Abstract :This study investigated potential drug-drug interactions (pDDIs) with warfarin with the aim of minimizing them, and to assess the acceptability of pharmaceutical interventions by the med- ical team and their impact on the international normalized ratio (INR). The retrospective, observa- tional study involved hospitalized patients (n=142) maintained on warfarin therapy with pDDI in Seoul National University Hospital from January 2012 to June 2012. Patients’demographics, medical history and medications used with daily warfarin doses were collected from electronic medical records. The pDDIs with warfarin were identified using the 9th ACCP guideline. Patients with pDDIs required lower warfarin doses than others (3.2±1.3 mg vs. 4.0±1.2 mg, p<0.05). There was a decreasing tendency for INR value in patients with pDDIs. The most common pDDIs with warfarin that resulted in increased anticoagulation were cardiovascular agents (71.8%), analgesics (16.4%), and
회원학술보고
Warfarin Therapy를 받는 환자에서 잠재적 약물상호작용 분석
문정연�, 박현희, 임정미, 이용화, 이혜숙, 한현주 서울대학교병원 약제부
Analysis of Potential Drug Drug Interaction with Warfarin Therapy in Hospitalized Patients
Jung Yeon Moon�, Hyeon Hee Park, Jeong Mi Im, Yong Hwa Lee, Hye Sook Lee, Hyeon Joo Hahn
Department of Pharmacy, Seoul National University Hospital, 101 Daehak-ro, Jongno-gu, Seoul, 110-744, Korea
투고일자 2015.3.4; 심사완료일자 2015.3.24; 게재확정일자 2015.4.10
�교신저자 문정연 Tel:02-2072-2594 E-mail:[email protected]
연구배경 및 목적
Warfarin은 정맥성 혈전 색전증의 예방 및 치료에 효과적이며, 인공심장 판막치환술을 받은 환자, 심방세 동, 판막 질환 혹은 급성심근경색 환자의 전신 색전증 을 예방하기 위하여 사용되고 있다.1)그러나 warfarin 과 다른 약물들과의 상호작용으로 인한 항응고 효과 조 절의 실패는 심각한 출혈 합병증이나 혈전색전증과 같 은 심각한 부작용을 야기할 수 있으므로 주의가 요구된
다.2),3)Warfarin의 항응고 효과와 연관된 출혈의 위험
성은 혈소판 응집 저해제, 위점막 미란을 일으킬 수 있 는 약물 등에 의해 증가되며4)비스테로이드성 소염진 통제 (NSAID) 또는 혈소판 응집 저해제와 warfarin을 동시에 복용하였을 때 warfarin을 단독 복용하는 것에
비해서 상부 위장관 출혈을 각각 2배, 3배 이상 증가시 키는 것으로 알려져 있다.4),5)
항응고 치료를 받는 대다수의 입원 환자들은 두 가지 이상의 만성질환을 가지므로 여러가지 약물을 동시에 복용하는 경우가 많아 대부분 잠재적인 약물상호작용 에 노출되어있다.6)-9)이는 warfarin을 처방받는 환자 에서 항응고 효과를 증가 또는 감소시킴으로써 출혈 합 병증 또는 혈전색전증의 위험을 높이는 결과를 초래할 수도 있다.10),11) 서울대학교병원 항응고 상담실(Anti Coagulation Service, ACS)에서는 외래 환자에 대해 서 잠재적 혹은 직접적 약물상호작용의 위험성을 낮추 고 안전한 항응고 치료가 이루어질 수 있도록 적절한 약사의 개입이 이루어지고 있지만, 입원 환자에 대해서 는 약물상호작용에 대한 면밀한 모니터링과 이에 대한 central nervous system drugs (6.3%). Concomitant cardiovascular and analgesic drugs reduced war- farin dose requirements, compared to patients not receiving either agent (2.5±0.8 mg vs. 4.0±1.2 mg, p<0.05). The difference of INR value was 0.36 between patients treated with cardiovascular drugs and the control group. The eight patients who received pDDIs experienced bleeding complications, and displayed a higher bleeding rate than the control group (5.6% vs. 3.0%). Major and moderate pDDIs with warfarin are very common in hospitalized patients and are associated with INR level out- side the therapeutic range. We conclude that concurrent use of pDDIs with warfarin is associated with increased risk of bleeding complication. Pharmaceutical interventions concerning the manage- ment of interactions by providing information to physicians can improve patient safety.
[Key words] Warfarin, pDDIs (potential drug-drug interactions), INR, Bleeding risk
적극적 개입이 부족한 실정이다.
