Interleukin-17 in Various Ocular Surface Inflammatory Diseases
Recently, the association of Th-17 cells or IL-17 with ocular inflammatory diseases such as uveitis, scleritis and dry eye syndrome was discovered. We assessed whether interleukin (IL)-17 was present in the tears of various ocular surface inflammatory diseases and the tear IL-17 concentrations were clinically correlated with various ocular surface inflammatory diseases. We measured concentrations of IL-17 in tears of normal subjects (n = 28) and patients (n = 141) with meibomian gland dysfunction (MGD), dry eye syndrome (DES), Sjögren syndrome (SS), Stevens-Johnson syndrome (SJS), graft-versus-host disease (GVHD), filamentary keratitis, and autoimmune keratitis associated with rheumatoid arthritis or systemic lupus erythematosus. Clinical epitheliopathy scores were based on the surface area of corneal and conjunctival fluorescein staining. The mean concentrations of IL-17 in tears of patients with filamentary keratitis, GVHD, autoimmune keratitis, SS, DES, MGD, SJS were significantly higher in order than that in normal subjects. Tear IL-17 concentration was significantly correlated with clinical epitheilopathy scores in the patients with systemic inflammatory disease, while tear IL-17 was not correlated with clinical severity of the cornea and conjunctiva in the dry eye patients without any systemic inflammatory disease.
Tear IL-17 is likely to correlate clinically with corneal disease severity only in the patients with systemic inflammatory disease.
Key Words: Interluekin-17; Tears; Ocular Surface Inflammatory Diseases; Epitheliopathy Score
Min Ho Kang1,2, Mee Kum Kim2,3, Hyun Joo Lee2, Hyeon Il Lee4, Won Ryang Wee2,3 and Jin Hak Lee2,3
1Department of Ophthalmology, Hanyang University Guri Hospital, Guri; 2Seoul Artificial Eye Center, Seoul National University Hospital Clinical Research Institute, Seoul; 3Department of Ophthalmology, Seoul National University College of Medicine, Seoul; 4GM Eye Clinic, Seoul, Korea
Received: 18 August 2010 Accepted: 27 April 2011 Address for Correspondence:
Mee Kum Kim, MD
Department of Ophthalmology, Seoul National University Hospital, 101 Daehak-ro, Jongno-gu, Seoul 110-744, Korea Tel: +82.2-2072-2438, Fax: +82.2-741-3187 E-mail: [email protected]
This research was supported by Grant from the Seoul National University Hospital Research Fund (Number 03-2008-0220).
DOI: 10.3346/jkms.2011.26.7.938 • J Korean Med Sci 2011; 26: 938-944
INTRODUCTION
Since a distinct T cell subset, known as T helper type 17 lympho- cyte (Th-17), which is characterized by the production of inter- leukin (IL)-17 has been identified (1, 2), compelling evidence has accumulated that Th-17 cells are involved in a wide variety of autoimmune (3-8) and allergic diseases (9) and transplanta- tion rejection (10). Recent studies have indicated that Th-17 cells are involved in psoriasis (3), rheumatoid arthritis (RA) (4), mul- tiple sclerosis (MS) (5), inflammatory bowel disease (IBD) (6), systemic lupus erythematosus (SLE) (7) and asthma (9), through the IL-17/IL-23 axis.
Currently, the association of Th-17 cells or IL-17 with ocular inflammatory diseases such as uveitis (11, 12) and scleritis (12), as well as dry eye syndrome (13, 14), has also been revealed. In addition, Th-17 cells have been found to play an important role in early herpes virus-induced corneal inflammation (15).
IL-17, which is mainly produced by Th-17 cells, mediates pow- erful effects on stromal cells, resulting in production of inflam- matory cytokines and recruitment of leukocytes, especially neu- trophils, thus creating a link between innate and adaptive im- munity (2). The IL-17 associated modulation of stromal cells may have an affect on conjunctival and corneal wound healing
in various ocular surface inflammatory diseases, leading to epi- thelial erosion, which the clinician assesses for clinical scoring and disease severity.
For this study, we hypothesized that Th-17 cells might be in- volved to different degrees not only in autoimmune ocular sur- face disease but also in nonautoimmune ocular surface disease.
We also presumed that the involvement of Th-17 cells could be correlated with clinical scores of ocular surfaces, which repre- sent disease severity. Therefore, we aimed to quantify IL-17 in the tears of various ocular surface inflammatory diseases, and to assess whether there were clinical correlations of tear IL-17 concentration with various ocular surface inflammatory dis- eases.
MATERIALS AND METHODS Subjects
Patients visiting the outpatient clinic of Seoul National Univer- sity Hospital between March and October 2009, and who pre- sented with various ocular surface diseases, were enrolled (n = 142). Normal subjects without any ocular problems and system- ic diseases voluntarily participated as controls (n = 28). Ocular surface disease was diagnosed by an ophthalmologist.
