530
Comparison of the Predictors of Coronary Restenosis after Drug-Eluting Stent Implantation in Diabetic and Nondiabetic Patients
Soon Jun Hong, MD1, Moo Hyun Kim, MD2, Tae Hoon Ahn, MD3, Wan Joo Shim, MD1, Seong Mi Park, MD1, Jong Il Choi, MD1, Hyung Joon Joo, MD1, Seung Yong Shin, MD1, Sang Yup Lim, MD1 and Do-Sun Lim, MD1
1Department of Cardiology, Cardiovascular Center, Korea University Anam Hospital, Seoul, 2Department of Cardiology, Donga University Hospital, Busan, 3Department of Cardiology, Gachon University Hospital, Incheon, Korea
ABSTRACT
Background and Objectives: Coronary restenosis after drug-eluting stent (DES) implantation occurs more fre- quently in diabetic patients than in nondiabetic patients. We compared the parameters influencing the like- lihood of restenosis after DES implantation in diabetic and nondiabetic patients. Subjects and Methods: Pat- ients who underwent DES implantation (619 patients with 917 lesions, 211 diabetics and 408 nondiabetics), followed by 8 months coronary angiogram, were retrospectively identified using the percutaneous coronary inter- vention database and included in the present study [AH1]. Predictors of restenosis were identified by multi- variate logistic regression analyses. Results: The baseline characteristics of the patients, such as sex, body mass index, hypertension, hyperlipidemia, and smoking status, were similar between the diabetic and nondiabetic patients.
Restenosis (>50% of the diameter stenosis) occurred in 32 of 408 (7.8%) nondiabetic patients and in 32 (15.2%) of 211 diabetic patients (p<0.001). The use of a paclitaxel-eluting stent (PES), a higher level of C-reactive protein (CRP), longer stent length, smaller reference diameter (RD) before DES implantation, smaller RD and minimal lumen diameter after DES implantation were common predictors of restenosis in both the diabetic and non- diabetic patients after multivariate analyses. Current smoking status [odds ratio (OR)=3.213, 95% confidence in- terval (CI) 1.458 to 7.080 p=0.004] and right coronary lesions (OR=2.444, 95% CI 1.048 to 5.703, p=0.039) were predictors of restenosis in the diabetic patients, while higher body mass index (OR=1.322, 95% CI 1.054 to 1.659, p=0.016) and A-type lesions (OR=0.108, 95% CI 0.022 to 0.530, p=0.006) were predictors of rest- enosis in the nondiabetic patients. Conclusion: The use of PESs and higher levels of CRP were associated with restenosis regardless of the presence of diabetes. Moreover, small baseline and post-PCI reference diameter and longer stent length remained significant angiographic predictors of restenosis in both diabetic and nondiabetic patients, even in the era of DES implantation. (Korean Circ J 2007;37:530-537)
KEY WORDS: Diabetes mellitus;Drug-eluting stent;Coronary restenosis.
Introduction
The long-term clinical and angiographic outcomes after percutaneous coronary intervention (PCI) with bare- metal stents (BMSs) have been demonstrated to be worse in diabetic patients than in nondiabetic patients.1-3) Se-
veral studies have shown that the introduction of drug- eluting stents (DESs) has significantly reduced the an- giographic rates of restenosis in the later months after PCI.4-8) Coronary restenosis occurs more frequently in diabetic patients than in nondiabetic patients, even after DES implantation.9) In the era of DESs, no study has compared the clinical and angiographic predictors of coronary restenosis in diabetic and nondiabetic pat- ients after DES implantation.10)11) The objective of this multicenter observational retrospective cohort study was to compare the parameters that influence coronary restenosis after DES implantation in diabetic and non- diabetic patients.
Received: June 29, 2007 Revision Received: August 8, 2007 Accepted: August 31, 2007
Correspondence: Do-Sun Lim, MD, Department of Cardiology, Cardio- vascular Center, Korea University Anam Hospital,126-1 Anam-dong 5-ga, Seongbuk-gu, Seoul 136-705, Korea
Tel: 82-2-920-5445, Fax: 82-2-927-1478 E-mail: [email protected]
Subjects and Methods
Patient population
The patients were retrospectively identified for inclu- sion in the study using the Multicenter PCI Database Registry from April 2005 to August 2006. Three car- diovascular centers representing three major cities in Korea participated in the Multicenter PCI Database Registry. All clinical and angiographic data were sent to the core laboratory (Korea University, Seoul, Korea) and entered into the PCI database. From this database, DES-implanted patients (619 patients, 917 lesions)[211 diabetics, 315 lesions; 408 nondiabetics, 602 lesions]
with 8 full months of clinical and angiographic follow- up were retrospectively included in the study. Diabetes mellitus was defined as a history of diabetes, a fasting plasma glucose concentration ≥126 mg/dL, or the use of hypoglycemic medications. Systemic hypertension was defined as a systolic blood pressure ≥140 mmHg, diastolic pressure ≥90 mmHg, or the use of antihyper- tensive medication. Hyperlipidemia was defined as a total cholesterol level ≥200 mg/dL, a low-density lip- oprotein cholesterol level ≥130 mg/dL, or treatment with a lipid-lowering agent. Aٛsmoker was defined as someone with a current or recent history of smoking within the past year. Family history of premature cor- onary artery disease was defined as coronary artery di- sease in a male first-degree relative <55 years and fe- male first-degree relative <65 years. Body mass index was calculated by dividing the square of the patient’s height in meters from their weight in kilograms. We excluded patients with a prior history of interventional or surgical treatment for coronary artery disease, coro- nary artery total occlusion, or a contraindication for antiplatelet or anticoagulation therapy. Written informed consent was obtained from each patient in accordance with the Declaration of Helsinki, and the study was app- roved by the Korea University Hospital institutional review committees.