따라서 본 연구에서는 서울대학교병원에서 warfarin 으로 항응고 치료를 받는 입원 환자들을 대상으로 warfarin과 동시에 투여되어 출혈의 위험성을 증가시 킬 수 있는 잠재적 상호작용(potential drug-drug interactions, pDDIs)이 보고된 약물의 처방빈도 및 임상적 결과를 평가하여12)약물상호작용으로 인해 출혈 합병증을 최소화하고, warfarin과 약물상호작용을 일 으킬 수 있는 처방에 대한 중재와 분석을 통해 안전한 약물요법의 발판을 마련하고 약사 개입의 필요성을 알 리고자 한다.
연구 방법
1. 연구 대상
2012년 1월부터 2012년 6월까지 총 6개월 동안 서울 대학교병원에 입원하여 ACS에 등록된 환자 중에서 warfarin therapy를 시작하는 환자 또는 최소 1년 이 상 warfarin을 복용하지 않았다가 다시 복용하는 환자 를 대상으로 후향적 연구를 진행하였다. 18세 미만, 입 원일수 5일 미만, warfarin 복용 기간이 5일 미만인 환자,6) PT prolongation으로 vitamin K 또는
FFP(Fresh frozen plasma)가 투여된 환자6), 의무기 록이 미비한 환자, 투약력이 불확실한 환자와 과도한 warfarin 투여로 인한 INR에 미치는 영향을 최소화하 기 위하여, 이전 유지 용량의 50%를 초과6)하여 war- farin이 투여된 환자는 연구 대상에서 제외하였다.
2. 연구 방법
대상 환자의 항응고 상담기록 및 전자의무기록지 (electronic medical record)를 통해 환자의 연령, 성 별, BMI(body mass index), 간 기능 검사, warfarin 적응증, 진료과, INR, 투약력(약품 이름, 1회 투여 용 량, 투여 횟수, 투약 일수)을 후향적으로 분석, 검토하 였다.
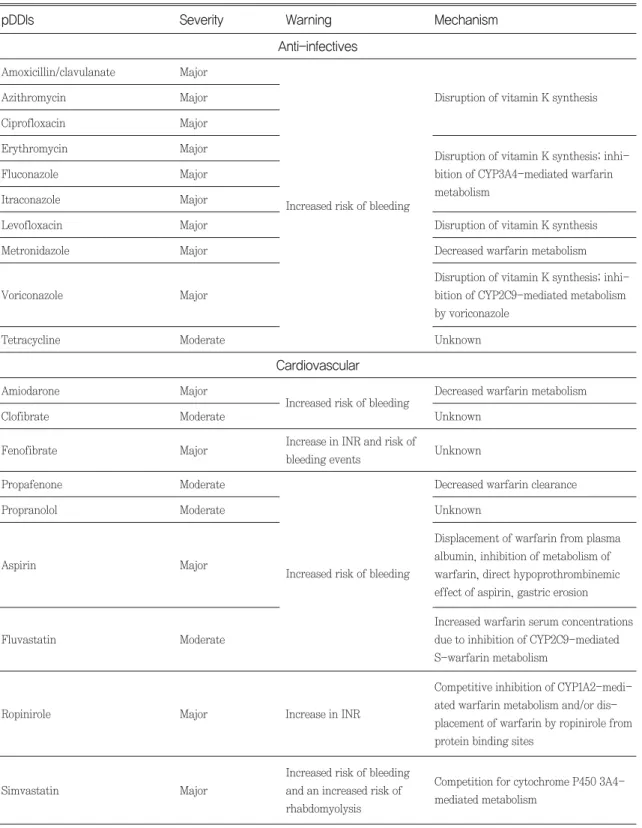
잠재적 약물상호작용은 동일한 날에 처방된 두 약물 을 대상으로 ACCP guideline 9th 13)을 활용하여 각각 highly probable, probable군에 속한 약물을 분류하 였고 MICROMEDEX(website, 2.0 version)를 활용 하여 상호작용의 심각도(severity)에 따라 major, moderate군으로 분류하였다(Table 1, 2).