The included ocular surface diseases were as follows: meibo- mian gland dysfunction (MGD, n = 51), dry eye syndrome with- out any systemic disease and meibomian gland dysfunction (DES, n = 38), Sjögren syndrome (SS, n = 33), chronic limbal de- ficiency secondary to Stevens-Johnson syndrome (SJS, n = 5), DES with rheumatoid arthritis (RA) or systemic lupus erythe- matosus (SLE, n = 4), graft-versus-host disease (GVHD, n = 7), and filamentary keratitis (n = 3). Patients taking oral or topical steroids or topical cyclosporine eye drops within one month before enrollment were excluded.
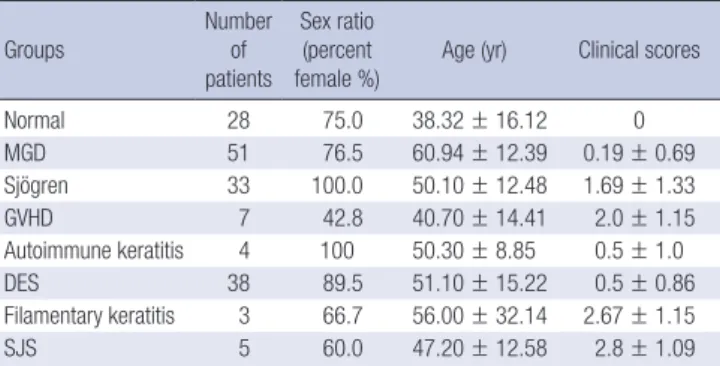
Patient characteristics are summarized in Table 1. There were 141 patients (23 males) included in the study, with a mean age of 52.6 yr.
The patients were divided into two groups; subjects without systemic inflammatory disease (group A) and the others with systemic inflammatory disease (group B). Group A included simple dry eye, MGD and filamentary keratitis, while group B included GVHD, SS, SJS, dry eye with RA or SLE. Tear IL-17 con- centration were compared among the disease in each group, and the correlation of tear IL-17 with clinical severity of the cornea
were analyzed in each group.
Measurement of tear IL-17 concentrations
A previously reported protocol was followed for sampling tears (16). Topical anesthetics was not used to avoid diluting effect before collecting tear. To avoid reflex tearing, Schirmer strip was carefully placed not to irritate conjunctival surface as possible as we could. Tears were collected for 5 min by the Schirmer I meth- od using filter paper (Color Bar Schirmer Tear Test standardized sterile strips, Eagle Vision, Inc., Memphis, TN, USA) in the same exam room to minimize the effect of ambient humidity. After collection, each Schirmer strip was stored at -20°C until use. For evaluation, each Schirmer strip was thawed and the tear volume was calculated by converting 1 mm of tear-moistened Schirmer strip to 1 μL of tear volume (16). The strip was eluted at room temperature overnight with a final volume of 0.05 M phosphate- buffered solution (PBS, pH 7.2) containing 0.5 M NaCl, and 0.5%
Tween 20, such that the tear sample was diluted to 40-fold.
Tear concentrations of IL-17A were measured using a com- mercially-available enzyme-linked immunosorbent assay (ELI- SA) kit (Human IL-17 DuoSet; R&D Systems, Minneapolis, MN, USA) according to manufacturer instructions. ELISAs were per- formed in triplicate to ensure the reproducibility of the data.
According to the manufacturer, the assay’s lower limit of detec- tion was 15 pg/mL.
Clinical scoring of ocular surface epitheliopathy
Clinical scoring was based on the area of corneal and conjunc- tival fluorescein staining (17), and was modified according to the protocol of the study clinic. One drop of 2% sterile fluores- cein was instilled into each conjunctival sac, and after the pa- tient blinked several times, corneal and conjunctival staining were scored as quickly as possible. There were 3 corneal regions (upper, middle, and lower) and 4 conjunctival regions (superi- Table 1. Demographic characteristics of study subjects
Groups
Number of patients
Sex ratio (percent
female %) Age (yr) Clinical scores
Normal 28 75.0 38.32 ± 16.12 0
MGD 51 76.5 60.94 ± 12.39 0.19 ± 0.69
Sjögren 33 100.0 50.10 ± 12.48 1.69 ± 1.33
GVHD 7 42.8 40.70 ± 14.41 2.0 ± 1.15
Autoimmune keratitis 4 100 50.30 ± 8.85 0.5 ± 1.0
DES 38 89.5 51.10 ± 15.22 0.5 ± 0.86
Filamentary keratitis 3 66.7 56.00 ± 32.14 2.67 ± 1.15
SJS 5 60.0 47.20 ± 12.58 2.8 ± 1.09
MGD, meibomian gland dysfunction; Sjögren, Sjögren syndrome; GVHD, graft-versus host disease; Autoimmune keratitis, dry eye syndrome with Rheumatic arthritis or Systemic lupus erythematosus; DES, dry eye syndrome without systemic disease;
SJS, Stevens-Johnson syndrome.