Drug-eluting stent implantation
Balloon angioplasty and stent implantation were performed according to standard clinical practice. The femoral or radial approach was used, and all patients were given 100 mg of aspirin combined with either 300 mg of clopidogrel or 500 mg of ticlopidine on the day before the procedure. Aspirin was given indefinitely, and 75 mg of clopidogrel or 250 mg of ticlopidine was administered once daily for 8 months. At the beginn- ing of the intervention, a heparin bolus of 100 units/kg was administered after sheath insertion, and supple- mental doses were then given to maintain an activated clotting time of >300 seconds. All patients in the study underwent balloon predilatation before stenting, and the size of the balloon was determined by the target
vessel size. Either sirolimus-eluting stents (SESs) (Cypher®, Cordis, Johnson & Johnson Corp., Miami, Florida) or paclitaxel-eluting stents (PESs) (Taxus®, Boston Scienti- fic Corp., Natick, Massachusetts) were selected. High- pressure balloon inflation was used in selected cases in an attempt to avoid stent underexpansion. Intravascular ultrasound (IVUS) was used in some cases if necessary.
Procedural myocardial infarction was defined as the pre- sence of new Q waves that were 0.03 seconds in width and/or one-third of the QRS complex in ≥2 contiguous leads and/or ≥3-fold increase in creatine kinase-MB concentration from the upper limit of the normal range.
Angiographic analysis
Coronary angiograms were performed at baseline, immediately after stenting, and after 8 months of follow- up. Two identical orthogonal views were obtained after the intracoronary administration of nitrates, and the images were stored on digital CD-ROM. End-diastolic frames were chosen for quantitative analysis using the computer-based Theoretical Computer Science system, Version 2.02 (Medcon Inc., Tel-Aviv, Israel) by an ope- rator who was unaware of the patients’ information. The average diameter of the normal segments distal and pro- ximal to the treated lesion was used as the reference dia- meter. Minimal lumen diameter (MLD), percentage of stenosis, and lesion length were calculated as the average value of the two orthogonal views. The same views and calibration were used at follow-up angiography. Restenosis was defined as stenosis of >50% of the luminal diameter.
Follow-up
A complete clinical work-up was scheduled at 1 month, 4 months, and 8 months after the procedure, and an- giographic follow-up was scheduled at 8 months post- procedure. All major adverse cardiovascular events (MA- CEs) were determined in-hospital, out-of hospital, and for 240 cumulative days after stent implantation. MACEs, which included all-cause death, myocardial infarction, and the need for repeated target lesion revascularization during the 8-month follow-up period were noted. 12- lead electrocardiography was performed immediately after the procedure and 6, 12, 24 hours following the pro- cedure. Creatine kinase-MB activity was measured at the same time intervals. The end points were defined as cardiac death, myocardial infarction, and the need for repeated revascularization of the target vessel.
Statistical analysis
Data for the continuous variables are expressed as the mean±SD and compared with an unpaired Student’s t-test. Data for the categorical variables are expressed as the number and percentage of patients, and Fisher’s exact test or a chi-square test was used as needed. Multi- variate logistic models were used to identify the predic-
tors of coronary restenosis in the diabetic and nondiabetic patients. Quantitative coronary angiographic parameters were entered as continuous variables into the univa- riate logistic regression. Univariate variables with p<0.20 were entered into the multivariate logistic models. A p of <0.05 was considered significant. Statistical analysis was performed using commercially available software (SPSS 10.0 for Windows, SPSS Inc., Chicago, Illinois).
Results
Patient population
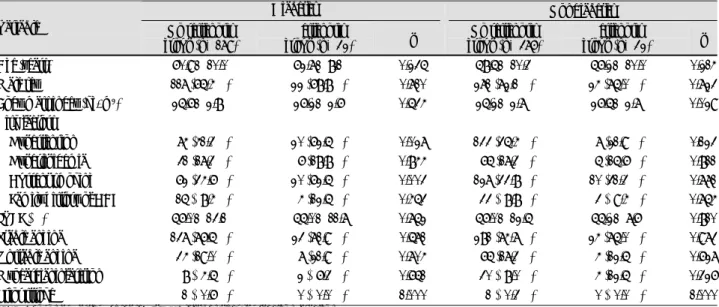
The baseline characteristics of the patients, such as sex, body mass index, hypertension, hyperlipidemia, and smoking status, were similar between the diabetic and nondiabetic patients. Restenosis (>50% of the lum- inal diameter stenosis during the 8 months of follow- up) occurred in 32 (7.8%) of 408 nondiabetic and 32 (15.2%) of 211 diabetic patients (p<0.001). The age and sex of the patients in the Restenosis Group (RG) and
the No Restenosis Group (NRG) were similar in both the diabetic and nondiabetic patients (Table 1). The baseline C-reactive protein (CRP) levels were significantly higher in the RG than in the NRG for both the diabetic and nondiabetic patients (Table 2).