두 정보원에 등재되지 않은 약물은 분석 대상에서 제 외하였으며 국소작용의 외용제, 수액제(normal saline, dextrose 등), 아미노산∙lipid제제 및 TPN
GI drugs CNS drugs
Analgesics, Antiinflammatories
Immunologies Cardiovascular
Level of
causation Anti-infectives
Cimetidine Omeprazole Citalopram
Entacapone Sertraline Phenylbutazone
Piroxicam Amiodarone
Clofibrate Fenofibrate Propafenone
Propranolol Highly probable Ciprofloxacin
Cotrimoxazole Erythromycin Fluconazole Itraconazole Metronidazole
Voriconazole
Table 1. List of potential drug drug interactions (pDDIs)
Fluvoxamine Phenytoin Acetaminophen
Aspirin Celecoxib Interferon Tramadol Aspirin
Fluvastatin Ropinirole Simvastatin Probable Amoxicillin/
Clavulanate Azithromycin
Levofloxacin Tetracycline
Mechanism Warning
Severity pDDIs
Anti-infectives
Cardiovascular Amoxicillin/clavulanate Major
Azithromycin Major
Ciprofloxacin Major
Amiodarone Major
Increased risk of bleeding Decreased warfarin metabolism
Clofibrate Moderate Unknown
Fenofibrate Major
Propafenone Moderate
Propranolol Moderate
Aspirin Major
Fluvastatin Moderate
Ropinirole Major Increase in INR
Simvastatin Major
Unknown
Decreased warfarin clearance Unknown
Displacement of warfarin from plasma albumin, inhibition of metabolism of warfarin, direct hypoprothrombinemic effect of aspirin, gastric erosion Increased warfarin serum concentrations due to inhibition of CYP2C9-mediated S-warfarin metabolism
Competitive inhibition of CYP1A2-medi- ated warfarin metabolism and/or dis- placement of warfarin by ropinirole from protein binding sites
Competition for cytochrome P450 3A4- mediated metabolism
Increased risk of bleeding and an increased risk of rhabdomyolysis
Increase in INR and risk of bleeding events
Increased risk of bleeding
Erythromycin Major
Fluconazole Major
Itraconazole Major
Levofloxacin Major
Metronidazole Major
Voriconazole Major
Tetracycline Moderate
Disruption of vitamin K synthesis
Disruption of vitamin K synthesis; inhi- bition of CYP3A4-mediated warfarin metabolism
Disruption of vitamin K synthesis; inhi- bition of CYP2C9-mediated metabolism by voriconazole
Unknown
Disruption of vitamin K synthesis Decreased warfarin metabolism Increased risk of bleeding
Table 2. Potential drug drug interactions(pDDIs) mechanism
Mechanism Warning
Severity pDDIs
Analgesics, Antiinflammatories, Immunologics
CNS drugs
GI drugs
Phenylbutazone Moderate
Citalopram Major
Sertraline Major Increased risk of bleeding Unknown
Fluvoxamine Major
Phenytoin Moderate
Cimetidine Moderate Increased risk of bleeding.
Omeprazole Moderate
Displacement of warfarin from protein binding sites, increased warfarin metabolism
Decreased warfarin metabolism Elevations of International
Normalized Ratio serum values and potentiation of anticoagulant effects Transient increased risk of bleeding when beginning phenytoin therapy but higher than expected war- farin dosage requirement during chronic therapy
Piroxicam Moderate
Acetaminophen Moderate
Celecoxib Major
Tramadol Moderate
Decreased warfarin metabolism, dis- placement of warfarin from protein binding sites
Decreased platelet aggregation, gastric erosion, and increased hypoprothrom- binemic response to warfarin
Competition for metabolism through cytochrome P450 2C9 enzymes
Unknown
Inhibition of warfarin metabolism or interference with clotting factor formation
Increased risk of bleeding
Increase in prothrombin time and an increased risk of bleeding.
(total parenteral nutrition)제제, 인슐린 제제, 임상 연구용 약물 또한 분석 대상에서 제외하였다. War- farin에 의한 항응고 효과는 warfarin therapy를 시 작한 시점부터 7일 이후 최대 효과를 나타낸다고 알려
져 있고,14),15) cytochrome P450(CYP)2C9 inhibitor 의 경우 2일 이상 warfarin과 동시에 투여되었을 때 충분한 상호작용을 나타내는 것으로 알려져 있다.16)따 라서 pDDIs 연관 약물 중에서 투약 일수가 7일 미만인
경우와(CYP2C9 inhibitor를 제외), 투약 일수 2일 미 만의 CYP2C9 inhibitor 투여 경우는 제외하였다.17) pDDIs 연관 약물 투여 기간 동안 대상 환자의 INR, warfarin 유지 용량, 출혈 합병증의 유무를 조사하여 pDDIs가 항응고 치료에 미치는 영향을 분석하였다.
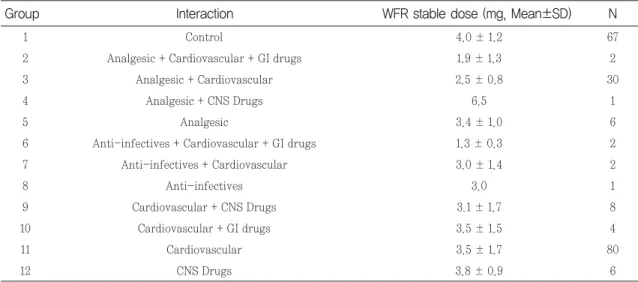
pDDIs 연관 약물의 종류에 따라 INR의 차이가 있는 지 분석하기 위해 pDDIs 연관 약물이 투여된 환자군을 ACCP guideline 9th 13)에서 제시한 기준을 근거로 11가 지 군으로 분류하였고, 대조군을 포함하여 다음과 같이 12개의 Group으로 나누어 분석하였다(Table 3).