A B C D
E F G H
Fig. 1. Photograph standards and diagram for clinical scoring of corneal and conjunctival staining, with fewer modifications. Corneal staining standards; (A, B) and (C) each are 1 point; (D) and (E) each are 2 points; (F) and (G) each are 3 points. (H) Diagram: fluorescein staining was recorded in upper, middle and lower corneal regions; and superior, inferior, nasal, and temporal conjunctival regions.
or, inferior, nasal, and temporal) evaluated (Fig. 1). A maximum of 3 points was used for corneal fluorescein staining as follows:
0 point for no punctuate staining of the cornea; 1 point for cor- neal epithelial staining in 1 region or less, 2 points for 2 regions or less, but more than 1 region, 3 points for more than 2 regions (Fig. 1).
A maximum of 3 points was also used for conjunctival fluo- rescein staining as follows: 0 point for no punctuate staining of the conjunctiva; 1 point for conjunctival staining in 1 quadrant or less, 2 points for 2 quadrants, and 3 points for 3 or more quad- rants of conjunctival staining. Clinical scores were calculated by adding the corneal and conjunctival scores, with a maximum score of 6 points (18).
Statistical analysis
To compare the mean IL-17 concentration in tears of normal subjects with the mean concentrations in tears of the disease groups, a nonparametric statistical test (Mann-Whitney U test) was used. The Pearson correlation analysis test was used to as- sess the relationship between clinical scores and IL-17 concen- trations in tears. For all tests, P < 0.05 was considered to be sig- nificant.
Ethics statement
This study was approved by the institutional review board of Seoul National University Hospital (H-0803-029-238). All sub- jects signed informed consent forms for participation in this study.
RESULTS
The demographics of the patients were shown in Table 1. The score in corneal severity were higher in SJS, filamentary kerati- tis, GVHD and SS in order (Table 1).
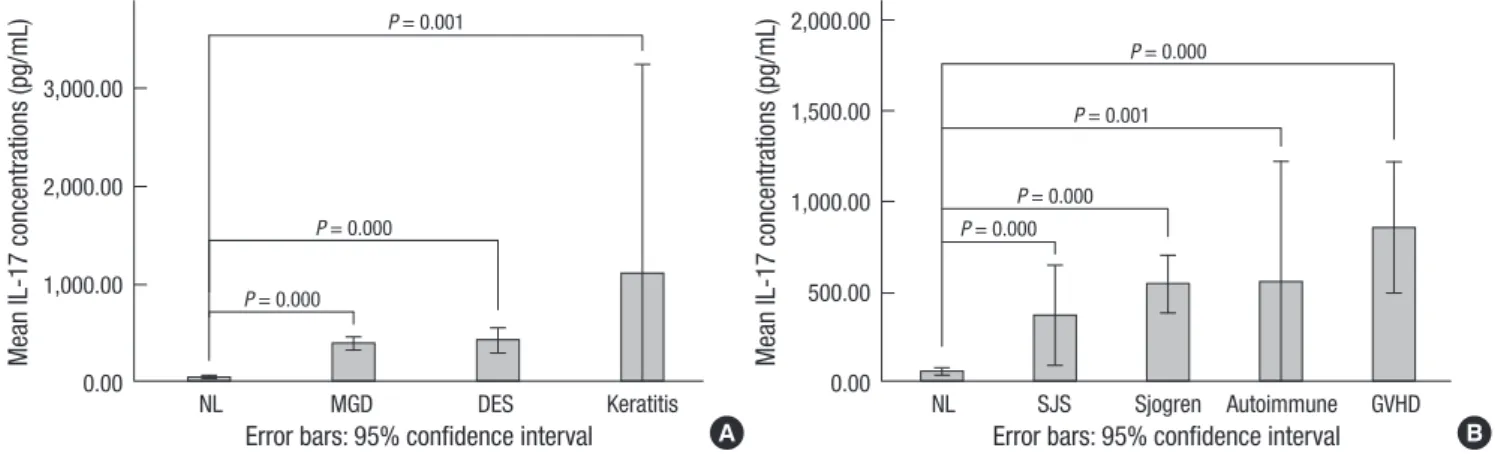
An aim of this study was to evaluate whether IL-17 is involved in various ocular surface inflammations. Surprisingly, most oc- ular surface diseases, including not only autoimmune-associ- ated keratitis but also non-autoimmune surface inflammation, showed increased tear IL-17 concentrations, suggesting possi- ble involvement of Th-17 cells. The mean concentrations of tear IL-17A in patients with GVHD, SS, autoimmune keratitis, MGD, DES, and filamentary keratitis were significantly higher than the mean concentration of IL-17A in normal subjects (Table 2 and Fig. 2, P < 0.05, Mann-Whitney U test). The mean concentration of tear IL-17A was highest in filamentary keratitis, followed in
Table 2. The concentrations of the tear IL-17 in the various ocular surface diseases (pg/mL)
Groups Mean Standard deviation Minimum Maximum Median
Normal 45.35 57.46 15.00 200.20 15.00
MGD 389.98 244.92 35.71 969.06 336.65
Sjögren 530.43 446.32 35.44 2,162.27 418.27
GVHD 845.23 391.11 222.08 1,455.10 908.22
Autoimmune keratitis 542.31 421.24 124.05 1,122.14 525.32
DES 422.98 389.77 39.76 1,740.43 279.78
Filamentary keratitis 1,102.04 859.71 232.78 1,998.70 1,022.63
SJS 356.79 223.74 141.99 728.16 328.89
MGD, meibomian gland dysfunction; Sjögren, Sjögren syndrome; GVHD, graft-versus host disease; Autoimmune keratitis, dry eye syndrome with Rheumatic arthritis or Systemic lupus erythematosus; DES, dry eye syndrome without systemic disease; SJS, Stevens-Johnson syndrome.