Angiographic characteristics
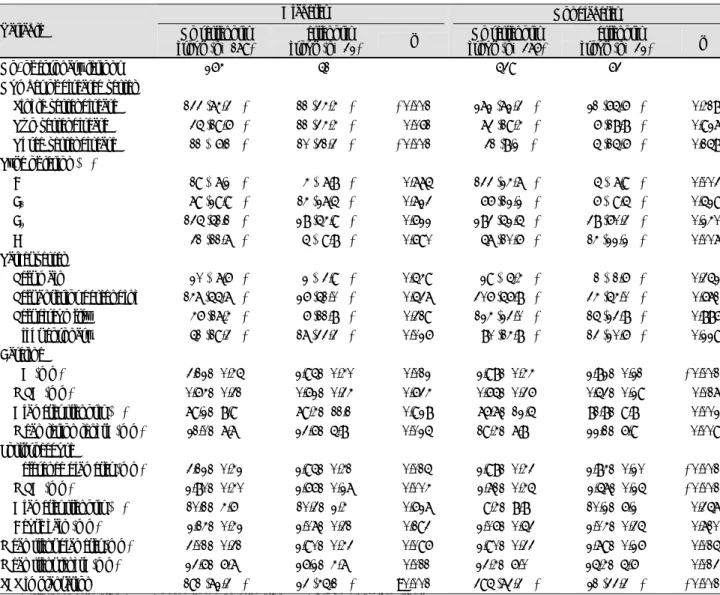
The results of quantitative coronary angiography are listed in Table 3. Lesions were characterized according to the modified American College of Cardiology/Ame- rican Heart Association classification. Postprocedure re- ference diameter and MLD were significantly larger in the NRG than in the RG for both diabetic and non- diabetic patients (Table 3). In the NRG, 191 (72.3%) SESs were used compared with 23 (45.1%) SESs in the RG for diabetic patients (p<0.001)[AH2]. Similar pat- terns were found for nondiabetic patients; 395 (73.3%) SESs were used in the NRG while 21 (33.3%) SESs were used in the RG (p<0.001). Focal type of coronary rest- enosis was observed in 22 lesions (43.1%) in the diabetic
Table 1.Baseline patient characteristics
Diabetes Nondiabetes
Variable No restenosis group (n=179)
Restenosis
group (n=32) p No restenosis group (n=376)
Restenosis
group (n=32) p Age (years) 60.9±10.0 62.7±8.1 0.235 58.5±10.3 56.2±10.0 0.214 Male sex 117 (65.4%) 22 (68.8%) 0.710 271 (72.1%) 24 (75.0%) 0.723 Body mass index (kg/m2) 25.6±2.8 26.2±2.6 0.534 25.2±2.7 26.5±2.7 0.029 Risk factors
Hypertension 074 (41.3%) 20 (62.5%) 0.027 133 (35.4%) 07 (21.9%) 0.123 Hyperlipidemia 031 (17.3%) 06 (18.8%) 0.844 065 (17.3%) 05 (15.6%) 0.811 Current smoking 062 (34.6%) 20 (62.5%) 0.003 127 (33.8%) 10 (31.3%) 0.771 Family history of CAD 015 (08.4%) 04 (12.5%) 0.453 033 (08.8%) 03 (09.4%) 0.754 LVEF (%) 56.0±13.1 55.0±11.7 0.752 56.0±12.5 55.2±7.6 0.810 Stable angina 137 (76.5%) 23 (71.9%) 0.571 281 (74.7%) 24 (75.0%) 0.973 Unstable angina 034 (19.0%) 07 (21.9%) 0.704 065 (17.3%) 04 (12.5%) 0.627 Myocardial infarction 008 (04.5%) 02 (06.3%) 0.651 030 (08.0%) 04 (12.5%) 0.326 Prior stroke 001 (00.6%) 00 (00.0%) 1.000 001 (00.3%) 00 (00.0%) 1.000 CAD: coronary artery disease, LVEF: left ventricular ejection fraction
Table 2.Baseline laboratory variables
Diabetes Nondiabetes
Variable No Restenosis group (n=179)
Restenosis
group (n=32) p No Restenosis group (n=376)
Restenosis
group (n=32) p FBS (mg/dL) 139.6±22.8 142.1±36.3 0.798 100.3±9.9 98.2±11.3 0.387 Uric acid (mg/dL) 5.4±1.5 6.8±1.1 0.030 5.4±1.5 4.8±1.1 0.419 hsCRP (mg/L) 2.0±1.9 4.5±3.2 0.024 2.1±2.0 3.9±3.0 0.019 ESR (mm/hr) 19.4±17.3 25.1±19.5 0.275 18.6±19.8 18.1±13.3 0.941 Creatinine (mg/dL) 1.1±1.1 1.0±0.2 0.555 1.0±0.6 1.0±0.2 0.642 Total cholesterol (mg/dL) 175.1±36.4 184.3±42.8 0.296 187.1±38.4 175.9±38.8 0.238 Triglyceride (mg/dL) 144.2±83.1 128.0±71.6 0.410 145.3±87.8 135.9±50.8 0.665 HDL cholesterol (mg/dL) 39.5±10.8 43.0±9.4 0.163 42.1±12.9 40.1±8.3 0.528 LDL cholesterol (mg/dL) 107.1±34.1 116.2±34.4 0.318 123.3±33.2 112.9±34.9 0.252 FBS: fasting blood sugar, hsCRP: high-sensitive C-reactive protein, ESR: erythrocyte sedimentation rate, HDL: high-density lipoprotein, LDL:
low-density lipoprotein
patients compared with 48 lesions (76.2%) in the nondi- abetic patients (p<0.05). Only 11 diabetic patients (5.2%) and 17 nondiabetic patients (4.2%) underwent IVUS study.