본 연구의 통계 분석은 SPSS(Statistical Package for the Social Sciences) version 19.0을 이용하였고 모든 통계 분석의 결과는 p<0.05일 때 통계적으로 유 의하다고 정의하였다. 대조군과 pDDIs군에서 연령, 성 별, BMI, 간 기능 검사, warfarin 투여 용량, 전체 처 방 약물 개수, pDDIs 유도 약물 개수에 따른 warfarin 유지 용량과 INR의 변화가 있는지 알아보기 위하여 다 중회귀분석(단변량 분석에서 p<0.20인 변수들을 다변 량 분석으로 진행, 최종 p<0.05 유의6))을 이용하였고 범주형 자료에 대해서 Dummy variable을 이용하였 다. 세 집단 이상 평균을 비교하기 위하여 Kruskal- Wallis test을 이용하였고, 이에 대한 사후분석으로 Bonferroni 보정을 시행하였다.
연구 결과
1. 환자 특성
연구 기간 동안 서울대학교병원에서 warfarin therapy를 받은 입원 환자 즉, 대조군은 67명, war- N
Interaction Group
Table 3. Classifications according to the type of pDDIs
1 Control 67
2 Analgesic + Cardiovascular + GI drugs 2
3 Analgesic + Cardiovascular 30
4 Analgesic + CNS drugs 1
5 Analgesic 6
6 Anti-infectives + Cardiovascular + GI drugs 2 7 Anti-infectives + Cardiovascular 2
8 Anti-infectives 1
9 Cardiovascular + CNS drugs 8
10 Cardiovascular + GI drugs 4
11 Cardiovascular 80
12 CNS drugs 6
pDDIs (n=142) Control
(n=67) Characteristics
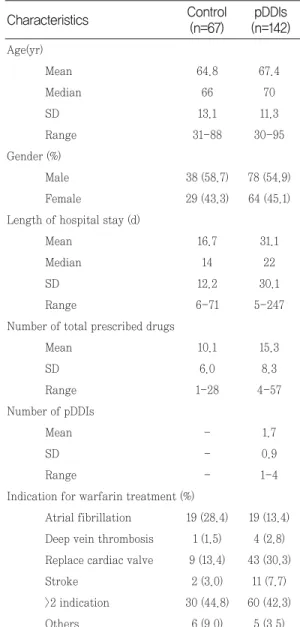
Table 4. Characteristics of Study Patients
Age(yr)
Mean 64.8 67.4
Median 66 70
SD 13.1 11.3
Range 31-88 30-95
Gender (%)
Male 38 (58.7) 78 (54.9)
Female 29 (43.3) 64 (45.1)
Length of hospital stay (d)
Mean 16.7 31.1
Median 14 22
SD 12.2 30.1
Range 6-71 5-247
Number of total prescribed drugs
Mean 10.1 15.3
SD 6.0 8.3
Range 1-28 4-57
Number of pDDIs
Mean - 1.7
SD - 0.9
Range - 1-4
Indication for warfarin treatment (%)
Atrial fibrillation 19 (28.4) 19 (13.4) Deep vein thrombosis 1 (1.5) 4 (2.8) Replace cardiac valve 9 (13.4) 43 (30.3)
Stroke 2 (3.0) 11 (7.7)
>2 indication 30 (44.8) 60 (42.3)
Others 6 (9.0) 5 (3.5)
farin과 pDDIs 연관 약물이 투여된 pDDIs군은 총 142명이었다. 환자 특성은 각각 다음 표와 같다(Table 4). pDDIs군의 평균 재원 기간은 대조군에 비해 약 2 배가량 길었다(31.1±30.1일 vs. 16.7±12.2일). 환자 별 전체 처방 약물 개수은 pDDIs군에서 대조군 보다 많았으며 (15.3±8.3 vs. 10.1±6.0), 이 때 환자별 pDDIs 연관 약물 개수는 평균 1.7±0.9개였다(range 1-4). Warfarin 적응증은 양쪽군 모두에서 심방세동 과, 인공심장 판막치환술 또는 심방세동과 심부정맥 혈 전증 등 2가지 이상의 적응증을 동시에 가진 비율이 가 장 많았다(42.3% vs. 44.8%).