Mean IL-17 concentrations (pg/mL) Mean IL-17 concentrations (pg/mL)
NL MGD DES Keratitis NL SJS Sjogren Autoimmune GVHD
3,000.00
2,000.00
1,000.00
0.00
2,000.00 1,500.00 1,000.00 500.00
0.00
A B
P = 0.000 P = 0.000
P = 0.001
P = 0.000
P = 0.001
P = 0.000 P = 0.000
Error bars: 95% confidence interval Error bars: 95% confidence interval
Fig. 2. Mean values of IL-17 concentrations in tears of each patient group compared to the normal control group. The patients were divided into two groups; subjects without systemic inflammatory disease (A, group A) and the others with systemic inflammatory disease (B, group B). In all groups, the mean concentrations of IL-17 were significantly higher than that of the normal group (Mann-Whitney U test). NL, normal control; MGD, meibomian gland dysfunction; Sjogren, Sjögren syndrome; GVHD, graft-versus host dis- ease; Autoimmune, dry eye syndrome associated with rheumatoid arthritis or systemic lupus erythematosus; DES, dry eye syndrome without systemic disease; SJS, Stevens- Johnson syndrome; Keratitis, filamentary keratitis.
order of decreasing concentrations by GVHD, autoimmune ker- atitis, SS, DES, MGD and SJS. Interestingly, the mean concen- tration of IL-17A in GVHD patients was higher than in DES, SJS and SS patients (P = 0.007, 0.032, and 0.031, Mann-Whitney U test, Fig. 3).
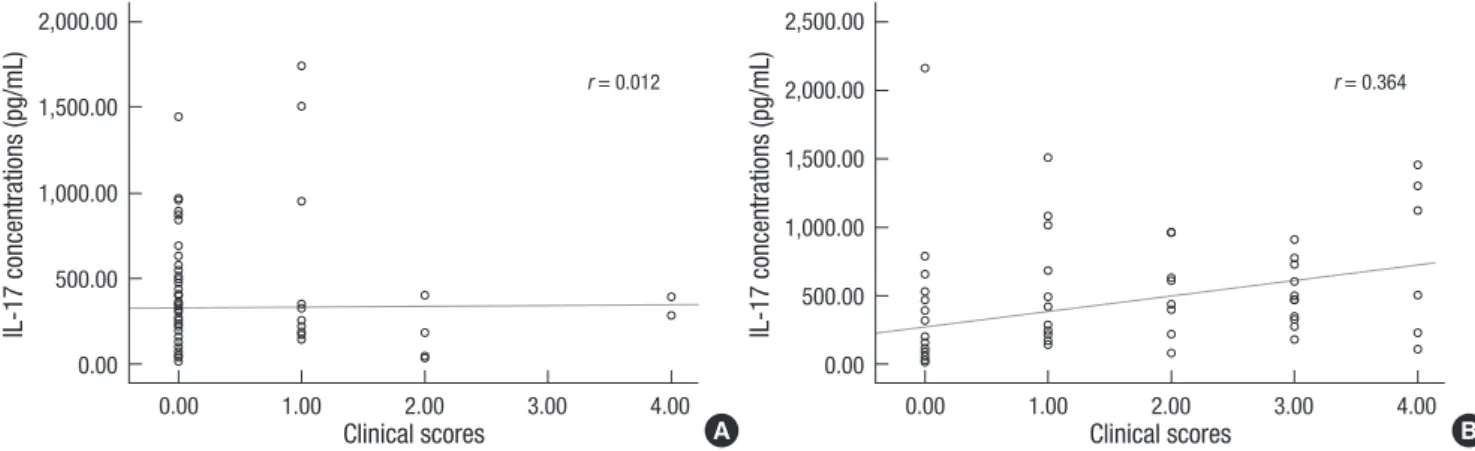
While, correlates tear IL-17 concentrations with clinical scores of ocular surface inflammation, it could provide clinically rele- vant information. As shown in Fig. 4, tear IL-17 concentrations significantly correlated with clinical scores in patients with sys- temic inflammatory disease, (Pearson correlation coefficient [r] = 0.364, P = 0.022, Pearson correlation analysis test) on the contrary, tear IL-17 did not correlate with the clinical severity in the dry eye patients without any systemic inflammatory disease (Pear- son correlation coefficient [r] = 0.012, P = 0.901, Pearson corre- lation analysis test) although high tear IL-17 was shown in these patients. To rule out age as a confounding factor, age was ana- lyzed in relation to tear IL-17 concentrations, and there was no
significant correlation (Pearson correlation coefficient [r] = -0.037, P = 0.637, Pearson correlation analysis test, Fig. 5). It suggested that tear IL-17 is likely to be clinically involved in corneal inflam- mation in the patients with systemic inflammatory disease.