Eight-month clinical outcomes
The rates of deathٛ(p=1.000) and myocardial infarc-
tion (p=0.180) were similar between the two groups of diabetic patients during 8 months of follow-up (Table 4).
However, the rate of myocardial infarction was higher for the nondiabetic patients in the RG (25.0% vs 9.3%, p=0.006) than in the NRG. Late stent thrombosis was observed in one diabetic patient (0.6%) in the NRG
Table 4. Eight-month clinical outcomes
Diabetes Nondiabetes
Variable No restenosis group (n=179)
Restenosis
group (n=32) p No restenosis group (n=376)
Restenosis
group (n=32) p Death (%) 01 (0.6%) 00 (0.0%) <1.000 00 (0.0%) 01 (03.1%) 0.078 Myocardial infarction (%) 07 (3.9%) 03 (9.4%) <0.180 35 (9.3%) 08 (25.0%) 0.006 TVR (%) 23 (12.8%) 16 (50.0%) <0.001 23 (6.1%) 15 (46.9%) <0.001 TVR (Non-TLR) (%) 19 (10.6%) 03 (9.4%) <0.833 17 (4.5%) 01 (03.1%) 1.000 TLR (%) 04 (2.2%) 13 (40.6%) <0.001 06 (1.6%) 14 (43.8%) <0.001
PCI 04 (2.2%) 13 (40.6%) <0.001 06 (1.6%) 14 (43.8%) <0.001
CABG 00 (0.0%) 00 (00.0%) - 00 (0.0%) 00 (00.0%) - Late stent thrombosis (%) 01 (0.6%) 00 (00.0%) <1.000 01 (0.5%) 00 (00.0%) 1.000 TVR: target vessel revascularization, TLR: target lesion revascularization, PCI: percutaneous coronary intervention, CABG: coronary artery bypass graft surgery
Table 3.Results of angiography
Diabetes Nondiabetes
Variable No restenosis group (n=179)
Restenosis
group (n=32) p No restenosis group (n=376)
Restenosis
group (n=32) p
No. of coronary lesions 264 51 539 63
Number of diseased vessel
Single-vessel disease 133 (74.3%) 11 (34.4%) <0.001 272 (72.3%) 21 (65.6%) <0.418 Two-vessel disease 035 (19.6%) 11 (34.4%) <0.061 073 (19.4%) 06 (18.8%) <0.927 Three-vessel disease 011 (06.1%) 10 (31.3%) <0.001 031 (8.2%) 05 (15.6%) <0.158 Type of lesion (%)
A 019 (07.2%) 04 (07.8%) <0.775 133 (24.7%) 05 (07.9%) <0.003
B1 079 (29.9%) 14 (27.5%) <0.723 066 (12.2%) 06 (09.5%) <0.529
B2 135 (51.1%) 28 (54.9%) <0.622 283 (52.5%) 38 (60.3%) <0.240
C 031 (11.7%) 05 (09.8%) <0.690 057 (10.6%) 14 (22.2%) <0.007
Target vessel
Left main 020 (07.6%) 02 (03.9%) <0.549 029 (05.4%) 01 (01.6%) <0.352 Left anterior descending 147 (55.7%) 26 (51.0%) <0.537 306 (56.8%) 34 (54.0%) <0.671 Left circumflex 046 (17.4%) 06 (11.8%) <0.319 124 (23.0%) 15 (23.8%) <0.886 Right coronary 051 (19.3%) 17 (33.3%) <0.026 080 (14.8%) 13 (20.6%) <0.229 Baseline
RD (mm) 3.12±0.45 2.95±0.40 <0.012 2.98±0.44 2.82±0.21 <0.001 MLD (mm) 0.64±0.31 0.62±0.34 <0.634 0.65±0.36 0.53±0.29 <0.017 Diameter stenosis (%) 79.2±8.9 79.4±11.1 <0.928 76.7±12.5 81.8±9.8 <0.002 Mean lesion length (mm) 21.0±7.7 23.6±5.8 <0.025 19.4±7.8 22.1±6.9 <0.009 Postprocedure
Reference diameter (mm) 3.12±0.42 2.95±0.41 <0.015 2.98±0.43 2.84±0.20 <0.001 MLD (mm) 2.80±0.40 2.66±0.27 <0.004 2.71±0.45 2.57±0.25 <0.001 Diameter stenosis (%) 10.1±4.6 10.3±2.4 <0.627 9.4±8.8 10.2±6.2 <0.357 Acute gain (mm) 2.14±0.42 2.07±0.31 <0.193 2.06±0.53 2.04±0.35 <0.710 Mean stent diameter (mm) 3.01±0.31 2.90±0.43 <0.096 2.90±0.33 2.79±0.26 <0.015 Mean stent length (mm) 23.6±6.7 26.2±4.7 <0.011 23.4±6.0 25.4±5.6 <0.013 SES implantation 191 (72.3%) 23 (45.1%) <0.001 395 (73.3%) 21 (33.3%) <0.001 RD: reference diameter, MLD: minimal lumen diameter, SES: sirolimus-eluting stent
and one nondiabetic patient (0.5%) in the NRG.
