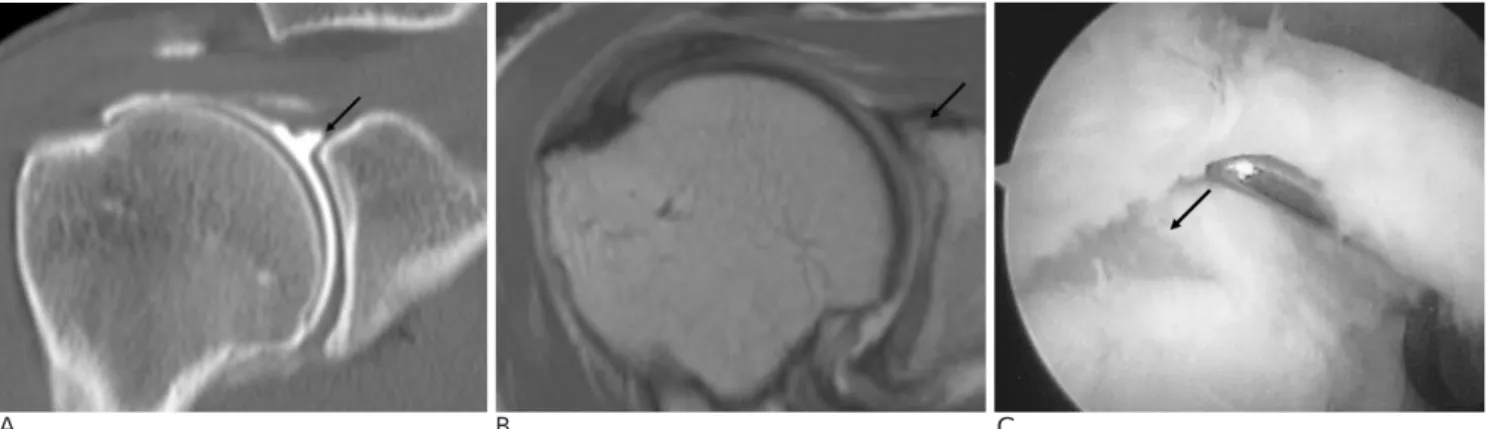
Fig. 2. Left shoulder of a 23-year-old man who suffered with anterior shoulder instability for 2 years after falling during a soccer game.
A. MDCTA in the transverse plane shows a slightly thickened, partially detached anterior labrum without displacement (arrow).
B. T1WSE (TR/TE, 500/10) of MRA in the transverse plane shows a fragmented anterior labrum with an intact periosteum (arrow).
C. Arthroscopy confirmed the Perthes lesion (arrows).
osseous lesion led to the diagnosis of a bony Bankart le- sion rather than a classic Bankart lesion (4, 6). ALPSA was seen as a tear of the anteroinferior labrum without rupture of the anterior scapular periosteum, stripped and medially displaced inferior glenohumeral ligament, labrum and periosteum (7). A Perthes lesion was also defined as a labroligamentous avulsion, but with a me- dially stripped intact periosteum (7). A posterior labral tear consisted of posterior labral, capsular and glenoid rim injury that was secondary to posterior dislocation or subluxation of the shoulder joint (6). The criteria for a SLAP lesion were extension of a labral tear into the su- perior labrum with the lateral or superior portion (3). An anterosuperior labral tear was a tear limited to the an- terosuperior aspect of the labrum, with or without asso- ciated lesions in the superior and middle portions of the glenohumeral joint (4). A sublabral recess was defined as a sulcus with smooth borders and a medial extension between the superior labrum and bony glenoid (3, 8). A tear of the glenoid labrum was diagnosed when the nor- mal cross-sectional appearance was disrupted or when an abnormal signal intensity was noted. The signal in- tensity on MRA was compared to that of the nearby muscles or circumferential labrum (9).