2. 잠재적 약물 상호작용
(1) pDDIs 연관 약물 처방 분포 현황
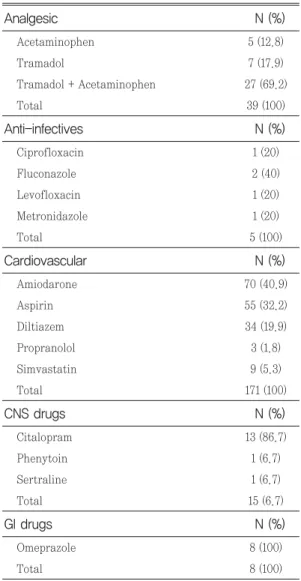
연구 결과 warfarin과의 pDDIs 분포는 다음 표와 같 았다(Table 5). 총 238건의 pDDIs 처방에서 car- diovascular 171건(71.8%), analgesics 39건(16.4%), CNS drugs 15건(6.3%), GI drugs 8건(3.4%), Anti- infectives 5건(2.1%) 순으로 많이 처방되었다 (Fig.
1). 가장 많이 처방된 cardiovascular 해당 약제는 amiodarone 70건(40.9%), aspirin 55건(32.2%), diltiazem 34건(19.9%) 순으로 처방 건수가 많았다.
Analgesics 해당 약제에서는 tramadol과 acetamin- ophen의 복합제제가 27건(69.2%)으로 가장 많이 처 방되었다.
(2) pDDIs 시 항응고 효과(INR) 및 warfarin 유지용량 조절 현황
대조군과 pDDIs군에서 연령, 성별, BMI, 간 기능 검 사, warfarin 투여 용량, 전체 처방 약물 개수, pDDIs 연관 약물 개수에 따른 INR이 증가 정도를 분석한 결 과 pDDIs 군에서만 전체 처방 약물의 개수 증가에 따 라 통계적으로 유의하게 INR이 증가하는 양상을 보였 으며 처방 약물 개수가 1개 증가시 INR은 0.015만큼 증가하였다(R2=0.075, y=0.469+0.015(전체 처방 약 물 개수)+0.093(warfarin 용량), p=0.024). 대조군과 pDDIs군의 warfarin 유지 용량은 Table 6에 제시하 였다. Warfarin 용량 조정에 의해 변화하는 INR 값을 보정한 상태에서 pDDIs군 중 Group 11(cardiovas- N (%)
Analgesic
Table 5. List of interacting drugs
Acetaminophen 5 (12.8)
Tramadol 7 (17.9)
Tramadol + Acetaminophen 27 (69.2)
Total 39 (100)
N (%) Anti-infectives
Ciprofloxacin 1 (20)
Fluconazole 2 (40)
Levofloxacin 1 (20)
Metronidazole 1 (20)
Total 5 (100)
N (%) Cardiovascular
Amiodarone 70 (40.9)
Aspirin 55 (32.2)
Diltiazem 34 (19.9)
Propranolol 3 (1.8)
Simvastatin 9 (5.3)
Total 171 (100)
N (%) CNS drugs
Citalopram 13 (86.7)
Phenytoin 1 (6.7)
Sertraline 1 (6.7)
Total 15 (6.7)
N (%) GI drugs
Omeprazole 8 (100)
Total 8 (100)
Fig. 1 Types of co-medications among patients on warfarin therapy
cular)에서 INR 최소값과 최대값의 차이는 0.36으로 통계적으로 유의한 결과를 보였다. Group 11의 처방 약물은 amiodarone 40건(38.8%), aspirin 35건 (34.0%), diltiazem 19건(18.4%), simvastatin 7건 (6.8%), propranolol 2건(1.9%) 순으로 많았다.
대조군에서는 전체 처방 약물 개수가 증가할수록 warfarin 유지용량이 감소하였으며(p=0.005) pDDIs 군에서는 전체 처방 약물 개수(p=0.012)와 pDDIs 약 물 개수(p=0.020)가 증가할수록 warfarin의 유지 용 량이 감소하였다. Warfarin의 평균 유지용량은 pDDIs군이 대조군보다 낮았다 (3.2±1.34 mg vs. 4.0
±1.2 mg, P<0.05). pDDIs군에서 전체 처방 약물 개 수가 1개 증가하고 pDDIs 약물 개수가 1개 증가 시 warfarin 투여 용량은 각각 0.039, 0.330만큼 감소하 였다(R2=0.099, y=4.389-0.039(전체 처방 약물 개 수)-0.330(pDDIs 연관 약물 개수)). pDDIs군 중에서 Group 3(analgesics + cardiovascular)과 대조군 사 이에 warfarin 유지 용량 간의 차이가 크게 나타났다 (2.5±0.8 mg vs. 4.0±1.2 mg, P<0.05)(Table 6).
Group 3에 해당하는 총 30명의 환자에서 acetamin- ophen + tramadol 복합제제와 amiodarone을 동시 에 처방받은 환자가 14명(46.7%)으로 가장 많았고, Group 3의 전체 처방 건수는 66건으로 analgesics 해 당 약제 중에서는 acetaminophen + tramadol 복합
제제가 25건(37.9%)으로 가장 많았고 cadiovascular 해당 약제 중에서는 amiodarone이 20건(30.3%)으로 가장 높은 비율로 처방되었다.