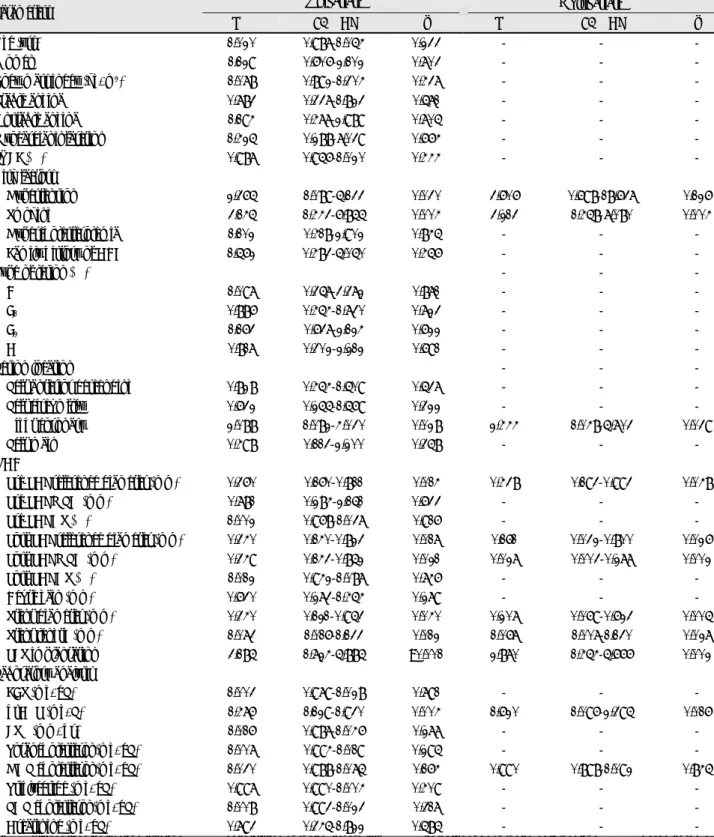
Multivariate analysis for predicting restenosis The multivariate parameters for predicting restenosis in the diabetic group were current smoker, higher CRP,
right coronary lesion, the use of PES, longer stent length, smaller RD before DES implantation, smaller RD after DES implantation and smaller MLD after DES implantation (Table 5). As shown in Table 6, the multivariate parameters for predicting restenosis in the
Table 5.Logistic regression analysis for predicting restenosis in diabetic patients
Univariate Multivariate Parameters
OR 95% CI p OR 95% CI p
Age (yrs) 1.020 0.987-1.054 0.233 - - -
Women 1.129 0.606-2.102 0.703 - - -
Body mass index (kg/m2) 1.078 0.892-1.304 0.437 - - -
Stable angina 0.783 0.337-1.823 0.571 - - -
Unstable angina 1.194 0.477-2.989 0.705 - - -
Myocardial infarction 1.425 0.288-7.039 0.664 - - -
LVEF (%) 0.987 0.956-1.020 0.444 - - -
Risk factors
Hypertension 2.365 1.089-5.133 0.030 3.606 0.698-18.637 0.126 Smoking 3.145 1.443-6.855 0.004 3.213 1.458-7.080 0.004
Hypercholesterolemia 1.102 0.418-2.902 0.845 - - -
Family history of CAD 1.562 0.483-5.050 0.456 - - -
Type of lesion (%) - - -
A 1.097 0.357-3.372 0.871 - - -
B1 0.886 0.454-1.730 0.723 - - -
B2 1.163 0.637-2.124 0.622 - - -
C 0.817 0.302-2.212 0.691 - - -
Lesion location - - -
Left anterior descending 0.828 0.454-1.509 0.537 - - -
Left circumflex 0.632 0.255-1.569 0.322 - - -
Right coronary 2.088 1.082-4.030 0.028 2.444 1.048-5.703 0.039
Left main 0.498 0.113-2.200 0.358 - - -
QCA
Pre-PCI reference diameter (mm) 0.360 0.160-0.811 0.014 0.438 0.193-0.993 0.048
Pre-PCI MLD (mm) 0.781 0.284-2.151 0.633 - - -
Pre-PCI DS (%) 1.002 0.968-1.037 0.916 - - -
Post-PCI reference diameter (mm) 0.340 0.140-0.823 0.017 0.161 0.032-0.800 0.026 Post-PCI MLD (mm) 0.349 0.143-0.852 0.021 0.027 0.003-0.277 0.002
Post-PCI DS (%) 1.012 0.942-1.087 0.746 - - -
Acute gain (mm) 0.630 0.273-1.454 0.279 - - -
Stent diameter (mm) 0.340 0.121-0.953 0.040 0.207 0.069-0.623 0.005 Stent length (mm) 1.073 1.016-1.133 0.012 1.067 1.007-1.130 0.027 PES implantation 3.185 1.724-5.885 <0.001 2.870 1.454-5.666 0.002 Laboratory analysis
FBS (mg/dL) 1.003 0.979-1.028 0.791 - - -
hsCRP (mg/L) 1.476 1.129-1.930 0.004 1.620 1.096-2.395 0.016
ESR (mm/hr) 1.016 0.987-1.046 0.277 - - -
Total cholesterol (mg/dL) 1.007 0.994-1.019 0.295 - - - HDL cholesterol (mg/dL) 1.030 0.988-1.075 0.164 0.990 0.898-1.092 0.845 Triglyceride (mg/dL) 0.997 0.990-1.004 0.409 - - - LDL cholesterol (mg/dL) 1.008 0.993-1.023 0.317 - - -
Creatinine (mg/dL) 0.793 0.345-1.822 0.585 - - -
LVEF: left ventricular ejection fraction, QCA: quantitative coronary angiography, PCI: percutaneous coronary intervention, MLD: minimal lumen diameter, DS: diameter stenosis, PES: paclitaxel-eluting stent, FBS: fasting blood sugar, hsCRP: high-sensitive C-reactive protein, HDL: high- density lipoprotein, LDL: low-density lipoprotein
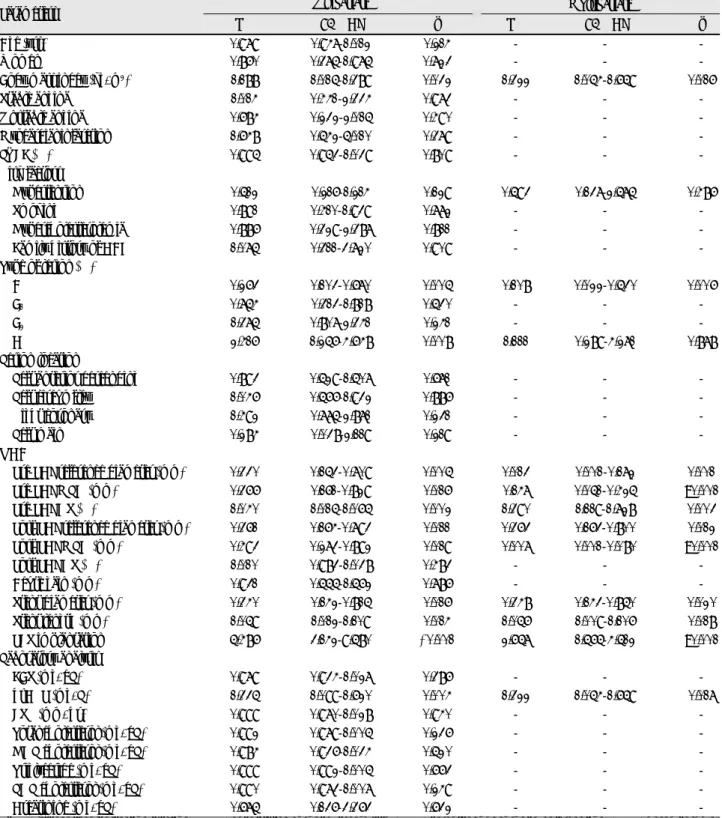
nondiabetic group were body mass index, A-type lesion, higher CRP, the use of PES, longer stent length, sma- ller RD before DES implantation, smaller MLD before DES implantation, smaller RD after DES implantation, and smaller MLD after DES implantation.
Discussion
In the present study, coronary restenosis after DES implantation remained significantly more common in diabetic patients than in nondiabetic patients (15.2%
Table 6.Logistic regression analysis for predicting restenosis in nondiabetic patients
Univariate Multivariate
Parameters
OR 95% CI p OR 95% CI p
Age (yrs) 0.979 0.947-1.012 0.214 - - -
Women 0.860 0.375-1.975 0.723 - - -
Body mass index (kg/m2) 1.188 1.015-1.389 0.032 1.322 1.054-1.659 0.016