Statistical analysis
The sensitivity, specificity, accuracy, positive and neg- ative predictive values were calculated for detecting labral lesions from the imaging and gross arthroscopic findings. Statistically significant differences were calcu- lated using the McNemar test. Statistical significance was set at p<0.05. All statistical operations were
processed using Stata statistical software (version 9.0;
Stata, College Station, TX, U.S.A.).
Results
Macroscopic assessment of the two modalities (MRA and MDCTA)
On arthroscopy, ten Bankart lesions (n=8 classic Bankart lesions, n=2 bony Bankart lesions), two posteri- or labral tears and 6 SLAP lesions were visualized in the 18 shoulder joints. Three shoulders with SLAP lesion had another lesion, including a classic Bankart lesion, bony Bankart lesion and posterior labral tear. No antero- superior labral tears or sublabral recesses were detected on arthroscopy.
The diagnoses, based on MDCTA and MRA, were the same for 16 of the 18 labral lesions; the exceptions were two SLAP lesions. The arthroscopic and imaging find- ings corresponded to nine Bankart lesions and one pos- terior labral lesion. One bony Bankart lesion was incor- rectly diagnosed as ALPSA on both imaging modalities.
For the SLAP lesions, six cases on MRA and four cases on MDCTA matched the arthroscopic findings. Two missed SLAP lesions on MDCTA were in fact sublabral recesses (Table 1).
For the eight Bankart variants (n=7 ALPSA, n=1 Perthes lesion), MRA correctly diagnosed two cases and MDCTA made three correct diagnoses. The intact pe- riosteum of the Bankart variants on arthroscopy ap- peared as a tear on MRA and MDCTA.
A B C
Fig. 3. Right shoulder of a 46-year-old man who suffered with chronic anterior shoulder dislocation for 10 years after an injury playing volleyball.
A. MDCTA in the coronal oblique plane reveals contrast medium interposed within the superior portion of the labrum (arrow).
B. T1WSE (TR/TE, 500/10) of MRA in the coronal plane demonstrates an irregularity and pooling of contrast material within the su- perior labrum (arrow), with no evidence indicating complete extension of the lesion throughout the superior labral substance.
C. The arthroscopic view was diagnosed as a SLAP tear (arrows).
Statistical comparison
The respective sensitivity, specificity, accuracy, posi- tive and negative predictive values for detecting Bankart lesion were 90%, 100%, 93.3%, 100% and 83.3% for both MRA and MDCTA (Table 1). The respective results for detecting posterior labral tears were same on both imaging modalities: 50%, 100%, 93.3%, 100% and 92.9%. MDCTA and MRA had the same sensitivities for detecting Bankart lesions and posterior labral tears (p=1.00). For SLAP lesions, the sensitivity, specificity, accuracy, positive predictive and negative predictive values for MRA were all 100% and those for MDCTA were 66.7%, 100%, 86.7%, 100% and 81.8%, respective- ly. The difference in the sensitivity between the two groups for detecting SLAP lesions was not significant (p=0.09; Table 1) on McNemar test.
Discussion
The discrepancy in size between the small glenoid fos- sa and the large humeral head gives the glenohumeral joint great mobility, but it also makes the shoulder joint particularly vulnerable to dislocation (4). Anteroinferior dislocation is the most frequent cause of anterior gleno- humeral instability and produces a constellation of le- sions (classic and bony Bankart lesions, Bankart vari- ants, ALPSA and Perthes lesions and anterosuperior labral tears). A posterior labral tear may occur during posterior dislocation of the shoulder joint. SLAP lesions involve the superior part of the labrum with varying de- grees of biceps tendon involvement (4, 10, 11). It is im- portant to differentiate a SLAP lesion from a sublabral recess of the superior glenoid labrum to avoid unneces- sary surgery (2, 8, 12). Therefore, radiologically assess-
ing instability of the glenohumeral joint is indispensable for surgical planning and selecting the appropriate treat- ment (13).