DISCUSSION
The demonstration of IL-17 involvement in various ocular sur- face diseases is supporting evidence for recent reports (13, 19) showing that Th-17 cells are important in the pathogenesis of ocular surface diseases. We demonstrated in this study that ele- vated tear IL-17 levels were seen in not only autoimmune-asso- ciated but also non-autoimmune-associated ocular surface dis- eases, including meibomian gland disease and dry eye syndrome.
However, the concentrations of IL-17 correlated well with clini- cal scoring of epitheliopathy only in the patients with systemic inflammatory disease, indicating that tear IL-17 expression lev- els can provide clinically-relevant information on corneal dis- ease severity in the patients with systemic autoimmune disease and systemic inflammatory disease like GVHD.
Fig. 3. Mean values of IL-17 concentrations in tears of each patient group compared to the Graft-versus-host disease patients. The mean IL-17 concentration of graft-ver- sus-host disease patients was significantly higher than those of dry eye syndrome without systemic disease patients, Stevens-Johnson syndrome and Sjögren syndrome patients (Mann-Whitney U test). GVHD, graft-versus-host disease; DES, dry eye syn- drome without systemic disease; SJS, Stevens-Johnson syndrome; Sjogren, Sjögren syndrome.
Mean IL-17 concentrations (pg/mL)
GVHD DES SJS Sjogren
2,000.00 1,500.00 1,000.00 500.00 0.00
P = 0.031
P = 0.032 P = 0.007
Error bars: 95% confidence interval
IL-17 concentrations (pg/mL) IL-17 concentrations (pg/mL)
0.00 1.00 2.00 3.00 4.00 0.00 1.00 2.00 3.00 4.00
2,000.00 1,500.00 1,000.00 500.00 0.00
2,500.00 2,000.00 1,500.00 1,000.00 500.00 0.00
A B
Clinical scores Clinical scores
r = 0.012 r = 0.364
Fig. 4. Correlation of tear IL-17 concentrations with clinical scores. There was no correlation of tear IL-17 with clinical scores in subjects the dry eye patients without systemic disease (group A; (A) Pearson correlation coefficient [r ] = 0.012, P = 0.901) while, tear IL-17 did correlate a statistically significantly positive correlation with clinical severity in the patients with systemic diseases (group B; (B) Pearson correlation coefficient [r ] = 0.364, P = 0.002).
IL-17 concentrations (pg/mL)
20.00 40.00 60.00 80.00
2,500.00 2,000.00 1,500.00 1,000.00 500.00 0.00
Age (yr)
r = -0.037
Fig. 5. Simple scatter graph of ages and IL-17 concentrations. There was no correla- tion between age and IL-17 concentrations (P = 0.637, r = Pearson correlation coef- ficient).
The discovery of specific cells and cytokines with pivotal roles in inflammation can lead to the development of targeted thera- py to selectively inhibit critical steps, with minimal side effects.
Chauhan et al. (13) showed that in vivo blockade of IL-17 signif- icantly reduced the severity and progression of disease. Fortu- nately, eyes can be treated topically, thereby avoiding systemic toxicity. Because of this, recent excellent work on the role of Th- 17 cells in ocular surface disease could in the near future lead to the development of topical IL-17-targeted therapy that acts by interfering with local Th-17 cell activity.
Actually, the ocular surface has a Th-17 cell differentiation- friendly environment enriched with cytokines, including TGF- β1, IL-6, IL-23, and IL-1β induced by certain stimuli (14, 19, 20).
Zheng et al. (19) showed that corneal epithelial cells that are ex- posed to hyperosmotic, microbial, and inflammatory stimuli secreted cytokines promoting Th-17 cell differentiation. Our clin- ical data also suggest that Th-17 cells may be crucial in various ocular surface inflammations, especially in systemic inflamma- tory disease. The in vivo correlation of IL-17 with clinical scores of epithelial cell injury in the patients with systemic inflamma- tory disease strongly supports the results of Zheng’s in vitro ex- periments that damaged epithelial cells might enhance Th-17 cell differentiation (19). In addition, IL-17 is known to induce epithelial, stromal and immune cells to secrete proinflamma- tory cytokines such as IL-6, TNF-α, IL-1, and IL-8 (21) and dis- ruptive enzymes such as metalloproteinase-9 (14). A vicious cycle may develop in which a high IL-17 concentration is main- tained in an ocular environment with damaged epithelial cells that have already produced proinflammatory cytokines.