Stable angina 1.014 0.441-2.334 0.973 - - -
Unstable angina 0.684 0.232-2.015 0.490 - - -
Myocardial infarction 1.648 0.542-5.010 0.379 - - -
LVEF (%) 0.995 0.953-1.039 0.809 - - -
Risk factors
Hypertension 0.512 0.216-1.214 0.129 0.593 0.137-2.575 0.486
Smoking 0.891 0.410-1.939 0.772 - - -
Hypercholesterolemia 0.886 0.329-2.387 0.811 - - -
Family history of CAD 1.075 0.311-3.720 0.909 - - -
Type of lesion (%)
A 0.263 0.103-0.670 0.005 0.108 0.022-0.530 0.006
B1 0.754 0.313-1.818 0.530 - - -
B2 1.375 0.807-2.341 0.241 - - -
C 2.416 1.256-4.648 0.008 1.111 0.289-4.271 0.878
Lesion location
Left anterior descending 0.893 0.529-1.507 0.671 - - -
Left circumflex 1.046 0.566-1.932 0.886 - - -
Right coronary 1.492 0.775-2.871 0.231 - - -
Left main 0.284 0.038-2.119 0.219 - - -
QCA
Pre-PCI reference diameter (mm) 0.330 0.153-0.709 0.005 0.013 0.001-0.172 0.001 Pre-PCI MLD (mm) 0.366 0.161-0.829 0.016 0.147 0.051-0.425 <0.001 Pre-PCI DS (%) 1.040 1.015-1.065 0.002 1.390 1.119-1.728 0.003 Post-PCI reference diameter (mm) 0.361 0.164-0.793 0.011 0.363 0.163-0.800 0.012 Post-PCI MLD (mm) 0.493 0.273-0.892 0.019 0.007 0.001-0.080 <0.001
Post-PCI DS (%) 1.010 0.983-1.038 0.483 - - -
Acute gain (mm) 0.931 0.555-1.562 0.786 - - -
Stent diameter (mm) 0.340 0.142-0.815 0.016 0.348 0.143-0.850 0.020 Stent length (mm) 1.059 1.012-1.109 0.014 1.056 1.009-1.106 0.018 PES implantation 5.486 3.142-9.580 <0.001 2.657 1.565-4.512 <0.001
Laboratory analysis
FBS (mg/dL) 0.979 0.934-1.027 0.386 - - -
hsCRP (mg/L) 1.335 1.099-1.620 0.004 1.322 1.054-1.659 0.017
ESR (mm/hr) 0.999 0.970-1.028 0.940 - - -
Total cholesterol (mg/dL) 0.992 0.979-1.005 0.236 - - -
HDL cholesterol (mg/dL) 0.984 0.936-1.034 0.520 - - -
Triglyceride (mg/dL) 0.999 0.992-1.005 0.663 - - -
LDL cholesterol (mg/dL) 0.990 0.973-1.007 0.249 - - -
Creatinine (mg/dL) 0.675 0.136-3.363 0.632 - - -
LVEF: left ventricular ejection fraction, QCA: quantitative coronary angiography, PCI: percutaneous coronary intervention, MLD: minimal lumen diameter, DS: diameter stenosis, PES: paclitaxel-eluting stent, FBS: fasting blood sugar, hsCRP: high-sensitive C-reactive protein, HDL: high- density lipoprotein, LDL: low-density lipoprotein ٛ
of restenosis in diabetic patients vs 7.8% in nondiabetic patients). To the best of our knowledge, no study has ever compared the clinical and angiographic parameters of coronary restenosis in diabetic and nondiabetic pat- ients after DES implantation. Small baseline and post- PCI vessel size, longer stent length, the use of PESs, cur- rent smokers, right coronary lesions, and high levels of CRP were significant predictors of coronary restenosis in diabetic patients after DES implantation. Moreover, small baseline and post-PCI vessel size, longer stent length, the use of PESs, higher body mass index, and high level of CRP were significant predictors of res- tenosis in nondiabetic patients. The high level of CRP, a small baseline and post-PCI vessel size, and longer stent length remained significant predictors of res- tenosis in both the diabetic and nondiabetic patients, even in the era of DES implantation. In the present study, the use of PESs was associated with an increased rate of restenosis in both diabetic (OR=2.870, 95% CI 1.454 to 5.666, p=0.002) and nondiabetic patients (OR=2.657, 95% CI 1.565 to 4.512, p<0.001). Alth- ough DES implantation was found to improve the an- giographic and clinical outcomes in both diabetic and nondiabetic patients when compared with BMS impl- antation, the angiographic predictors of restenosis after DES implantation seemed to be similar to the predi- ctors of restenosis after BMS implantation in both dia- betic and nondiabetic patients.