(3) 출혈 부작용
pDDIs군 142명 중 8명(5.6%)에서 출혈 합병증이 발 생하였고, 이들의 전체 처방 약물 수는 평균 21.5개 (range:15-31)였으며 pDDIs 연관 약물 개수는 2.3개 (range:1-3)였다. 출혈 합병증으로는 bloody sputum (n=1), hematuria(n=1), hematochezia(n=1), mele- na(n=1), hematoma(n=3), hematuria와 epistaxis 가 동시에 발생한(n=1) 경우로 나타났다. 두 가지 출혈 합병증을 가진 환자의 전체 처방 약물 수는 31개, pDDIs 연관 약물 개수는 3개로, 8명 중 약물의 처방수 가 가장 많았다. 대조군에서는 67명 중 2명(3.0%)에서 출혈 합병증이 발생하였고 각각의 전체 처방 개수는 11 개, 7개 였으며 hematoma와 소량의 nasal bleeding 이 있었다.
결론 및 고찰
Warfarin은 치료 범위가 좁은 약물로 작은 용량 변 화로도 혈전색전증 또는 출혈 합병증 등이 발생할 위험 성이 크며 약물상호작용으로 인해 항응고 효과가 변할
N WFR stable dose (mg, Mean±SD)
Group Interaction
Table 6. Warfarin stable dose between control and pDDIs group
1 Control 4.0 ± 1.2 67
2 Analgesic + Cardiovascular + GI drugs 1.9 ± 1.3 2
3 Analgesic + Cardiovascular 2.5 ± 0.8 30
4 Analgesic + CNS Drugs 6.5 1
5 Analgesic 3.4 ± 1.0 6
6 Anti-infectives + Cardiovascular + GI drugs 1.3 ± 0.3 2
7 Anti-infectives + Cardiovascular 3.0 ± 1.4 2
8 Anti-infectives 3.0 1
9 Cardiovascular + CNS Drugs 3.1 ± 1.7 8
10 Cardiovascular + GI drugs 3.5 ± 1.5 4
11 Cardiovascular 3.5 ± 1.7 80
12 CNS Drugs 3.8 ± 0.9 6
수 있으므로 주의 깊은 모니터링이 필요하다. 본 연구 에서는 2012년 1월부터 6월까지 서울대학교병원에서 warfarin을 복용하는 입원환자를 대상으로 ACCP guideline 9th 13)에 근거하여 잠재적 약물 상호작용과 연관된 약물 병용과 INR 증가 또는 warfarin 유지용 량 변화와의 상관성을 밝히고 출혈합병증의 발생 빈도 를 분석함으로써 약물 상호작용을 최소화 하기 위한 처 방중재의 필요성을 알리고 안전한 약물요법의 발판을 마련하고자 수행되었다.
서울대학교병원에서 warfarin therapy를 시작하는 입원환자에게 처방된 총 238건의 pDDIs 처방 분포는 cardiovascular 171건(71.8%), analgesics 39건 (16.4%), CNS drugs 15건(6.3%), GI drugs 8건 (3.4%), Anti-infectives 5건(2.1%)이였고 이중 car- diovascular 약물로는 amiodarone 70건(40.9%), aspirin 55건(32.2%), diltiazem 34건(19.9%) 순으로 처방 건수가 많았다. Hauta-Aho M 등의 연구에서는 warfarin으로 항응고 치료를 받는 환자의 약 48%가 잠재적 상호작용이 있는 약물(Potential drug-drug interactions, pDDIs)에 노출된다고 보고하였다.6),18) Castro T.A. 등과 Kotirum S. 등의 연구 결과에서는 warfarin therapy를 받는 환자 중 84%가 적어도 하 나 이상의 pDDIs에 노출된다고 보고 하였다.6),19)본 연 구결과 서울대학교병원에서 연구기간 중 warfarin therapy를 시작하는 입원환자의 평균 pDDIs 개수는 1.7개였으며 대조군에 비해 약 2배 가량 긴 재원일수를 보였다. Castro T.A. 등의 연구에 따르면 재원일수의 증가는 INR의 증가에 영향을 주는 독립적인 risk fac- tor이며(p=0.01) 그 자체로 환자의 comorbidity를 증 가시키며 더 많은 약물에 노출되게 함으로써 INR을 증 가시키는 부정적인 결과를 초래할 수 있다고 밝힌 바 있다.6)본 연구에서도 재원일수가 더 길었던 pDDIs군 의 전체 처방 약물 개수가 대조군에 비해 더 많았던 것 으로 확인되었으며 이로인해 INR의 증가로 이어져 출 혈의 합병증이 증가한 것으로 추정할 수 있었다.