As mentioned in the introduction, autoimmune diseases such as Sjögren syndrome, rheumatoid arthritis, and systemic lupus erythematosus, which often involve the ocular surface, are re- lated to Th-17 cells. In fact, serum levels of IL-17 have been re- ported to correlate with both the activity and severity of these autoimmune diseases (22, 23). Subsequently, ocular involve- ment of IL-17 in these diseases may well be expected, which was clearly seen in the results of our study. Moreover, we found that serum IL-17 was also elevated in patients with GVHD, Sjögren syndrome- and rheumatoid arthritis-associated dry eye (24). In that previous study, the serum IL-17 level correlated significant- ly with the fluorescein staining score in these patients with sys- temic inflammatory disease, which corresponded well with this study showing correlation of tear IL-17 with clinical severity of the cornea. Therefore, on top of this previous evidence, the fact that correlation of the tear IL-17 with clinical severity strongly suggested that IL-17 might be involved in corneal surface inflam- mation in systemically autoimmune disease patients. Therefore, taking into consideration these previous reports including our study (22, 23), clinical correlation of tear IL-17 concentrations with ocular surface damage scores may be a valuable approach for assessing disease severity, providing the chance of bypass of
lacrimal biopsy in Sjögren’s syndrome.
Another interesting finding in this study was that chronic oc- ular GVHD showed a markedly high concentration of tear IL-17 compared with autoimmune and nonautoimmune ocular sur- face disorders. To the best of our knowledge, this is the first find- ing of IL-17 in ocular GVHD. Th-17 cells are known to mediate systemic GVHD (25, 26) although the exact role of Th-17 is still debated (27). The reason why ocular GVHD presented with high IL-17 values is still unclear. It can be presumed that it may be caused by direct invasion of host Th-17 cells as well as by dam- aged ocular epithelial cells inducing Th-17 cell differentiation from recruited naïve T cells. Further investigation is needed to elucidate the exact mechanisms for GVHD ocular IL-17.
While, the simple dry eye and MGD did not present significant correlation between the tear IL-17 and clinical severity, although high concentration of tear IL17 was observed compared with control. The reason why this disparity happened might be con- densing effect of tear as tear evaporated. That is, the condensed concentration of tear might include condensed concentration of IL-17. To clarify condensing effect of tear IL-17 due to tear evaporation, additional analysis for the abundant tear keeping protein like lactoferrin in normal condition as a control. The change of tear IL-17 would be analyzed after adjustment of lac- toferrin to exclude condensing effect. Although this study was limited that additional protein data could not be analyzed to adjust condensing effect due to small volume of the tear, our study is still worthy of notice to understand role of IL-17 in not only simple dry eye but also keratitis with systemic autoimmune disease. That is, our data suggested that tear IL-17 might be clin- ically relevant in systemic autoimmune disease patients to as- sess disease severity, while tear IL-17 might not be clinically rel- evant in simple evaporated type of dry eye.
On the other hand, the simple dry eye and MGD did not show severe clinical scores, in contrast dry eye with systemic disease presented wide range of clinical scores from mild type to very severe type. Simple dry eye or MGD seemed not to accompany severe corneal epithelial lesion. Considering that there is a cer- tain possibility that damaged cells per se would enhance IL-17 production by CD4 T cells (28), the explanation the other way around would be plausible. That is, the more cells are injured, the production of IL-17 appeared to be the more affected. That might be a reason why simple dry eye with rather low clinical scores did not show any relation with IL-17.
A limitation of this study is the relatively small number of pa- tients in the autoimmune-associated ocular surface disease groups. Another limitation is that we did not identify the cells secreting IL-17. Although the main source of IL-17 is Th-17 cells, in minor amounts it can also be produced by CD8+ T cells, γδT cells, natural killer T (NKT) cells, neutrophils, eosinophils, and macrophages (8, 29, 30). IL-17A is the prototypical member of the IL-17 family, which consists of six related proteins, from IL-
17A to IL-17F. Th-17 cells are the major source of IL-17A and F, while other cell populations express IL-17A to a lesser extent. As a result, assessment of IL-17A indicates that Th-17 cells are more likely to be the source cells than other cell populations. Conse- quently, our measurement of IL-17A can to some extent justify our assumption that Th-17 cells were the source cells but this correlation certainly needs further investigation. Another limi- tation was that we could not control unseen microscopic reflex tearing completely during the examination. However, when the gross reflex tearing was observed, we removed Schirmer strip, wait 10-20 min, and then re-applied it to exclude most gross re- flex tearing as possible as we could. In fact, one of the other lim- itation was that age was significantly younger in volunteering control group than the diseased group. Although we confirmed that age was not a confounding factor of IL-17 level using Pear- son correlation test, it could still act a little bit as a bias factor.