MRA and CT arthrography are highly efficient imag- ing techniques for diagnosing labral lesions, based on the high contrast resolution from the intra-articular di- luted paramagnetic contrast or iodinated agent, and the distension of the joint capsule (1, 2). Of the two modali- ties, MRA has been considered the reference standard for the workup of patients with shoulder instability, and MRA has significantly higher sensitivity and specificity (2, 13, 15). For labral lesions in 28 patients, Chandnani et al. (14) reported a sensitivity of 96% for MRA com- pared to 93% and 73% for MRI and CT arthrography, respectively. Spiral single-detector row CT did not have sufficient sensitivity for detecting labral lesions. The spi- ral four-detector row CT that was available in 1998 im- proved the performance by a factor of eight, and this was the result of combining multiple rows of detectors and faster gantry rotation with narrow collimation. In 2002, 16-slice row CT scanners were introduced, with a further reduction of section collimation and scan time (16). The advantages of CT arthrography for detecting the calcification of tendon and ligament, and the dam- age of cortical bone are already acknowledged (1). In particular, MDCTA allows multiplanar images of the le- sions, the same as with MRA. MDCTA even makes re- construction images with sections that are less than 1 mm thick in any direction, whereas MRA can show on- ly images of a fixed section thickness. Owing to the higher spatial resolution of MDCTA, even small sections of sublabral recesses anterior or posterior to the biceps insertion were better delineated with MDCTA than with MRA (3). Contrast media extension posterior to the Table 1. Comparison of MDCTA and MRA for Detecting Labral Lesions
Labral Op. Modality True- True- False- False- Sensitivity Specificity Accuracy Positive Negative lesion finding positive negative positive negative (%) (%) (%) predictive predictive
(p value) (n=18) value (%) value (%)
Bankart 10 MDCTA 9 5 0 1 90 100 93.3 100 83.8
lesion MRA 9 5 0 1 90 100 93.3 100 83.8
(p=1.00)
Posterior 2 MDCTA 1 13 0 1 50 100 93.3 100 92.9
labral tear MRA 1 13 0 1 50 100 93.3 100 92.9
(p=1.00)
SLAP lesion 6 MDCTA 4 9 0 2 66.7 100 86.7 100 81.8
(p=0.09) MRA 6 9 0 0 100 100 100 100 100
Note; * MDCTA = 16-slice multi-detector row computed tomographic arthrography, MRA = Magnetic resonance arthrography 18 lesions on intra-operative arthroscopy (Op. findings) in 15 shoulder joints
Statistical analysis by McNemar test
biceps anchor during MRA should not be regarded as a reliable criterion for a SLAP lesion (3). However, MDC- TA is appropriate for a patient with a metallic object in the shoulder and it is cheaper than MRA.
In some patients who have a chronic history of shoul- der instability, a Perthes lesion detected on MRA may be indistinguishable from a normal labrum seen on arthroscopy. Based on intraoperative arthroscopy, the Bankart variants may be indistinguishable from the oth- er classification of labral lesions and the reliability of the surgical findings may be diminished (7). Therefore, we didn’t include Bankart variants in the statistical analysis of our study.
This prospective study demonstrated that MDCTA and MRA have almost equal sensitivity for labral le- sions. No statistically significant differences between the two imaging modalities were found on McNemar test. Therefore, any comparison of our results with oth- er published results differs according to the diagnostic performance of the two modalities for detecting labral lesions (1). Our results revealed that both MRA and MD- CTA are useful techniques for diagnosing labral lesions that induce shoulder instability. MDCTA can help eval- uate the presence, degree and classification of a labral tear. This modality can also be used in patients with a metallic object in the shoulder. Conversely, considering MRA as a possible next step after performing MDCTA is an interesting diagnostic option in selected cases.
Additional studies will help to further evaluate the per- formance and applications of this modality.