대조군에서는 연령, 성별, BMI, 간 기능 검사, 전체 처방 약물 개수에 따라 INR이 증가하지 않았지만, pDDIs군에서는 전체 처방 약물 개수 증가시 INR이 유 의하게 증가하였다. Cardiovascular군에 속하는 amiodarone, aspirin, diltiazem 등은 적응증상 필수
적으로 복용해야 하는 약물임에도 warfarin과의 약물 상호작용에 크게 관여한 것으로 조사되어 ACS시 주의 깊은 INR monitoring을 통해 warfarin 용량 조절이 이루어져야 함을 알 수 있었고, 의료진에게 항응고 효 과를 변화시킬 수 있는 약물에 대한 정보제공이 필요함 을 알 수 있었다. 대조군에서는 전체 처방 약물 개수가 증가할수록 pDDIs군에서는 전체 처방 약물 개수와 pDDIs 연관 약물 개수가 증가할수록 warfarin의 유지 용량이 감소하였고 특히 analgesics와 cardiovas- cular 약제가 동시에 투여된 pDDIs군에서 대조군보다 평균 warfarin 유지 용량이 적었다(4.0±1.2 mg vs.
2.5±0.8 mg, P<0.05). 한편, 전체 pDDIs군 중 car- diovascular군을 제외한 나머지 군에서 유의하게 INR 의 증가가 관찰되지 않은 이유는 의료진이 daily INR monitoring 결과에 따라 warfarin의 용량을 적절하 게 변경했기 때문이라고 생각된다.
복용하는 pDDIs 연관 약물의 수가 많을수록 INR의 증가로 인해 출혈 발생 빈도가 증가하게 되며 Gasse 등의 연구에 따르면 4개 이상의 약물을 복용하면서 warfarin therapy를 받는 환자들은 1개 이상의 약물 상호작용으로 인한 출혈 합병증이 빈번히 발행하기 때 문에 그렇지 않은 환자들에 비해 출혈 발생 빈도가 3.4 배 더 높다고 보고하였다.6),20)이번 연구에서도 pDDIs 군 142명 중 8명(5.6%)에서 출혈 합병증이 발생하였 고, 대조군은 67명 중 2명(3.0%)에서 출혈이 발생하여 pDDIs군에서의 출혈 발생율이 약 2배 더 높았다. 따라 서 잠재적 약물 상호작용으로 인한 출혈의 위험이 증가 할 수 있음을 알 수 있었고 이에 대한 면밀한 모니터링 이 필요할 것으로 생각된다.
본 연구의 한계점으로는 대상 환자의 수가 제한적이 고 ACS 상담기록지 분석을 통한 후향적 조사방법으로 진행되어 누락된 약물상호작용이나 부작용 보고가 있 을 수 있으며 병용약물 이외에 항응고 효과 변화에 영 향을 주는 요인이 완전히 배제되었는지의 여부를 확실 하게 알 수 없다는 점이 있다.
치료영역이 좁고 여러 가지 요인에 의해 항응고효과 가 변화할 수 있는 warfarin을 안전하고 효과적으로 환자에게 적용하기 위해서는 close monitoring이 필 요하다. 항응고 효과를 변화시키는 여러 요인 중 pDDIs는 INR 상승을 유발하는 요인 중 하나로 알려져
있다. Warfarin 적응증 이외에도 다른 여러 가지 병존 질환을 가지고 있는 입원환자에서는 warfarin과 관련 된 pDDIs가 빈번히 발생할 수 있고, 이로 인해 항응고 효과가 치료범위를 벗어난 경우 출혈의 합병증으로 연 결될 가능성이 높다.21)-23)다양한 약물을 복용하는 입원 환자군에서는 안정적으로 INR을 유지하기 어렵기 때 문에, 약물 상호 작용에 대한 연구는 매우 중요하며 warfarin 복용에 안전하고 효과적으로 처방하기 위해 서 의료진의 약물 사용에 대한 정확한 인식 및 교육이 필요하며 약사는 의료진에게 pDDIs에 대해 체계적인 정보를 제공하고 적절한 처방 중재를 통해 환자에게 안 전한 약물요법이 적용될 수 있도록 기여해야 할 것으로 사료된다.
참고문헌
1) Hirsh J., James E., Anderson D. R., Poller L., Bussey H., Ansell J., Deykin D. : Oral anti- coagulants: mechanism of action, clinical effectiveness, and optimal therapeutic range.
Chest, 119(1 suppl), 8S-21S (2001)
2) Harder S., Thurmann P. : Clinically impor- tant drug interactions with anticoagulants.