Nontheless, we still believe our findings may contribute to the further understanding of ocular surface disease pathogenesis regarding involvement of IL-17.
In conclusion, tear IL-17 is likely to be associated with the dry eye in the patients with systemic autoimmune diseases or sys- temic inflammatory disease by showing concentrations of IL-17 correlated well with clinical severity of the cornea. This suggests that Th-17 cells may be involved in the pathogenesis of ocular surface inflammatory disease. Clinically, the measurement of the concentration of IL-17 in tear may be applied as a valuable option to evaluate the ocular surface inflammatory severity quan- titatively in the patients with systemic inflammatory disease.
REFERENCES
1. Aggarwal S, Ghilardi N, Xie MH, de Sauvage FJ, Gurney AL. Interleukin-23 promotes a distinct CD4 T cell activation state characterized by the pro- duction of interleukin-17. J Biol Chem 2003; 278: 1910-4.
2. Harrington LE, Hatton RD, Mangan PR, Turner H, Murphy TL, Murphy KM, Weaver CT. Interleukin 17-producing CD4+ effector T cells develop via a lineage distinct from the T helper type 1 and 2 lineages. Nat Immu- nol 2005; 6: 1123-32.
3. Zheng Y, Danilenko DM, Valdez P, Kasman I, Eastham-Anderson J, Wu J, Ouyang W. Interleukin-22, a T(H)17 cytokine, mediates IL-23-induced dermal inflammation and acanthosis. Nature 2007; 445: 648-51.
4. Nakae S, Nambu A, Sudo K, Iwakura Y. Suppression of immune induc- tion of collagen-induced arthritis in IL-17-deficient mice. J Immunol 2003;
171: 6173-7.
5. Kebir H, Kreymborg K, Ifergan I, Dodelet-Devillers A, Cayrol R, Bernard M, Giuliani F, Arbour N, Becher B, Prat A. Human TH17 lymphocytes promote blood-brain barrier disruption and central nervous system in- flammation. Nat Med 2007; 13: 1173-5.
6. Yen D, Cheung J, Scheerens H, Poulet F, McClanahan T, McKenzie B, Kleinschek MA, Owyang A, Mattson J, Blumenschein W, Murphy E, Sathe M, Cua DJ, Kastelein RA, Rennick D. IL-23 is essential for T cell- mediated colitis and promotes inflammation via IL-17 and IL-6. J Clin
Invest 2006; 116: 1310-6.
7. Singh R, Aggarwal A, Misra R. Th1/Th17 cytokine profiles in patients with reactive arthritis/undifferentiated spondyloarthropathy. J Rheumatol 2007; 34: 2285-90.
8. Tesmer LA, Lundy SK, Sarkar S, Fox DA. Th17 cells in human disease.
Immunol Rev 2008; 223: 87-113.
9. Hashimoto T, Akiyama K, Kobayashi N, Mori A. Comparison of IL-17 production by helper T cells among atopic and nonatopic asthmatics and control subjects. Int Arch Allergy Immunol 2005; 137 Suppl 1: 51-4.
10. Burlingham WJ, Love RB, Jankowska-Gan E, Haynes LD, Xu Q, Bobadilla JL, Meyer KC, Hayney MS, Braun RK, Greenspan DS, Gopalakrishnan B, Cai J, Brand DD, Yoshida S, Cummings OW, Wilkes DS. IL-17-dependent cellular immunity to collagen type V predisposes to obliterative bronchi- olitis in human lung transplants. J Clin Invest 2007; 117: 3498-506.
11. Yoshimura T, Sonoda KH, Ohguro N, Ohsugi Y, Ishibashi T, Cua DJ, Ko- bayashi T, Yoshida H, Yoshimura A. Involvement of Th17 cells and the effect of anti-IL-6 therapy in autoimmune uveitis. Rheumatology (Ox- ford) 2009; 48: 347-54.
12. Amadi-Obi A, Yu CR, Liu X, Mahdi RM, Clarke GL, Nussenblatt RB, Gery I, Lee YS, Egwuagu CE. TH17 cells contribute to uveitis and scleritis and are expanded by IL-2 and inhibited by IL-27/STAT1. Nat Med 2007; 13:
711-8.
13. Chauhan SK, El Annan J, Ecoiffier T, Goyal S, Zhang Q, Saban DR, Dana R. Autoimmunity in dry eye is due to resistance of Th17 to Treg suppres- sion. J Immunol 2009; 182: 1247-52.
14. De Paiva CS, Chotikavanich S, Pangelinan SB, Pitcher JD 3rd, Fang B, Zheng X, Ma P, Farley WJ, Siemasko KF, Niederkorn JY, Stern ME, Li DQ, Pflugfelder SC. IL-17 disrupts corneal barrier following desiccating stress.