This study has several limitations. First, only a small number of shoulders were evaluated. We presumed that the sensitivity of CT for detecting calcifications and bone injuries was greater, while MR was more sensitive for diagnosing soft tissue abnormalities, as based on the optimal MR contrast resolution. Nevertheless, in this study, MDCTA was not superior to MRA for detecting the bony defects of bony Bankart lesions. An additional study with a large number of cases should help to clarify the statistical results in this study. One of two bony Bankart lesions was missed on both MDCTA and MRA, resulting in the same sensitivity of 50% for both modali- ties, but this was too few cases to draw any final conclu- sion. We also expect a study focusing on a large number of SLAP lesions will show higher detectability on MRA than that on MDCTA. This is because one limitation of MDCTA includes the difficulty in evaluating a SLAP le- sion that presents as abnormal signal intensity on MRA.
Second, mixed contrast material was used in this
study. The stability of the mixture of gadolinium chelates and iodinated contrast agents has already been reported on, and its clinical safety was manitest for per- forming CTA and MRA of the ankle and wrist as a one- shot CTA-MRA exam (1, 17). Nevertheless, a decrease in the signal intensity on MRA was seen due to the dilu- tion of the gadolinium chelate mixed with the iodinated contrast agent (1). This might have reduced the sensitivi- ty of MRA for Bankart variants in this study, as com- pared to previous studies (1, 3, 4, 7, 13). So, the MRA protocol included one T1-wighted and five PD/T2/T2*- weighted pulse sequences.
In conclusion, the sensitivity of detecting labral lesions that induce shoulder instability was almost equal for MDCTA and MRA in this prospective study. The capa- bility of MDCTA for isotropic data acquisition with high spatial resolution appears to be a promising precondi- tion for the accurate diagnosis and classification of labral lesions. MDCTA is very effective for the diagnosis and evaluation of shoulder instability.
References
1. Aliprandi A, Fausto A, Quarenghi M, Modestino S, Randelli P, Sardanelli F. One-shot CT and MR arthrography of the shoulder with a mixture of iodinated and paramagnetic contrast agents us- ing arthroscopy as a gold standard. Radiol Med 2006;111:53-60 2. Bencardino JT, Beltran J, Rosenberg ZS, Rokito A, Schmahmann S,
Mota J, et al. Superior labrum anterior-posterior lesions: diagnosis with MR arthrography of the shoulder. Radiology 2000;214:267- 271
3. Waldt S, Metz S, Burkart A, Mueller D, Bruegel M, Rummeny EJ, et al. Variants of the superior labrum and labro-bicipital complex:
a comparative study of shoulder specimens using MR arthrogra- phy, multi-slice CT arthrography and anatomical dissection. Eur Radiol 2006;16:451-458
4. Beltran J, Rosenberg ZS, Chandnani VP, Cuomo F, Beltran S, Rokito A. Glenohumeral instability: evaluation with MR arthrog- raphy. Radiographics 1997;17:657-673
5. Beltran J, Bencardino J, Mellado J, Rosenberg ZS, Irish RD. MR arthrography of the shoulder: variants and pitfalls. Radiographics 1997;17:1403-1412
6. Stoller DW, Tirman PFJ, Bredella MA, Beltran S, Branstetter RM, Blease SCP. Diagnostic Imaging: Orthopaedics. Philadelphia: Amirsys, 2004:I62-I65
7. Waldt S, Burkart A, Imhoff AB, Bruegel M, Rummeny EJ, Woertler K. Anterior shoulder instability: accuracy of MR arthrog- raphy in the classification of anteroinferior labroligamentous in- juries. Radiology 2005;237:578-583
8. De Maeseneer M, Van Roy F, Lenchik L, Shahabpour M, Jacobson J, Ryu KN, et al. CT and MR arthrography of the normal and pathologic anterosuperior labrum and labral?bicipital complex.