An update. Clin Pharmacokinet, 30(6), 416- 444 (1996)
3) Wells P. S., Holbrook A. M., Crowther N.R., Hirsh J. : Interactions of warfarin with drugs and food. Ann Intern Med, 121(9), 676- 683 (1994)
4) Hauta-Aho M., Tirkkonen T., Vahlberg T., Laine K. : The effect of drug interactions on bleeding risk associated with warfarin ther- apy in hospitalized patients, Annals of Medicine, 41(8), 619-628 (2009)
5) Egger S. S., Drewe J., Schlienger R. G. : Potential drug-drug interactions in the medication of medical patients at hospital discharge, Eur J Clin Pharmacol, 58(11), 773- 778 (2003)
6) Castro T. A., Heineck I. : Interventions to
improve anticoagulation with warfarin, Ther Drug Monit, 34(2), 209-216 (2012)
7) Teklay G., Shiferaw N., Legesse B., Bekele M. L. : Drug-drug interactions and risk of bleeding among inpatients on warfarin thetapy: a prospective observational study.
Thromb J, 17(20), 12-20 (2014)
8) Vonbach P., Dubied A., Beer J. H. : Recognition and management of potential drug-drug interactions in patients on inter- nal medicine wards. Eur J Clin Pharmacol, 63(11), 1075-1083 (2007)
9) Seymour R. M., Routledge P. A .: Important drug-drug interactions in the elderly. Drugs Aging, 12 (6), 485-494 (1998)
10) Schulman S., Beyth R. J., Kearon C. : Hemorrhagic complications of anticoagu- lant and thrombolytic treatment: American College of Chest Physicians evidence-based clinical practice guidelines (8th edition).
Chest, 133(6 Suppl), 257S-298S (2008) 11) Levine M. N., Raskob G., Beyth R. J. :
Hemorrhagic complications of anticoagulant treatment: the seventh ACCP conference on antithrombotic and thrombolytic therapy.
Chest, 126(3 Suppl), 287S-310S (2004) 12) Wiedermann C. J., Stockner I. : Warfarin-
induced bleeding complications-clinical presentation and therapeutic options.
Thromb Res, 122 (suppl 2), S13-S18. (2008) 13) Ageno W., Gallus A. S., Wittkowsky A.,
Crowther M., Hylek E. M., Palareti G. : Oral Anticoagulant Therapy, American College of Chest, Physicians evidence-based clinical practice guidelines (9th edition), Chest, 141 (2 Suppl), e44S-e88S (2012)
14) Mosher D. F. : Cecil Textbook of Medicine, 18th ed. WB Saunders, Philadelphia. 1040- 1058 (1988)
15) Majerus P. W., Broze Jr G. J., Miletich J. P.
: Good man & Gilman’s The Pharmacological Basis of Therapeutics 1467-1488 (1996) 16) Johnson S. G., Rogers K., Delate T., Witt D.
M. : Outcomes associated with combined antiplatelet and anticoagulant therapy.
Chest, 13(4), 948-954 (2008)
17) Laine K., Forsstrom J., Gronroos P., Irjala K., Kailajarvi M., Scheinin M. : Frequency and Clinical Outcome of Potentially Harmful Drug Metabolic Interactions in Patients Hospitalized on Internal and Pulmonary Medicine Wards: Focus on Warfarin and Cisapride. Ther Drug Monit, 22(5), 503-509 (2000)
18) Hauta-Aho M., Tirkkonen T., Vahlberg T., Laine K. : The effect of drug interactions on bleeding risk associated with warfarin therapy in hospitalized patients. Ann Med, 41(8), 619-628 (2009)
19) Kotirum S., Chaiyakunapruk N., Jampa- chaisri K. : Utilization review of concomi- tant use of potentially interacting drugs in Thai patients using warfarin therapy.
Pharmacoepidemiol Drug Saf, 16(2), 216- 222 (2007)
20) Gasse C., Hollowell J., Meier C. R. : Drug interactions and risk of acute bleeding leading to hospitalisation or death in patients with chronic atrial fibrillation treated with warfarin. Thromb Haemost, 94 : 537-543 (2005)
21) Ansell J., Hirsh J., Dalen J., Bussey H., Anderson D., Poller L., Jacobson A., Deylin D., Matchar D. : Managing oral anticoagu- lant therapy. Chest, 119(1 suppl), 22S-38S (2001)
22) Brigden M. L., Kay C., Le A., Graydon C., McLeod B. : Audit of the frequency and clinical response to excessive oral antico- agulation in an out-patient population. Am
J Hematol, 59 (1), 22-7 (1998)
23) Lousberg T. R., Witt D. M., Beall D. G., Carter B. L., Malone D. C. : Evaluation of excessive anticoagulation in a group model health maintenance organization. Arch Intern Med, 158(5), 528-534 (1998)