Mucosal Immunol 2009; 2: 243-53.
15. Molesworth-Kenyon SJ, Yin R, Oakes JE, Lausch RN. IL-17 receptor sig- naling influences virus-induced corneal inflammation. J Leukoc Biol 2008; 83: 401-8.
16. Shoji J, Kawaguchi A, Gotoh A, Inada N, Sawa M. Concentration of solu- ble interleukin-6 receptors in tears of allergic conjunctival disease patients.
Jpn J Ophthalmol 2007; 51: 332-7.
17. Kaido M, Goto E, Dogru M, Tsubota K. Punctal occlusion in the manage- ment of chronic Stevens-Johnson syndrome. Ophthalmology 2004; 111:
895-900.
18. Nichols KK, Mitchell GL, Zadnik K. The repeatability of clinical measure- ments of dry eye. Cornea 2004; 23: 272-85.
19. Zheng X, Bian F, Ma P, De Paiva CS, Stern M, Pflugfelder SC, Li DQ. In- duction of Th17 differentiation by corneal epithelial-derived cytokines. J Cell Physiol 2010; 222: 95-102.
20. Heo YJ, Park MK, Ju JH, Park KS, Cho ML, Kim HY. The effect of inflam- matory cytokines on the differentiation of Th17 cells in human peripher- al blood. J Korean Rheum Assoc 2009; 16: 133-43.
21. McGeachy MJ, Cua DJ. Th17 cell differentiation: the long and winding road. Immunity 2008; 28: 445-53.
22. Ziolkowska M, Koc A, Luszczykiewicz G, Ksiezopolska-Pietrzak K, Klim- czak E, Chwalinska-Sadowska H, Maslinski W. High levels of IL-17 in rheumatoid arthritis patients: IL-15 triggers in vitro IL-17 production via cyclosporin A-sensitive mechanism. J Immunol 2000; 164: 2832-8.
23. Katsifis GE, Rekka S, Moutsopoulos NM, Pillemer S, Wahl SM. Systemic and local interleukin-17 and linked cytokines associated with Sjögren’s syndrome immunopathogenesis. Am J Pathol 2009; 175: 1167-77.
24. Oh JY, Kim MK, Choi HJ, Ko JH, Kang EJ, Lee HJ, Wee WR, Lee JH. Inves- tigating the relationship between serum interleukin-17 levels and system- ic immune-mediated disease in patients with dry eye syndrome. Korean J Ophthalmol 2011; 25: 73-6.
25. Carlson MJ, West ML, Coghill JM, Panoskaltsis-Mortari A, Blazar BR, Serody JS. In vitro-differentiated TH17 cells mediate lethal acute graft- versus-host disease with severe cutaneous and pulmonary pathologic manifestations. Blood 2009; 113: 1365-74.
26. Kappel LW, Goldberg GL, King CG, Suh DY, Smith OM, Ligh C, Holland AM, Grubin J, Mark NM, Liu C, Iwakura Y, Heller G, van den Brink MR.
IL-17 contributes to CD4-mediated graft-versus-host disease. Blood 2009;
113: 945-52.
27. Iclozan C, Yu Y, Liu C, Liang Y, Yi T, Anasetti C, Yu XZ. T helper17 cells are sufficient but not necessary to induce acute graft-versus-host disease.
Biol Blood Marrow Transplant 2010; 16: 170-8.
28. Rao DA, Tracey KJ, Pober JS. IL-1alpha and IL-1beta are endogenous mediators linking cell injury to the adaptive alloimmune response. J Im- munol 2007; 179: 6536-46.
29. Gu Y, Yang J, Ouyang X, Liu W, Li H, Yang J, Bromberg J, Chen SH, May- er L, Unkeless JC, Xiong H. Interleukin 10 suppresses Th17 cytokines se- creted by macrophages and T cells. Eur J Immunol 2008; 38: 1807-13.
30. O’Brien RL, Roark CL, Born WK. IL-17-producing gammadelta T cells.
Eur J Immunol 2009; 39: 662-6.
AUTHOR SUMMARY
Interleukin-17 in Various Ocular Surface Inflammatory Diseases
Min Ho Kang, Mee Kum Kim, Hyun Joo Lee, Hyeon Il Lee, Won Ryang Wee and Jin Hak Lee
We measured concentration of interleukin (IL)-17 in patients’ tears and found that the tear IL-17 is increased in various ocular surface diseases. Interestingly, in the patients with systemic autoimmune diseases or with systemic inflammatory disease, concentrations of IL-17 are positively correlated with clinical severity of the cornea. Our results suggest that Th-17 cells are involved in the pathogenesis of ocular surface inflammatory disease. Clinically, the measurement of tear IL-17 could be applied as a parameter for quantitative evaluation of ocular surface inflammation.