Coronary restenosis results from neointimal hyper- plasia, which causes late luminal loss. New devices, such as DESs, can be used to reduce the rate of restenosis by decreasing the late luminal loss. The introduction of DES implantation has significantly overcome the major limitation of BMS implantation by reducing the rates of coronary restenosis. Many studies have shown that the blockage of smooth muscle cell proliferation with DESs results in the preservation of the normal vessel phenotype and function, thereby decreasing the rate of neointimal hyperplasia and coronary restenosis.12-15) Many now regard paclitaxel and sirolimuseluting stents to be the standard mode of treatment for patients undergoing PCI. The identification of the parameters of coronary restenosis after DES implantation is im- portant since angiographic outcomes can be predicted from the baseline clinical and angiographic parameters.
Moreover, modifiable risk factors, such as smoking sta- tus, in the present study could be adjusted to reduce the rate of restenosis, and patients with multiple pre- dictors of coronary restenosis could be considered for other treatment options, such as coronary bypass sur- gery. Even though DES implantation lowers the rates of restenosis by preventing smoothmuscle cell prolifera- tion at the stented site, atherosclerosis could progress at other coronary sites. Therefore, combined approaches using systemic therapies, such as HMG (3-hydroxy-3-
methylglutaryl)-CoA reductase inhibitors and peroxi- some proliferator-activated receptor (PPAR)-γ activators, are required to prevent neointimal proliferation and to prevent the progression of atherosclerosis at other cor- onary sites.
Although the total percentage of patients with res- tenosis after DES implantation has decreased compared with that after BMS implantation, various predictors of restenosis with DESs overlap with those associated with BMSs.16-20) Notably, the angiographic parameters of restenosis in the diabetic and nondiabetic patients were similar, even after DES implantation. Since coro- nary restenosis was mainly the result of neointimal hyperplasia, binary restenosis was more likely to occur in patients with small baseline and post-PCI vessel diameters. Pre-and post-PCI small vessel size and longer stent length were the major angiographic predictors of restenosis, regardless of the presence of diabetes, even in the era of DES implantation. In the present study, a high level of CRP and the use of PESs were found to be associated with coronary restenosis in both diabetic and nondiabetic patients. Patients with unfavorable ba- seline angiographic parameters should be treated with aggressive adjunctive systemic pharmacotherapy to mo- dify the underlying pathophysiological mechanisms res- ponsible for neointimal formation and the progression of atherosclerosis, even in the era of DESs.
This study has the inherent limitations of every obs- ervational, nonrandomized study. It is pertinent to note that the findings of this study are based on a relatively short-term retrospective study. Moreover, the number of study participants was relatively small, and therefore we may not be able to generalize our results to all pat- ients with DESs. The present study demonstrated the associations between various clinical and angiographic parameters and coronary restenosis; however, the causes and effects of these associations were not completely verified. IVUS studies were performed only on selected patients; therefore, it is possible that stent underex- pansion and short lesion coverage may have occurred.