Radiographics 2000;20:S67-S81
9. Kieft GJ, Bloem JL, Rozing PM, Obermann WR. MR imaging of re- current anterior dislocation of the shoulder: comparison with CT arthrography. AJR Am J Roentgenol 1998;150:1083-1087
10. Jee WH, McCauley TR, Katz LD, Matheny JM, Ruwe PA, Daigneault JP. Superior labral anterior posterior (SLAP) lesions of the glenoid labrum: reliability and accuracy of MR arthrography for diagnosis. Radiology 2001;218:127-132
11. Kreitner KF, Botchen K, Rude J, Bittinger F, Krummenauer F, Thelen M. Superior labrum and labral-bicipital complex: MR imaging with pathologic-anatomic and histologic correlation. AJR Am J Roentgenol 1998;170:599-605
12. Jin W, Ryu KN, Kwon SH, Rhee YG, Yang DM. MR arthrography in the differential diagnosis of type II superior labral anteroposteri- or lesion and sublabral recess. AJR Am J Roentgenol 2006;187:887- 893
13. Wischer TK, Bredella MA, Genant HK, Stoller DW, Bost FW, Tirman PF. Perthes lesion (a variant of the Bankart lesion): MR imaging and MR arthrographic findings with surgical correlation.
AJR Am J Roentgenol 2002;178:233-237
14. Chandnani VP, Yeager TD, DeBerardino T, Christensen K, Gagliardi, JA, Heitz DR, et al. Glenoid labral tears: prospective evaluation with MRI imaging, MR arthrography, and CT arthrog- raphy. AJR Am J Roentgenol 1993;161:1229-1235
15. Duc SR, Mengiardi B, Pfirrmann CW, Jost B, Hodler J, Zanetti M.
Diagnostic performance of MR arthrography after rotator cuff re- pair. AJR Am J Roentgenol 2006;186:237-241
16. Cademartiri F, Raaijmakers RH, Kuiper JW, van Dijk LC, Pattynama PM, Krestin GP. Multi-detector row CT angiography in patients with abdominal angina. Radiographics 2004;24:969-984 17. Schmid MR, Pfirrmann CW, Hodler J, Vienne P, Zanetti M.
Cartilage lesions in the ankle joint: comparison of MR arthrograpy and CTA. Skeletal Radiol 2003;32:259-265
대한영상의학회지 2007;57:471-477
견관절 전산화단층촬영 관절조영술과 자기공명 관절조영술의 비교:
견관절 관절순인대 열상의 진단
11순천향대학교 부천병원 영상의학과
최승아・차장규・홍현숙・최득린・박재성・이혜경・김대호
목적: 관절순인대 열상의 진단을 위한 16 slice 전산화단층촬영 관절조영술(16-slice multi-detector row computed tomographic arthrography; MDCTA)과 자기공명 관절조영술(magnetic resonance arthrography; MRA)의 진단율 을 비교한다.
대상과 방법: 견관절 불안정성을 호소하는 23명의 환자를 대상으로 MRA와 MDCTA를 모두 시행한 후 수술적 관 절경으로 병변을 확인하였다. 두 명의 영상의학 전문의가 개별적으로 MRA와 MSCTA를 판독하여 견관절 불안정 성을 유발하는 병변의 유무를 기술하였다. 관절경 소견을 기준으로 각 검사의 민감도, 특이도, 정확도 및 양성예측 도와 음성예측도를 구하고 McNemar test를 이용하여 민감도 차이를 비교하였다.
결과: 관절경에서Bankart variant를 제외한 15 개의 견관절 중 3 개에서 두 가지 병변이 혼재하여, 총 18예의 병 변을 확인하였다. Bankart lesion과 posterior labral tear의 진단에서 MRA와 MDCTA의 판독결과는 일치하였다. 결 과적으로 McNemar test를 이용한 통계분석에서 MRA와 MDCTA의 유의한 민감도 차이는 없었다.
결론: 견관절 불안정을 유발하는 관절순인대 열상의 질환에서, MDCTA의 진단율은 MRA의 진단율에 상당히 근접 하여, 진단에 유용하게 사용할 수 있다.