The First Korean Case of Nontuberculous Mycobacterial Lung Disease Caused by
Mycobacterium abscessus Subspecies bolletii in a Patient with Bronchiectasis
Byeong-Ho Jeong, M.D.
1,*, Su-Young Kim, Ph.D.
1,*, Kyeongman Jeon, M.D.
1, Hee Jae Huh, M.D.
2, Chang-Seok Ki, M.D.
2, Nam Yong Lee, M.D.
2, Sung Jae Shin, Ph.D.
3and Won-Jung Koh, M.D.
11
Division of Pulmonary and Critical Care Medicine, Department of Medicine,
2Department of Laboratory Medicine and Genetics, Samsung Medical Center, Sungkyunkwan University School of Medicine,
3Department of Microbiology, Yonsei University College of Medicine, Seoul, Korea
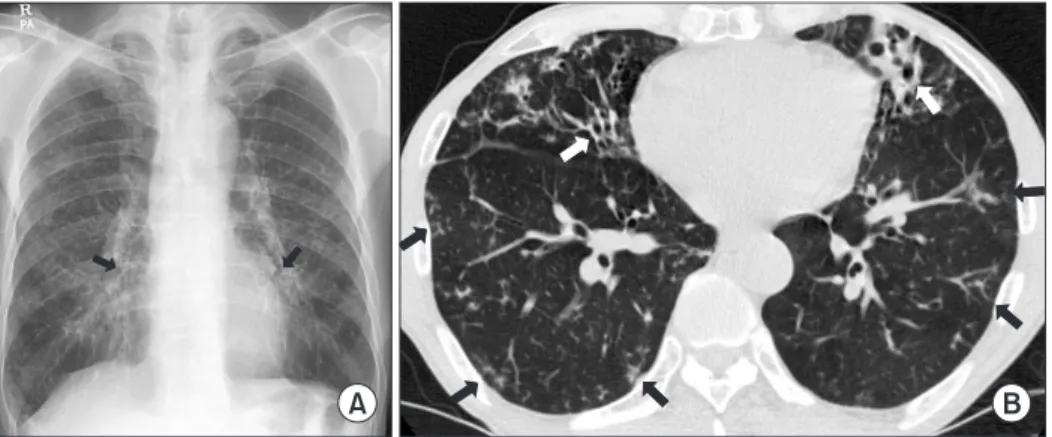
We report the first Korean case of lung diseases caused by Mycobacterium abscessus subsp. bolletii in a previously healthy male, except for a previous history of pulmonary tuberculosis and bronchiectasis. All serial isolates are identified as M. abscessus subsp. bolletii by multi-locus sequence analysis based on the hsp65, rpoB, and 16S rRNA fragments. At the genetic level, the isolate has the erm(41) gene with a T28 sequevar, associated with clarithromycin resistance, and no rrl mutation. The isolate is resistant to clarithromycin. Although the symptoms and radiographic findings have improved after combination of antibiotics, the follow-up sputum cultures are persistently positive.
Keywords: Bronchiectasis; Mycobacterium Infections, Nontuberculous; Nontuberculous Mycobacteria; Sequence Analysis, DNA
mycobacteria (NTM) in Korea
1. Of the RGM species, Myco- bacterium abscessus complex is most commonly associated with NTM lung disease. Although subspeciation of M. absces- sus complex is still controversial, M. abscessus complex is currently divided into three subspecies: M. abscessus subsp.
abscessus, M. abscessus subsp. massiliense and M. abscessus subsp. bolletii
2.
In Korea, M. abscessus subsp. bolletii is identified in only 1.3−1.6% of clinical strains of M. abscessus complex
3. Although a case with disseminated infection of M. abscessus subsp.
bolletii was reported
4, there has been no report of NTM lung disease caused by M. abscessus subsp. bolletii in Korea. Here, we describe a case of chronic pulmonary disease caused by M.
abscessus subsp. bolletii.
Case Report
A 66-year-old male was referred to our hospital for manage- ment of probable NTM lung disease. He was an ex-smoker and had a history of previous treatment for pulmonary tuber- Copyright © 2014
The Korean Academy of Tuberculosis and Respiratory Diseases.
All rights reserved.
Introduction
Rapidly growing mycobacteria (RGM) are relatively com- mon pathogens of lung disease caused by nontuberculous
CASE REPORT
http://dx.doi.org/10.4046/trd.2014.76.1.30ISSN: 1738-3536(Print)/2005-6184(Online) • Tuberc Respir Dis 2014;76:30-33
30
Address for correspondence: Won-Jung Koh, M.D.
Division of Pulmonary and Critical Care Medicine, Department of Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, 81 Irwon-ro, Gangnam-gu, Seoul 135-710, Korea
Phone: 82-2-3410-3429, Fax: 82-2-3410-3849 E-mail: [email protected]
*Byeong-Ho Jeong and Su-Young Kim contributed equally to this work.
Received: Aug. 7, 2013 Revised: Sep. 4, 2013 Accepted: Sep. 16, 2013
cc