Unexpectedly, A-type lesions were a predictor of res- tenosis in nondiabetic patients, and this finding might be due to the short lesion coverage and stent under- expansion by inexperienced operators. A larger pro- spective randomized clinical trial is warranted to con- firm the various predictors of coronary restenosis after DES implantation.
In conclusion, although DES implantation was found to improve the angiographic and clinical out-comes in both diabetic and nondiabetic patients when com- pared with BMS implantation, coronary restenosis after DES implantation remained significantly more com- mon in diabetic patients than in nondiabetic patients.
The use of PESs, a high level of CRP, small base-line and post-PCI reference diameter, and longer stent leng-
th remained significant predictors of restenosis in both the diabetic and nondiabetic patients, even in the era of DES implantation. The identification of patients with the predictors of coronary restenosis after DES im- plantation may aid in the alteration of the modifiable predictors of restenosis, the application of more aggre- ssive risk factor management, and in helping interven- tionists to know when to consider other treatment mo- dalities, such as coronary artery bypass graft surgery.
Acknowledgments
The authors express their sincere gratitude to the study parti-
cipants and greatly appreciate Hae Joo Kim, Jun Won Kang, and Youn Won Lee for their excellent assistance. There is no conflict of interest in connection with any commercial associations, and all authors have nothing to disclose.
This study was supported by the Korea University Research Grant K0518341 of 2005 and R0600701.
REFERENCES
1) Mathew V, Gersh BJ, Williams BA, et al. Outcomes in patients with diabetes mellitus undergoing percutaneous coronary inter- vention in the current era. Circulation 2004;109:476-80.
2) Elezi S, Kastrati A, Pache J, et al. Diabetes mellitus and the cli- nical and angiographic outcome after coronary stent placement.
J Am Coll Cardiol 1998;32:1866-73.
3) Carrozza JP Jr, Kuntz RE, Fishman RF, Baim DS. Restenosis after arterial injury caused by coronary stenting in patients with diabetes mellitus. Ann Intern Med 1993;118:344-9.
4) Stone GW, Ellis SG, Cox DA, et al. A polymer-based, paclitaxel- eluting stent in patients with coronary artery disease. N Engl J Med 2004;350:221-31.
5) Grube E, Silber S, Hauptmann KE, et al. Six- and twelve-month results from a randomized, double-blind trial on a slow-release paclitaxel-eluting stent for de novo coronary lesions. Circulation 2003;107:38-42.
6) Moses JW, Leon MB, Popma JJ, et al. Sirolimus-eluting stents versus standard stents in patients with stenosis in a native coronary artery. N Engl J Med 2003;349:1315-23.
7) Holmes DR Jr, Leon MB, Moses JW, et al. Analysis of 1-year
clinical outcomes in the SIRIUS trial: a randomized trial of a sirolimus-eluting stent versus a standard stent in patients at high risk for coronary restenosis. Circulation 2004;109:634-40.
8) Gaspardone A, Versaci F, Tomai F, et al. C-reactive protein, clin- ical outcome, and restenosis rates after implantation of different drug-eluting stents. Am J Cardiol 2006;97:1311-6.
9) Kuchulakanti PK, Torguson R, Canos D, et al. Impact of treatment of coronary artery disease with sirolimus-eluting stents on out- comes of diabetic and nondiabetic patients. Am J Cardiol 2005;
96:1100-6.
10) Hermiller JB, Raizner A, Cannon L, et al. Outcomes with the polymer-based paclitaxel-eluting TAXUS stent in patients with diabetes mellitus: the TAXUS-IV trial. J Am Coll Cardiol 2005;
45:1172-9.
11) Moussa I, Leon MB, Baim DS, et al. Impact of sirolimus-eluting stents on outcome in diabetic patients. Circulation 2004;109:
2273-8.
12) Lim DS. Coronary restenosis after drug-eluting stent implanta- tion in diabetic patients. Korean Circ J 2006;36:1-7.
13) Leon MB, Bakhai A. Drug-eluting stents and glycoprotein Iib/
IIIa inhibitors: combination therapy for the future. Am Heart J 2003;146:S13-7.
14) Bennett MR. In-stent stenosis: pathology and implications for the development of drug eluting stents. Heart 2003;89:218-24.
15) Fattori R, Piva T. Drug-eluting stents in vascular intervention.
Lancet 2003;361:247-9.
16) Lee CW, Park SJ. Predictive factors for restenosis after drug-elu- ting stent implantation. Korean Circ J 2007;37:97-102.
17) Mercado N, Boersma E, Wijns W, et al. Clinical and quantitative coronary angiographic predictors of coronary restenosis: a com- parative analysis from the balloon-to-stent era. J Am Coll Cardiol 2001;38:645-52.
18) Kim BK, Oh SJ, Jeon DW, et al. Clinical outcomes following sirolimus-eluting stent implantation in patients with end-stage renal disease. Korean Circ J 2006;36:424-30.
19) West NE, Ruygrok PN, Disco CM, et al. Clinical and angiogr- aphic predictors of restenosis after stent deployment in diabetic patients. Circulation 2004;109:867-73.
20) Mazeika P, Prasad N, Bui S, Seidelin PH. Predictors of angio- graphic restenosis after coronary intervention in patients with diabetes mellitus. Am Heart J 2003;145:1013-21.